
Abstract
In preterm infants intraventricular hemorrhage occurs predominantly within the perinatal period, which may be due to a “lost autoregulation” of cerebral blood flow (CBF). In this study, perinatal autoregulation dynamics were investigated in high risk preterm infants by cross-spectral analysis (CSA), which is a statistical tool in the analysis of time series. In 15 ventilated preterm infants of 25-32 gestational weeks, a total number of 30 records were made between 24 and 96 h of life. Doppler-derived CBF velocity (CBFv), used as a quantitative measure for CBF, and direct mean arterial blood pressure (MABP) were measured continuously for 10 min. The spectral power of low frequency (LF, 0.02-0.2 Hz) oscillations in CBFv and MABP was quantified by spectral analysis. From the results of CSA, a LF phaseshift between the CBFv and MABP LF oscillations was calculated in each record. Within the study group, the LF spectral power of CBFv and MABP was initially low and increased significantly until 96 h of life. The LF phase-shift was about 0 ° at 24 h and increased significantly to 55 ° at 96 h of life. The initially low LF spectral power of CBFv and MABP may indicate a perinatal depression of autonomic nervous centers, which are thought to control LF oscillations of vital parameters. In the light of a high pass filter model for autoregulation, the initially low LF phase-shift may indicate an initially impaired autoregulation, which supports the “lost autoregulation” hypothesis.
Similar content being viewed by others

Main
Especially immature preterm infants of less than 33 gw are at risk for cerebral lesions such as IVH(1–3). Typically, IVH occurs between some hours and some days of life, but often not immediately after birth or beyond the age of 1 wk(1, 2). So there is evidence that not only pre- and intranatal, but also postnatal, events such as fluctuations in MABP might trigger IVH, particularly in case of a “lost autoregulation”(1). Two main aspects of CBF regulation are: 1) central regulation of CBF. Vital parameters such as body temperature, blood pressure, and heart rate show LF oscillations, which are thought to be mediated by the autonomic nervous system(4–6). Used as a quantitative measure for CBF(7–9), CBFv also showed LF oscillation, which seems to be a normal phenomenon in healthy preterm neonates, especially during the perinatal period(10–12). Their absence may indicate severe illness(12), so that LF oscillations may reflect the state of central regulation. The amount of LF oscillations can be quantified by simple spectral analysis. 2) Autoregulation of CBF describes the capacity of the cerebral resistance vessels to balance out disturbing changes in MABP(13). Autoregulation can be subdivided into a “static” and “dynamic” component(14). “Static autoregulation” represents the well known sigmoid steady-state relation between CBF and MABP(13). “Dynamic autoregulation” describes the dynamic response to a MABP stimulus, e.g. how fast CBF is balanced out after a step decrease in MABP. Both static and dynamic autoregulation measurements yield similar results(14), so that analysis of the dynamic component may be sufficient to quantify the capacity for autoregulation.
In general, a regulation system can be analyzed by step, sinusoidal, or more complex types of stimuli(15). A step MABP decrease leads to a corresponding step decrease in CBFv. If autoregulation is active, CBFv increases again within a few seconds, whereas it stays decreased if autoregulation is impaired(14, 16). A sinusoidal MABP stimulus at 0.05 or 0.10 Hz leads to a sinusoidal CBFv response, oscillating “in front” of MABP at a positive phase-shift(17, 18). A high phase-shift was found in healthy individuals, whereas a low phase-shift occurred in patients with cerebrovascular disease(18). In the mentioned studies(14, 16–18) the CBFv responses to step and sinusoidal MABP stimuli were analyzed in the time domain by methods that are limited to the specific type of MABP stimulus. The results indicated that cerebral autoregulation has properties of a high pass filter system(18). If so, complex MABP stimuli will lead to corresponding complex CBFv responses. In this case, CSA has advantages, because CSA is independent of the type of MABP stimulus. CSA measures the temporal relationship between two time series over a range of frequencies(15). Further details of CSA are given in the “Methods” section. In this study, natural LF oscillations of MABP were regarded as complex stimuli to the autoregulation system. Referring to the results of other studies(17, 18), the cross-spectral phase-shift between CBFv and MABP LF oscillations was used to quantify the individual capacity for autoregulation. The results were compared with the independent method of Panerai et al.(19).
