
Abstract
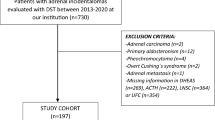
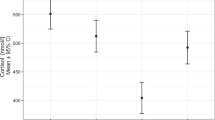
There are limited data regarding the frequency of hypertension in nonfunctioning adrenal incidentaloma (NFAI). Our objectives were to investigate rates of hypertension and resistant hypertension in NFAI patients, and compare them to a control group without adrenal adenoma. We also aimed to evaluate the relationship between cortisol levels after 1 mg-dexamethasone suppression test (DST) and hypertension in NFAI patients. We selected 40 patients with NFAI and 40 control patients over the age of 18 without adrenal lesions on abdominal imaging. Data regarding hypertension, resistant hypertension, number, and type of antihypertensive drugs were collected from each subject. Blood samples for C-reactive protein (CRP), plasma adrenocorticotropic hormone (ACTH) and dehydroepiandrosterone sulfate (DHEA-S) were also collected from the patients. Age, gender, race, smoking status, menopause status and BMI were comparable between patient and control groups. Patients with NFAI had a higher frequency of hypertension (72.5 vs. 47.5%; p = 0.04), resistant hypertension (37.9 vs. 11.1%; p = 0.04) and took three or more antihypertensive drugs (33.3 vs. 5.2%; p = 0.002) when compared to the controls, respectively. NFAI patients with hypertension had higher mean cortisol levels after 1 mg-DST when compared to NFAI patients without hypertension (1.3 ± 0.3 vs. 1.0 ± 0.4; p = 0.03, respectively). We found a negative correlation between cortisol levels after 1 mg-DST DHEA-S levels (r = −0.61; p < 0.001) and a positive correlation with CRP levels (r = 0.44; p = 0.02). In conclusion, NFAI patients presented a higher frequency of hypertension, resistant hypertension and used more antihypertensive medications when compared to the control group. We found an association between hypertension in NFAI patients and cortisol levels after 1 mg-DST.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2016;175:G1–34.
Morelli V, Reimondo G, Giordano R, Della Casa S, Policola C, Palmieri S, et al. Long-term follow-up in adrenal incidentalomas: an Italian multicenter study. J Clin Endocrinol Metab. 2014;99:827–34.
Di Dalmazi G, Vicennati V, Garelli S, Casadio E, Rinaldi E, Giampalma E, et al. Cardiovascular events and mortality in patients with adrenal incidentalomas that are either non-secreting or associated with intermediate phenotype or subclinical Cushing’s syndrome: a 15-year retrospective study.Lancet Diabetes Endocrinol. 2014;2:396–405
Peppa M, Koliaki C, Raptis SA. Adrenal incidentalomas and cardiometabolic morbidity: an emerging association with serious clinical implications. J Intern Med. 2010;268:555–66.
Tuna MM, Imga NN, Dogan BA, Yilmaz FM, Topcuoglu C, Akbaba G et al. Non-functioning adrenal incidentalomas are associated with higher hypertension prevalence and higher risk of atherosclerosis. J Endocrinol Invest 2014;37:765–8.
Androulakis II, Kaltsas GA, Kollias GE, Markou AC, Gouli AK, Thomas DA, et al. Patients with apparently nonfunctioning adrenal incidentalomas may be at increased cardiovascular risk due to excessive cortisol secretion. J Clin Endocrinol Metab. 2014;99:2754–62.
Comlekci A, Yener S, Ertilav S, Secil M, Akinci B, Demir T, et al. Adrenal incidentaloma, clinical, metabolic, follow-up aspects: single centre experience. Endocrine. 2010;37:40–6.
Yener S, Genc S, Akinci B, Secil M, Demir T, Comlekci A, et al. Carotid intima media thickness is increased and associated with morning cortisol in subjects with non-functioning adrenal incidentaloma. Endocrine. 2009;35:365–70.
Yener S, Comlekci A, Akinci B, Secil M, Demir T, Ertilav S, et al. Non-functioning adrenal incidentalomas are associated with elevated D-dimer levels. J Endocrinol Invest. 2009;32:338–43.
Yener S, Comlekci A, Yuksel F, Sevinc A, Ertilav S, Yesil S. Traditional and novel cardiovascular risk factors in non-functioning adrenal adenomas. Eur J Intern Med. 2012;23:83–7.
Jones DW, Hall JE. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure and evidence from new hypertension trials. Hypertension. 2004;43:1–3.
Beaglehole R, Bonita R. Global public health: a scorecard. Lancet. 2008;372:1988–96.
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies C. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–13.
Boland GW, Blake MA, Hahn PF, Mayo-Smith WW. Incidental adrenal lesions: principles, techniques, and algorithms for imaging characterization. Radiology. 2008;249:756–75.
Lenders JW, Duh QY, Eisenhofer G, Gimenez-Roqueplo AP, Grebe SK, Murad MH, et al. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014;99:1915–42.
Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2016;101:1889–916.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507–20.
Tuna MM, Imga NN, Dogan BA, Yilmaz FM, Topcuoglu C, Akbaba G, et al. Non-functioning adrenal incidentalomas are associated with higher hypertension prevalence and higher risk of atherosclerosis. J Endocrinol Invest. 2014;37:765–8.
Debono M, Bradburn M, Bull M, Harrison B, Ross RJ, Newell-Price J. Cortisol as a marker for increased mortality in patients with incidental adrenocortical adenomas. J Clin Endocrinol Metabol. 2014;99:4462–70.
Lopez D, Luque-Fernandez MA, Steele A, Adler GK, Turchin A, Vaidya A. “Nonfunctional” adrenal tumors and the risk for incident diabetes and cardiovascular outcomes: a cohort study. Ann Intern Med. 2016;165:533–42.
Di Dalmazi G, Vicennati V, Rinaldi E, Morselli-Labate AM, Giampalma E, Mosconi C, et al. Progressively increased patterns of subclinical cortisol hypersecretion in adrenal incidentalomas differently predict major metabolic and cardiovascular outcomes: a large cross-sectional study. Eur J Endocrinol. 2012;166:669–77.
Yilmaz H, Tutuncu NB, Sahin M. Two-year follow-up of thirty-two non-functional benign adrenal incidentalomas. J Endocrinol Invest. 2009;32:913–6.
Pereira M, Lunet N, Azevedo A, Barros H. Differences in prevalence, awareness, treatment and control of hypertension between developing and developed countries. J Hypertens. 2009;27:963–75.
Piaditis GP, Kaltsas GA, Androulakis II, Gouli A, Makras P, Papadogias D, et al. High prevalence of autonomous cortisol and aldosterone secretion from adrenal adenomas. Clin Endocrinol (Oxf). 2009;71:772–8.
Seppel T, Schlaghecke R. Augmented 17 alpha-hydroxyprogesterone response to ACTH stimulation as evidence of decreased 21-hydroxylase activity in patients with incidentally discovered adrenal tumours (‘incidentalomas’). Clin Endocrinol (Oxf). 1994;41:445–51.
Harman E, Karadeniz M, Biray C, Zengi A, Cetinkalp S, Ozgen AG, et al. The relation of adiponectin and tumor necrosis factor alpha levels between endothelial nitric oxide synthase, angiotensin-converting enzyme, transforming growth factor beta, and tumor necrosis factor alpha gene polymorphism in adrenal incidentalomas. J Endocrinol Invest. 2009;32:881–8.
Ermetici F, Malavazos AE, Corbetta S, Morricone L, Dall’Asta C, Corsi MM, et al. Adipokine levels and cardiovascular risk in patients with adrenal incidentaloma. Metabolism. 2007;56:686–92.
Arlt W, Biehl M, Taylor AE, Hahner S, Libe R, Hughes BA, et al. Urine steroid metabolomics as a biomarker tool for detecting malignancy in adrenal tumors. J Clin Endocrinol Metab. 2011;96:3775–84.
Bancos I, Alahdab F, Crowley RK, Chortis V, Delivanis DA, Erickson D, et al. Therapy of endocrine disease: improvement of cardiovascular risk factors after adrenalectomy in patients with adrenal tumors and subclinical Cushing’s syndrome: a systematic review and meta-analysis. Eur J Endocrinol. 2016;175:R283–95.
Acknowledgements
This study was made possible thanks to grants from the Research Support Foundation of the State of Rio de Janeiro, (FAPERJ) and the Brazilian National Council for Scientific and Technological Development (CNPq) to LVN.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Arruda, M., Mello Ribeiro Cavalari, E., Pessoa de Paula, M. et al. The presence of nonfunctioning adrenal incidentalomas increases arterial hypertension frequency and severity, and is associated with cortisol levels after dexamethasone suppression test. J Hum Hypertens 32, 3–11 (2018). https://doi.org/10.1038/s41371-017-0011-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41371-017-0011-4
This article is cited by
-
Mild autonomous cortisol secretion: pathophysiology, comorbidities and management approaches
Nature Reviews Endocrinology (2024)
-
Adrenalectomy improves blood pressure control in nonfunctioning adrenal incidentalomas and glycemic and lipid control in patients with autonomous cortisol secretion
Endocrine (2022)
-
Adrenal incidentaloma as a novel independent predictive factor for periodontitis
Journal of Endocrinological Investigation (2021)
-
Cortisol level after dexamethasone suppression test in patients with non-functioning adrenal incidentaloma is positively associated with the duration of reactive hyperemia response on microvascular bed
Journal of Endocrinological Investigation (2021)
-
Evaluation of body composition using dual-energy X-ray absorptiometry in patients with non-functioning adrenal incidentalomas and an intermediate phenotype: Is there an association with metabolic syndrome?
Journal of Endocrinological Investigation (2019)
