
Abstract
Introduction
Consensus regarding optimal glucagon dosing for management or diagnosis of neonatal/infant hypoglycemia has not been established.
Objective
To investigate glycemic effects of glucagon dosed ≤0.2 mg/kg (Gnlow) vs. >0.2 mg/kg (Gnhigh) in neonatal/infant hypoglycemia.
Study design
Retrospective, observational, cohort study.
Results
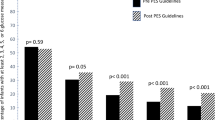
Glucagon administration at any dose resulted in 75/77 (97.4%) samples meeting criteria for normoglycemia (plasma glucose >60 mg/dL), and plasma glucose increases of >30 mg/dL occurred in 74.2% vs. 63% (NS) of samples in the Gnlow and Gnhigh groups, respectively. Despite equivalent glucagon dosing, there was a trend toward smaller (<2500 g) patients achieving post-glucagon plasma glucose increases of >30 mg/dL less often than their bigger (≥2500 g) counterparts (60% vs. 74.1%, NS).
Conclusions
Glucagon is highly effective in raising plasma glucose levels in neonatal/infant hypoglycemia. No differences in glycemic effects were noted between either dosing regimen. However, glycemic effects may be diminished in lower weight patients.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others


References
McGowan J. Neonatal hypoglycemia. Pediatr Rev 1999;20:e6–e15.
Adamkin DH. Neonatal hypoglycemia. Semin Fetal Neonatal Med. 2017;22:36–41.
Gregory KE. New approaches to care of the infant with hypoglycemia. J Perinat Neonatal Nurs. 2016;34:284–7.
Committee on Fetus and Newborn, Adamkin DH. Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics 2011;127:575–9.
Thornton PS, Stanley CA, De Leon DD, Harris D, Haymond MW, Hussain K, et al. Recommendations from the Pediatric Endocrine Society for evaluation and management of persistent hypoglycemia in neonates, infants, and children. J Pediatr 2015;167:238–45.
Glucagon. Lexi-Drugs. Lexicomp. Riverwoods: Wolters Kluwer Health, Inc.; 2019. http://online.lexi.com. Accessed 12 Dec 2019.
Stanley CA, Rozance PJ, Thornton PS, De Leon DD, Harris D, Haymond MW, et al. Re-evaluating “transitional neonatal hypoglycemia”: Mechanism and implications for management. J Pediatr 2015;166:1520–5.e1.
Finegold DN, Stanley CA, Baker L. Glycemic response to glucagon during fasting hypoglycemia: an aid in the diagnosis of hyperinsulinism. J Pediatr 1980;96:257–9.
Lord K, De Leon DD. Hyperinsulinism in the neonate. Clin Perinatol 2018;45:61–74.
Palladino AA, Stanley CA. A specialized team approach to diagnosis and medical versus surgical treatment of infants with congenital hyperinsulinism. Semin Pediatr Surg 2011;20:32–37.
Blanco M, Khan O, Stanley K, Hageman JR, Greeley SAW. Hyperinsulinism in a neonate. Pediatr Ann 2014;43:e50–e60.
De Leon DD, Stanley CA. Mechanisms of disease: advances in diagnosis and treatment of hyperinsulinism in neonates. Nat Clin Pr Endocrinol Metab. 2007;3:57–68.
Miralles RE, Lodha A, Perlman M, Moore AM. Experience with intravenous glucagon infusions as a treatment for resistant neonatal hypoglycemia. Arch Pediatr Adolesc Med. 2002;156:999–1004.
Carter PE, Lloyd DJ, Duffty P. Glucagon for hypoglycaemia in infants small for gestational age. Arch Dis Child. 1988;63:1264–6.
Belik J, Musey J, Trussell R. Continuous infusion of glucagon induces severe hyponatremia and thrombocytopenia in a premature neonate. Pediatrics 2001;107:595–7.
Froehlich JM, Daenzer M, von Weymarn C, Erturk SM, Zollikofer CL, Patak MA. Aperistaltic effect of hyoscine n-butylbromide versus glucagon on the small bowel assessed by magnetic resonance imaging. Eur Radiol 2009;19:1387–93.
Mitsios JV, Ashby LA, Haverstick DM, Bruns DE, Scott MG. Analytic evaluation of a new glucose meter system in 15 different critical care settings. J Diabetes Sci Technol. 2013;7:1282–7.
Kermani SK, Khatony A, Jalali R, Rezaei M, Abdi A. Accuracy and precision of measured blood sugar values by three glucometers compared to the standard technique. J Clin Diagn Res. 2017;11:OC05–OC08.
Roche Diagnostic. Accu-Chek Inform II blood glucose monitoring system operator’s manual, Ver. 6. 2017 Retrieved from http://diagnostic.roche.com/content/dam/diagnostics/us/en/products/a/accu-chek-inform-ii/toolkit/08424705001-01.pdf. Accessed 12 Dec 2019.
Blum D, Dodion J, Loeb H, Wilkin P, Hubinont PO. Studies on hypoglycaemia in small-for-dates newborns. Arch Dis Child. 1969;44:304–10.
Le Dune MA. Response to glucagon in small-for-dates hypoglycaemic and non-hypoglycaemic newborn infants. Arch Dis Child. 1972;47:754–9.
Cornblath M, Levin EY, Marquetti E. Studies of carbohydrate metabolism in the newborn. II: the effect of glucagon on the concentration of sugar in capillary blood of the newborn infant. Pediatrics 1958;21:885–92.
Linarelli LG, Bobik C, Bobik J, Drash AL, Rubin HM. The effect of glucagon on adenosine 3′,5′-monophosphate (cyclic AMP), glucose, insulin and growth hormone in the full term newborn and children. J Clin Endocrinol Metab. 1974;39:411–7.
Mehta A, Wootton R, Cheng KN, Penfold P, Halliday D, Stacey TE. Effect of diazoxide or glucagon on hepatic glucose production rate during extreme neonatal hypoglycaemia. Arch Dis Child. 1987;62:924–30.
Hawdon JM, Aynsley-Green A, Ward Platt MP. Neonatal blood glucose concentrations: metabolic effects of intravenous glucagon and intragastric medium chain triglyceride. Arch Dis Child. 1993;68:255–61.
van Kempen AAMW, Ackermans MT, Endert E, Kok JH, Sauerwein HP. Glucose production in response to glucagon is comparable in preterm AGA and SGA infants. Clin Nutr 2005;24:727–36.
Thompson-Branch A, Havranek T. Neonatal hypoglycemia. Pediatr Rev 2017;38:147–57.
Funding
The project was funded with no specific support
Author information
Authors and Affiliations
Contributions
R.G. collected and analyzed the data, drafted the initial manuscript, and approved the final manuscript. M.T. analyzed the data, revised the manuscript, and approved the final manuscript. D.J.K. analyzed the data, drafted the initial manuscript, and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Godin, R., Taboada, M. & Kahn, D.J. A comparison of the glycemic effects of glucagon using two dose ranges in neonates and infants with hypoglycemia. J Perinatol 40, 1841–1848 (2020). https://doi.org/10.1038/s41372-020-00770-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-020-00770-4
This article is cited by
-
The use of intramuscular glucagon to prevent IV glucose infusion in early neonatal hypoglycemia
Journal of Perinatology (2021)