This study is part of an ongoing observational study on autoregulation of the preterm neonate. Considerations about “critical closing pressure” as a comprehensive model of cerebral autoregulation have been published elsewhere(20). The aim of this observational study was to investigate whether in high risk preterm infants of less than 33 wk of gestation there are any abnormalities in both mentioned regulation phenomena within the perinatal period, i.e. within the period prone to IVH.
METHODS
Patients. Fifteen ventilated preterm infants of 25-32 gw were studied (Table 1), if they had indwelling arterial lines and were clinically stable enough within the first 4 d of life. Patients with perinatal risk factors prone to IVH were intentionally not excluded from the study. Birth weight ranged from 575 to 1730 (median 1065) g. All patients were sedated with 5-10 mg/kg/d phenobarbital throughout the study. One patient (26 gw, 575 g) died after fourth degree IVH, the other survived and showed IVH of grade zero or one.
Measurements. In each patient Doppler-derived CBFv and direct ABP was recorded one to three times within the first 4 d of life. This was done in the narrow time window between clinical stabilization and withdrawal of the umbilical or radial arterial line, which had been inserted for clinical reasons at birth. Direct ABP was digitally sampled for 10 min(21). Simultaneously, the enveloping CBFv in an internal carotid artery was traced by a transfontanellar miniaturized range-gated Doppler device(22, 23). Its acoustic power output was below the recommended limits of the American Institute for Ultrasound in Medicine(24). The study was approved by the local Ethical Committee, and informed parental consent was obtained.
Statistics. For data processing and statistical analysis, DBase IV (Ashton Tate), Statgraphics Plus 7.0 (Statistical Graphics Corporation), and proprietary programs were used.
Preprocessing. Within the digitized CBFv and ABP curves, each value was replaced by the time-average of its corresponding cardiac pulse. This algorithm removed the systolic-diastolic pulsatility from the data. The modified data were time-averaged at intervals of exactly 1 s, resulting in an equidistant time series of 600-s duration. The mean of the complete 10 min was defined as the individual “baseline.” Each CBFv and MABP time series was transformed from absolute (cm/s or mm Hg) units to percentage deviation from its baseline. Before spectral analysis, a first order trend was removed(25), and each first and last 10% of the time series was cosine tapered to minimize spectral leakage(15, 25). The data were digitally band pass-filtered(26) between 0.02 and 0.2 Hz to extract the LF component.
Simple spectral analysis and CSA. By fast Fourier transform, the preprocessed CBFv and MABP time series were transformed from the time domain to the frequency domain, resulting in fast Fourier transform spectra(15, 25). By CSA the temporal relationship between the CBFv and MABP time series was examined over the LF range. CSA was carried out by multiplication of the CBFv and MABP fast Fourier transform spectra(15, 25). To receive statistically robust spectral estimates, the spectra were smoothed by a seven-point simple moving average(15). In each record, CSA resulted in a cross-power spectrum, a coherence spectrum, and a phase-shift spectrum. At each specific frequency, the cross-spectral power quantifies the amount of spectral power, which CBFv and MABP have in common. The cross-spectral power is high if both CBFv and MABP show marked coherent oscillations. The cross-spectral power is low if the oscillations of CBFv and MABP are small or not coherent. The cross-spectral coherence estimates the strength of temporal relationship between CBFv and MABP at each frequency. A coherence of zero indicates that the CBFv and MABP oscillations are not related to each other. The closer the coherence is to 1, the stronger the CBFv and MABP oscillations are related(15). The temporal relationship of the CBFv and MABP oscillations is quantified by the phase-shift. A phase-shift of 0 ° indicates parallel oscillations which are “in phase,” whereas, e.g. a phase-shift of 45 ° indicates that CBFv oscillates “in front” of MABP.
Calculation of individual LF spectral parameters. To quantify the tendencies within the individual LF spectra, five LF spectral parameters were calculated. Their equations are given in “Appendix A.”
MABP-SPLF and CBFv-SPLF measure the total spectral power of the MABP and CBFv LF oscillations. Their square roots equal the “coefficient of variation” within the preprocessed time series and are used to measure the individual amount of LF oscillations. Phase-shiftLF estimates the average phase-shift between the CBFv and MABP oscillations within the LF band. Its calculation accounts for the fact that the CBFv and MABP oscillations have different cross-spectral powers at different frequencies. The 95% confidence intervals for phase-shiftLF were estimated by computer simulation (Table 2). The coherenceLF is to some extent comparable to a correlation coefficient and measures the strength of temporal relationship between CBFv and MABP over the LF range. In contrast to a correlation coefficient, the coherenceLF does not neglect that the CBFv and MABP time series may have a strong, but somewhat delayed, temporal relationship. Significance limits for coherenceLF were determined by CSA of 10 000 random time series (Table 2). The log-center-freqLF marks the center of the LF cross-power spectrum, if the frequency axis is logarithmic.
