
Abstract
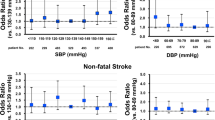
Clinical practice guidelines for patients with diabetes recommend using blood pressure (BP) and atherosclerotic cardiovascular disease (ASCVD) risk to guide antihypertensive treatment. While this approach directs treatment to patients who should receive a large ASCVD risk reduction, its effect on other outcomes is uncertain. The aim of this study was to assess the contributions of systolic blood pressure level (SBP) and predicted 10-year ASCVD risk using Pooled Cohort risk equations to the prediction of major macrovascular disease, death and major microvascular disease in patients with diabetes. Data came from 7426 individuals with type 2 diabetes (T2D) without macrovascular disease at baseline in the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial. The risk for major macrovascular events and death increased progressively across ASCVD risk categories. Compared to participants with 10-year predicted ASCVD risk <20% and SBP <130 mmHg, the hazard ratios (HRs) (95% confidence intervals (CIs)) associated with SBP ≥150 mmHg and 10-year predicted ASCVD risk <20%, 20–34% and ≥35% were 1.01 (0.58, 1.77), 1.90 (1.28, 2.84) and 2.82 (1.98, 4.01) for major macrovascular disease, respectively, and 0.83 (0.42, 1.62), 1.79 (1.13, 2.82) and 3.29 (2.22, 4.88) for death, respectively. The risk for major microvascular disease increased with BP regardless of ASCVD risk; HRs for SBP ≥150 mmHg and 10-year predicted ASCVD risk <20%, 20–34% and ≥35% vs. ASCVD risk <20% and SBP <130 mmHg were 1.52 (1.08,2.13), 1.47 (1.10, 1.96) and 1.23 (0.94, 1.60), respectively. ASCVD risk in addition to SBP improved the estimation of major macrovascular events and death but not major microvascular events among individuals with T2D.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

Data availability
Restrictions apply to the availability of these data, which were used by agreement of the ADVANCE steering committee for the current study, and so are not publicly available. R code for the c-statistic and NRI calculations is given in the Supplementary Material.
References
American Diabetes Association. 10. Cardiovascular disease and risk management: standards of medical care in diabetes-2020. Diabetes Care. 2020;43:S111–34.
Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 International Society of Hypertension global hypertension practice guidelines. J Hypertens. 2020;38:982–1004.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens. 2018;36:1953–2041.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:1269–324.
Goff DC Jr, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB Sr, Gibbons R, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2935–59.
ADVANCE Management Committee. Rationale and design of the ADVANCE study: a randomised trial of blood pressure lowering and intensive glucose control in high-risk individuals with type 2 diabetes mellitus. Action in Diabetes and Vascular Disease: PreterAx and DiamicroN Modified-Release Controlled Evaluation. J Hypertens. 2001;19:S21–8.
Patel A, MacMahon S, Chalmers J, Neal B, Woodward M, Billot L, et al. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet. 2007;370:829–40.
Patel A, MacMahon S, Chalmers J, Neal B, Billot L, Woodward M, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560–72.
Rahman F, McEvoy JW, Ohkuma T, Marre M, Hamet P, Harrap S, et al. Effects of blood pressure lowering on clinical outcomes according to baseline blood pressure and cardiovascular risk in patients with type 2 diabetes mellitus. Hypertension. 2019;73:1291–9.
Woodward M. Epidemiology: study design and data analysis. 3rd ed. Boca Raton: CRC Press, Taylor & Francis Group; 2014. p. 832.
Zheng Y, Parast L, Cai T, Brown M. Evaluating incremental values from new predictors with net reclassification improvement in survival analysis. Lifetime Data Anal. 2013;19:350–70.
Jackson R, Lawes CM, Bennett DA, Milne RJ, Rodgers A. Treatment with drugs to lower blood pressure and blood cholesterol based on an individual’s absolute cardiovascular risk. Lancet. 2005;365:434–41.
Alderman MH. Blood pressure management: individualized treatment based on absolute risk and the potential for benefit. Ann Intern Med. 1993;119:329–35.
Karmali KN, Lloyd-Jones DM, van der Leeuw J, Goff DC Jr, Yusuf S, Zanchetti A, et al. Blood pressure-lowering treatment strategies based on cardiovascular risk versus blood pressure: a meta-analysis of individual participant data. PLoS Med. 2018;15:e1002538.
Blood Pressure Lowering Treatment Trialists' Collaboration. Blood pressure-lowering treatment based on cardiovascular risk: a meta-analysis of individual patient data. Lancet. 2014;384:591–8.
Karmali KN, Ning H, Goff DC, Lloyd-Jones DM. Identifying individuals at risk for cardiovascular events across the spectrum of blood pressure levels. J Am Heart Assoc. 2015;4:e002126.