Within the study group, the relation between the LF spectral parameters and postnatal age, postconceptional age, and birth weight was investigated by linear regression analysis. Statistical significance was assessed at p < 0.05. The prerequisites for application of linear regression analysis including approximately normal distribution for at least one variable were assessed according to Shott(27).
Comparison of phase-shiftLF with an independent measure for autoregulation. In this study phase-shiftLF is used as a measure for dynamic autoregulation. The results for phase-shiftLF were compared with the regression method of Panerai et al.(19). In this method the original CBFv and MABP traces are split into contiguous 8-s intervals. The averages of those intervals are calculated and used to determine the “regression slope” between CBFv and MABP. Significant regression slopes above the “critical slope” of 1.5%/mm Hg indicate an impaired autoregulation(19). Only records with a MABP range of at least 5 mm Hg are analyzed.
RESULTS
Illustrative patient. Two records of patient 7 (29 gw, birth weight 1430 g) illustrate how LF oscillations of CBFv and MABP and their temporal relationship can change during the perinatal period.
LF oscillations of CBFv and MABP (Fig. 1). At 64 h of life, MABP and CBFv oscillated around baselines of 38.4 mm Hg and 15.4 cm/s (Fig. 1A). The LF components (0.02-0.2 Hz) of those oscillations become more prominent after trend removal and band-pass filtering (Fig. 1B). The amount of spectral power is quantified by the square root of CBFv-BFv-SPLF = 1.31% and the square root of MABP-SPLF = 1.14%. The power spectra of CBFv and MABP show a relatively similar, but not completely identical distribution (Fig. 1C).

Simultaneous tracings of MABP and CBFv (record 19). (A) Unfiltered time series, where LF oscillations are already visible. (B) Preprocessed time series after band-pass filtering (0.02-0.2 Hz) and cosine tapering. MABP and CBFv are given as percentage deviation from their individual baselines. (C) The corresponding power spectra show relatively similar distributions for CBFv and MABP.
Cross-spectral analysis of LF oscillations (Fig. 2). At 48 h of life, the LF oscillations of CBFv and MABP are nearly in phase and show a strong alignment (Fig. 2A). This visual impression is confirmed by a phase-shiftLF of -2.6 ° (Fig. 2B) and a coherenceLF of 0.71, which indicates a significant temporal relationship between CBFv and MABP (p < 0.001, according to Table 2). At 64 h of life, CBFv tends to oscillate in front of MABP (Fig. 2C) with a positive phase-shiftLF of 66.2 ° (Fig. 2D). The temporal relationship between CBFv and MABP seems to be weak at 64 h (Fig. 2C), but this visual impression is rejected by a coherenceLF of 0.66 (p < 0.001), which is not much less than the coherenceLF of 0.71 at 48 h.

Course of LF phase-shift between CBFv and MABP from 48 to 64 postnatal hours in an illustrative patient (29 gw, birth weight 1430 g). (A) At 48 h: the LF oscillations of CBFv and MABP seem to be nearly in phase. (B) At 48 h: CSA confirms this impression by a phase-shiftLF of -2.6 °, which is nearly 0 °. (C) At 64 h: now CBFv tends to oscillate in front of the MABP curve. (D) At 64 h: this is confirmed by a corresponding positive phase-shiftLF of 66.2 °. The phase-shift trace in B and D is shown only at frequencies with a statistically significant temporal relationship between CBFv and MABP, i.e. at frequencies where the coherence was significantly (p < 0.05) different from zero(25). If CBFv and MABP would have a random temporal relationship, the phase trace would show only some spots that are dispersed in a random fashion. However, there are long connected parts within the phase trace. This indicates a strong temporal relationship between CBFv and MABP, which is confirmed by a significant coherenceLF of 0.71 at 48 h and 0.66 at 64 h (p < 0.001). The asterisk (*) marks the LF logarithmic center frequency (log-center-freqLF) of the cross-power spectrum.
Study group (30 records in 15 patients, Fig. 3). All records showed a coherenceLF of more than 0.59. According to Table 2, this indicated a significant temporal relationship between CBFv and MABP (p < 0.001), and a 95% confidence interval of not more than ±10 ° for phase-shiftLF.

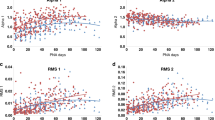
Correlation between LF spectral parameters and postnatal age (30 records). The graphs show the regression line, inner confidence limits, and outer prediction limits. (A and B) The amount of LF oscillation in MABP and CBFv was quantified by sqrt(MABP-SPLF) and sqrt(CBFv-SPLF). Within the study group, the amount of MABP and CBFv LF oscillation increased significantly within the first four postnatal days (p < 0.05). (C) Within the study group, the phase-shiftLF (LF phase-shift between CBFv and MABP) increased significantly from about 0 ° toward about 55 ° during the first days of life. (D) In all records, the coherenceLF was above 0.59, which indicated a significant temporal relationship between CBFv and MABP (p < 0.001, Table 2). Within the study group, the coherenceLF showed no significant tendency in regard to postnatal age (p > 0.05).
Within the study group the amount of LF oscillation in CBFv and MABP, measured by the square root of CBFv-SPLF and MABP-SPLF, increased significantly with postnatal age (Fig. 3,A and B). Phase-shiftLF increased significantly from about 0 ° at 24 h of life toward 55 ° at 96 h (Fig. 3C), whereas coherenceLF showed no significant correlation with postnatal age (Fig. 3D). No significant correlations were found in respect to postconceptional age or birth weight (Table 3). Those results remained unchanged, when correcting for the statistical influence of log-center-freqLF by multiple regression analysis.
In this study phase-shiftLF is used as a measure for dynamic autoregulation. For comparison, the independent regression slope method of Panerai et al.(19) was applied to the 18 records, which exceeded the minimum MABP range of 5 mm Hg. Within those 18 records, the regression slope was initially high and decreased significantly with postnatal age (p < 0.05), whereas there was no significant correlation with postconceptional age or birth weight (Table 3). This correspondence between regression slope and phase-shiftLF is explained by the highly significant inverse correlation between both measures (r = -0.65, p < 0.01). Their regression line is given by phase-shiftLF = -11.8 °·mm Hg/%·regression slope + 34.6 °. On this regression line, the critical slope 1.5%/mm Hg corresponds to a phase-shiftLF of 16.9 °.
DISCUSSION
CBF and CBFv. Many articles have dealt with the theme whether Doppler-derived CBFv is a quantitative measure for CBF or not. The main question is whether the investigated vessel's diameter remains nearly constant, e.g. during Pco2 changes. Different methods have shown significant correlations between CBFv and CBF, if measured within the great cerebral arteries(7–9). Therefore, the following discussion does not always differentiate between the terms CBF and CBFv.
Central regulation of CBF and MABP. In humans, several vital parameters show cycling oscillations, which are thought to be mediated by the autonomic nervous system(4–6). Typical cycling frequencies are 0.01-0.15 Hz(28) or 0.05 Hz(4, 12) for thermoregulation, and 0.02-0.20 Hz for heart rate(4). Typical CBFv cycling frequencies in preterm and term newborns range from 0.025 to 0.083 Hz(10–12). At least within the first weeks of life, LF CBFv cycling seems to be a normal phenomenon in healthy preterm infants(10, 12). As in adults, its absence may indicate cerebral pathology(12, 29). Within the study group, the amount of LF oscillations in CBFv and MABP was initially low, and increased significantly within the first four postnatal days. If LF oscillations of CBFv and MABP are mediated by the autonomic nervous system, this finding may indicate an initial perinatal depression of the cerebral regulation centres.
Dynamic autoregulation of CBF (Fig. 4). Autoregulation of CBF describes the capacity of the cerebral resistance vessels to balance out disturbing changes in MABP(13). This autoregulation of CBF can be absent after traumatic events such as prolonged cerebral hypoxemia(13). In this case CBF changes passively with MABP, whether there is a step increase in MABP (Fig. 4A) or a sinusoidal change in MABP (Fig. 4B). If autoregulation is active, a step change in MABP causes an initial step change in CBF (Fig. 4C)(16). However, the cerebral resistance vessels respond actively by adapting their resistance within a few seconds(16). According to Ohm's law (flow = pressure/resistance), CBF returns to baseline within a few seconds. This dynamic response of CBF to a MABP stimulus is the “dynamic” component of autoregulation. It yields similar results as measurements of the “static” component of autoregulation(14), so that analysis of the dynamic component may be sufficient to quantify the capacity for autoregulation.