Herrett E, Gadd S, Jackson R, Bhaskaran K, Williamson E, van Staa T, et al. Eligibility and subsequent burden of cardiovascular disease of four strategies for blood pressure-lowering treatment: a retrospective cohort study. Lancet. 2019;394:663–71.
Whelton SP, McEvoy JW, Shaw L, Psaty BM, Lima JAC, Budoff M, et al. Association of normal systolic blood pressure level with cardiovascular disease in the absence of risk factors. JAMA Cardiol. 2020;5:1011–8.
Muntner P, Colantonio LD, Cushman M, Goff DC Jr, Howard G, Howard VJ, et al. Validation of the atherosclerotic cardiovascular disease Pooled Cohort risk equations. JAMA. 2014;311:1406–15.
Bertoluci MC, Rocha VZ. Cardiovascular risk assessment in patients with diabetes. Diabetol Metab Syndr. 2017;9:25.
Mohammedi K, Woodward M, Marre M, Colagiuri S, Cooper M, Harrap S, et al. Comparative effects of microvascular and macrovascular disease on the risk of major outcomes in patients with type 2 diabetes. Cardiovasc Diabetol. 2017;16:95.
Tangri N, Grams ME, Levey AS, Coresh J, Appel LJ, Astor BC, et al. Multinational assessment of accuracy of equations for predicting risk of kidney failure: a meta-analysis. JAMA. 2016;315:164–74.
Mora S, Wenger NK, Cook NR, Liu J, Howard BV, Limacher MC, et al. Evaluation of the pooled cohort risk equations for cardiovascular risk prediction in a multiethnic cohort from the women’s health initiative. JAMA Intern Med. 2018;178:1231–40.
Morris AA, Ko YA, Hutcheson SH, Quyyumi A. Race/ethnic and sex differences in the association of atherosclerotic cardiovascular disease risk and healthy lifestyle behaviors. J Am Heart Assoc. 2018;7:e008250. .
Peters SAE, Muntner P, Woodward M. Sex differences in the prevalence of, and trends in, cardiovascular risk factors, treatment, and control in the United States, 2001 to 2016. Circulation. 2019;139:1025–35.
Woodward M. Cardiovascular disease and the female disadvantage. Int J Environ Res Public Health. 2019;16:1165.
Lloyd-Jones DM, Braun LT, Ndumele CE, Smith SC, Sperling LS, Virani SS, et al. Use of risk assessment tools to guide decision-making in the primary prevention of atherosclerotic cardiovascular disease. J Am Coll Cardiol. 2019;73:3153–67.
Chalmers J, Arima H. Importance of blood pressure lowering in type 2 diabetes: focus on ADVANCE. J Cardiovasc Pharm. 2010;55:340–7.
Funding
The ADVANCE trial (ClinicalTrials.gov registration no. NCT00145925) was funded by grants from the National Health and Medical Research Council (NHMRC) of Australia (project grant ID 211086 and programme grant IDs 358395 and 571281) and from Servier. The study sponsors had no role in the design of the study, data collection, data analysis, data interpretation or the writing of the manuscript. Study data were not made available to the sponsors. The Management Committee, whose membership did not include any sponsor representatives, had final responsibility for the decision to submit for publication.
Author information
Authors and Affiliations
Contributions
MW and JC conceived, designed and acquired the ADVANCE trial data. JC and JM conceived this study. KH conducted the statistical analyses, with advice from MW. KH wrote the initial drafts of the manuscript. All authors were involved in data interpretation. Drafts were revised for important scientific content by all authors. All authors gave final approval of the version to be published. KH is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Competing interests
JC reports research grants from the NHMRC and from Servier for the ADVANCE trial and ADVANCE-ON post-trial follow-up, and honoraria for speaking about these studies at scientific meetings and support from NHMRC Programme Grant (APP1149987). MW reports consultancy fees from Amgen, Freeline and Kyowa Kirin and is supported by NHMRC grants APP1149987 and APP1174120. JM does not report any conflict of interest and reports attendance at the European Society of Hypertension, Barcelona, paid by ISORDIA (Switzerland) in 2018.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Harris, K., Muntner, P., Woodward, M. et al. Clinical outcomes by atherosclerotic cardiovascular disease risk score and blood pressure level in high risk individuals with type 2 diabetes. J Hum Hypertens 37, 181–188 (2023). https://doi.org/10.1038/s41371-022-00661-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41371-022-00661-5
This article is cited by
-
Metabolomics signature of cardiovascular disease in patients with diabetes, a narrative review
Journal of Diabetes & Metabolic Disorders (2023)