Simple high pass filter model for cerebral autoregulation (see “Appendix B”) (with flow = pressure/resistance according to Ohm's law). (A) Absent autoregulation, step pressure increase; the resistance vessels are not active, so that flow changes passively with pressure. (B) Absent autoregulation, sinusoidal pressure oscillations; the resistance vessels are not active, so that flow changes passively in phase (phase-shift φ = 0 °) with pressure. (C) Active autoregulation, step pressure increase; the resistance increases to restore the original pressure/resistance relation. According to Ohm's law, flow is initially forced to a step increase, but returns to its baseline within seconds. In this example, the time constant TC of the regulation system is 5 s. The half-maximal CBF response time is T1/2 = TC·ln(2) = 3.47 s. (D) Active autoregulation, sinusoidal pressure oscillations; the flow oscillates in front of MABP at a positive phase-shift (φ = +51.9 °). The resistance oscillates after MABP at a negative phase-shift. Although not immediately obvious, the underlying autoregulation system is the same as in C (see Fig. 5 and “Discussion”).
Dynamic autoregulation analysis by step and sinusoidal MABP changes. A step decrease in MABP was used as standard stimulus to the autoregulation system(14, 16). It causes an initial step decrease in CBFv(14, 16). The cerebral resistance vessels need some time to adapt their resistance, with the regulative aim to bring CBFv back to its baseline. The half-maximal CBFv response time T1/2 (Fig. 4C) may be used to quantify the speed of dynamic autoregulation. A short T1/2 indicates a fast autoregulation, whereas a long T1/2 indicates a slow or impaired autoregulation(16). Dynamic autoregulation was also analyzed by nearly sinusoidal MABP oscillations at low frequencies of 0.05 and 0.10 Hz(17, 18). As a typical CBF response, CBFv oscillates in front of MABP at a positive phase-shift(17, 18). The principle is shown in Figure 4D. Healthy individuals showed a positive phase-shift between the CBFv and MABP oscillations of about 51.7 ± 35.1 °(18), whereas patients with cerebrovascular disease and suspected impairment of autoregulation showed a low phase-shift of about 26.8 ± 13.5 °(18). Other studies investigated the characteristic responses of the cerebral autoregulation system to sinusoidal and step MABP stimuli at different levels of Pco2(16, 17). Their results are summarized in Table 4, which also offers a hypothetical explanation for the finding, that acute hypo- and hypercapnia can alter the speed of dynamic autoregulation.
There is yet no “gold-standard” for the investigation of dynamic autoregulation. So far, the step stimulus method seems to be the most accepted method. This may be due to the fact that it presents a well defined MABP stimulus with a comprehensible CBFv response (Fig. 4C). In contrast, the CBFv response to a sinusoidal MABP stimulus is difficult to understand (Fig. 4D). It seems to measure something that is completely different from the CBFv response to a step change in MABP. It is quite difficult to accept that CBFv oscillates at a positive phase shift in front of MABP, because this seems to violate the principle of causality. By intuition one would expect that CBFv has to oscillate behind MABP, if MABP is the stimulus. However, the changes in CBFv are the result of autoregulation, whereas the adaptation of the cerebrovascular resistance is the active process(13). The cerebrovascular resistance oscillates after MABP (Fig. 4D), and, therefore, the principle of causality is not violated. Although not immediately obvious, the positive phase-shift between CBFv and MABP in Figure 4D is closely linked with the exponential CBFv response in Figure 4C. This is visualized in Figure 5 by approximation from a step MABP stimulus to a sinusoidal MABP stimulus. The phase-shift method seems to describe the same basic autoregulation mechanism, only in a different way.

Stepwise approximation from a step to a sinusoidal pressure change. Although not immediately obvious, the underlying regulation mechanism in Figure 4D is the same as in Figure 4C. This is visualized by stepwise approximation from a single pressure step (A) toward a sinusoidal pressure curve (F). The resistance is always reacting on a new change in pressure, with the regulative aim to bring flow back to baseline. This cannot be achieved completely, because the resistance vessels are not foresighted and need some time for contraction or dilation.
Dynamic autoregulation analysis by complex MABP changes. There is no evidence that autoregulation is active only at the low frequencies 0.05 and 0.10 Hz, which were used in the previously cited studies(17, 18). Additionally, there is no evidence that autoregulation is active only during induced MABP changes. Therefore, we consider natural LF oscillations of MABP as an alternative stimulus to the autoregulation system. Stimulus-dependent time domain methods cannot be used to analyze the complete information within the complex CBFv and MABP curves. Instead, CSA can be applied, which does not require a specific MABP stimulus. To interpret the results of CSA, it is useful to know that dynamic autoregulation has high pass filter properties.
High pass filter properties of dynamic autoregulation. The results of different studies indicated that cerebral autoregulation has properties of a high pass filter system(14, 16–18). A detailed description of a simple high pass filter model is given in “Appendix B.” In this context, the artificial step and sinusoidal MABP stimuli and their specific CBFv responses (Fig. 4) are only special cases of the same basic autoregulation system. If dynamic autoregulation has high pass filter properties, it can be expected that natural complex changes in MABP will lead to corresponding complex CBFv responses. As an example, autoregulation was simulated in record 19 (Fig. 6). The two model parameters T1/2 and C of the simple high pass filter model (“Appendix B”) were derived from the results of CSA (detailed information on request). The inspection of Figure 6 reveals that the simulated estimates curve is quite similar to the original CBFv curve, although the estimates have been calculated solely by MABP and only two model parameters, and both the CBFv and MABP curves include measurement errors. Tiecks et al.(14) have proposed and validated a second-order differential equation to describe the high pass filter properties of autoregulation. Further studies have to show whether those more complex models, perhaps including nonlinear components(17, 23), describe the cerebral autoregulation system even better.

Simulation of cerebral autoregulation by a simple high pass filter model. Based on a simple high pass filter model (“Appendix B”), dynamic autoregulation is simulated for record 19. Estimates for CBFv are calculated from the measured MABP values and only two model parameters T1/2 = 1.2 s and C = 2.4, which were derived from the results of CSA (details on request). (A) CBFv sometimes seems to oscillate in front of MABP. The temporal relationship between CBFv and MABP seems to be only weak, but this impression is rejected by a significant coherenceLF of 0.66 (p < 0.001). (B) The estimates show how a simple high pass filter would balance out the MABP LF oscillations. The estimates curve shows similarities with the original CBFv in detail, although the estimates are solely calculated from the measured MABP values and only two model parameters.
Analysis of autoregulation dynamics by CSA. All 30 records showed a significant temporal relationship between the LF oscillations of CBFv and MABP (p < 0.001). Within the study group, at 24 h of life phase-shiftLF was about 0 °, which indicates an impaired autoregulation when referring to the results of other studies(17, 18). Within the study group, phase-shiftLF increased significantly toward about 55 ° until 96 h of life, indicating a more or less active autoregulation in the corresponding patients at that time. Phase-shiftLF showed no significant correlations with postconceptional age or birth weight (p > 0.05). If phase-shiftLF is a valid measure for autoregulation, this indicates that, in preterm infants below 33 gw, not birth weight or postconceptional age, but the first few postnatal days are the main risk factor for IVH. This finding is in accordance with the fact that in preterm infants IVH occurs predominantly within the perinatal period and usually not after the first week of life(1, 2), independent of gestational age. So it is unlikely that a 16-d-old preterm infant of 26 gw develops a new IVH, whereas a 2-d-old preterm infant of 28 gw is at potential risk for IVH.
Comparison of phase-shiftLF with an independent measure for autoregulation. The results for phase-shiftLF were highly correlated (p < 0.01) with the results of the independent regression slope method of Panerai et al.(19). This supports the hypothesis that the phase-shiftLF between LF oscillations of CBFv and MABP may be used as an alternative measure for autoregulation, as long as there is no “gold-standard.”
Conclusions. Dynamic autoregulation and its high pass filter properties can be studied by CSA of natural CBFv and MABP LF oscillations. In our patients the LF spectral power of CBFv and MABP, and the phase-shiftLF between CBFv and MABP was initially low. This seems to indicate a postnatal depression of cerebral regulation centers and a “loss of autoregulation,” which may be caused by the stresses of the birth process or by the prenatal events that triggered the premature birth. Despite a generally low initial phase-shiftLF, only one of our patients developed a severe IVH. This is consistent with the known hypothesis that an impaired autoregulation is only the basis for IVH, which has then to be triggered by additional events such as excessive fluctuations in blood pressure or blood gases(1, 30). If in high risk preterm infants autoregulation is “lost” during the first days of life, a meticulous monitoring of the vital parameters and external control within a physiologic range may be beneficial, with the goal to prevent permanent cerebral lesions.
Abbreviations
- IVH:
-
intraventricular hemorrhage
- gw:
-
gestational weeks
- CBF(v):
-
cerebral blood flow (velocity)
- (M)ABP:
-
(mean) arterial blood pressure
- CSA:
-
cross-spectral analysis
- LF:
-
low frequency band (0.02-0.2 Hz)
- SPLF:
-
total spectral power within the LF band
- MABP-SPLF:
-
spectral power of MABP
- CBFv-SPLF:
-
LF spectral power of CBFv
- phase-shiftLF:
-
LF phase-shift between CBFv and MABP
- coherenceLF:
-
LF coherence between CBFv and MABP
- log-center-freqLF:
-
LF logarithmic center frequency
- T1/2:
-
half-maximal CBFv response time
References
Lou HC 1988 The “lost autoregulation hypothesis” and brain lesions in the newborn-an update. Brain Dev 10: 143–146.
Shortland DB, Levene M, Archer N, Shaw D, Evans D 1990 Cerebral blood flow velocity recordings and the prediction of intracranial haemorrhage and ischemia. J Perinat Med 18: 411–417.
Altman DI, Volpe JJ 1987 Cerebral blood flow in the newborn infant: measurement and role in the pathogenesis of periventricular and intraventricular hemorrhage. Adv Pediatr 34: 111–138.
Dykes FD, Ahmann PA, Baldzer K, Carrigan TA, Kitney R, Giddens DP 1986 Breath amplitude modulation of heart rate variability in normal full term neonates. Pediatr Res 20: 301–308.
Malliani A, Pagani M, Lombardi F, Cerutti S 1991 Cardiovascular neural regulation explored in the frequency domain. Circulation 84: 482–492.
Chatow U, Davidson S, Reichman BL, Akselrod S 1995 Development and maturation of the autonomic nervous system in premature and full-term infants using spectral analysis of heart rate fluctuations. Pediatr Res 37: 294–302.
Giller CA, Bowmann G, Dyer H, Mootz L, Krippner W 1993 Cerebral arterial diameters during changes in blood pressure and carbon dioxide during craniotomy. Neurosurgery 32: 737–742.
Newell DW, Aaslid R, Lam A, Mayberg TS, Winn HR 1994 Comparison of flow and velocity during dynamic autoregulation testing in humans. Stroke 25: 793–797.
Haaland K, Karlsson B, Skovlund E, Thoresen M 1994 Simultaneous measurements of cerebral circulation with electromagnetic flowmetry and Doppler ultrasound velocity in the newborn pig. Pediatr Res 36: 601–606.
Michel E, Zernikow B, Steck J, Kohlmann G, von Siebenthal K, Hirano S, Fock A, Casaer P, Jorch G 1994 Cyclic variation pattern of cerebral blood flow and postconceptional age. Eur J Pediatr 153: 751–755.
Anthony MY, Evans DH, Levene MI 1991 Cyclical variations in cerebral blood flow velocity. Arch Dis Child 66: 12–16.
Coughtrey H, Rennie JM, Evans DH 1992 Postnatal evolution of slow variability in cerebral blood flow velocity. Arch Dis Child 67: 412–415.
Paulson OB, Strandgard S, Edvinsson L 1990 Cerebral autoregulation. Cerebrovasc Brain Metab Rev 2: 161–192.
Tiecks FP, Lam AM, Aaslid R, Newell DW 1995 Comparison of static and dynamic cerebral autoregulation measurements. Stroke 26: 1014–1019.
Chatfield C 1989 The Analysis of Time Series: An Introduction, 4th ed. Chapman & Hall, London, pp 105–180.
Aaslid R, Lindegard KF, Sorteberg W, Nornes H 1989 Cerebral autoregulation dynamics in humans. Stroke 20: 45–52.
Birch AA, Dirnhuber MJ, Hartley-Davies R, Iannotti F, Neil-Dwyer G 1995 Assessment of autoregulation by means of periodic changes in blood pressure. Stroke 26: 834–837.
Diehl RR, Linden D, Lucke D, Berlit P 1995 Phase relationship between cerebral blood flow velocity and blood pressure. A clinical test of autoregulation. Stroke 26: 1801–1804.
Panerai RB, Kelsall AWR, Rennie JM, Evans DH 1995 Cerebral autoregulation dynamics in premature newborns. Stroke 26: 74–80.
Michel E, Zernikow B, von Twickel J, Hillebrand S, Jorch G 1995 Critical closing pressure in preterm neonates: towards a comprehensive model of cerebral autoregulation. Neurol Res 17: 149–155.
Michel E, Zernikow B 1994 Sample! Low cost hard- and software for 16-channel pressure monitoring. In: Mutz NJ, Koller W, Benzer H (eds) 7th European Congress on Intensive Care Medicine. Monduzzi Editore, Bologna, Italy, pp 1055–1058.
Michel E, Zernikow B, Rabe H, Jorch G 1993 Adaptive multipurpose probe fixation device for use on newborns. Ultrasound Med Biol 19: 581–586.
Zernikow B, Michel E, Kohlmann G, Steck J, Schmitt RM, Jorch G 1994 Cerebral autoregulation of preterm neonates-a non-linear control system? Arch Dis Child 70:F166–F173.
Rabe H, Grohs B, Schmidt RM, Schloo R, Bömelburg T, Jorch G 1990 Acoustic power measurements of Doppler ultrasound devices used for perinatal and infant examinations. Pediatr Radiol 20: 277–281.
Shimada SG, Marsh DJ 1979 Oscillations in mean arterial blood pressure in conscious dogs. Circ Res 44: 692–700.
Hamming RW 1983 Digital Filters. Prentice-Hall, Englewood Cliffs, NJ, pp 121–160.
Shott S 1990 Statistics for Health Professionals. WB Saunders, Philadelphia, pp 269–312.
Bignall S, Bailey PC, Rivers RPA, Lissauer TJ 1988 Quantification of cardiovascular instability in premature infants using spectral analysis of waveforms. Pediatr Res 23: 398–401.
Diehl RR, Diehl B, Sitzer M, Hennerici M 1991 Spontaneous oscillations in cerebral blood flow velocity in normal humans and in patients with carotid artery disease. Neurosci Lett 127: 5–8.
Menke J, Michel E, Rabe H, Bresser BW, Grohs B, Schmitt RM, Jorch G 1993 Simultaneous influence of blood pressure, Pco2, and Po2 on cerebral blood flow velocity in preterm infants of less than 33 weeks gestation. Pediatr Res 34: 173–177.
Rake H 1991 Regelungstechnik A und Ergänzungen (Regelungstechnik B). Institut für Regelungstechnik, Rheinisch-Westfälische Technische Hochschule Aachen, Aachen, pp 4/1–4/46
Heinbockel B Voβ HJ 1989 Alles geregelt-Reglersimulationsprogramm in Turbo Pascal 4/5. c't August 1989, Verlag Heinz Heise, Hannover, pp 140–160
Acknowledgements
The authors thank the parents and the nurses of the intensive care unit for their support.
Author information
Authors and Affiliations
Additional information
Supported in part by a grant of the Deutsche Forschungsgemeinschaft (Jo 156-2).
The raw data are part of the theses of J.v.T. and S.H.
Appendices
Appendix A
Description of LF spectral parameters. The following symbols are used: Equation

Calculation of LF spectral parameters Equation

Appendix B
Simple high pass filter model for dynamic cerebral autoregulation. In the time domain the general equation of a simple high pass filter system is given by (31): Equation

In control engineering theory this first-order differential equation describes a so-called DT1-element (31), which is a combination of a differential (D) and one (1) temporal (T) element and acts as a high pass filter (15, 17, 18). A high pass filter dampens especially LF MABP oscillations. High frequency MABP oscillations pass the high pass filter and lead to corresponding disturbances in CBF. The effect of step, sinusoidal, or more complex MABP changes on CBF can be visualized by computer simulation (32). Step and sinusoidal MABP changes and their specific CBF responses (Fig. 4) are only special cases of this generalized model. The general equation of the DT1-element can then be specified:
1) Step MABP increase (Fig. 4, A and C): Equation

Rights and permissions
About this article
Cite this article
Menke, J., Michel, E., Hillebrand, S. et al. Cross-Spectral Analysis of Cerebral Autoregulation Dynamics in High Risk Preterm Infants during the Perinatal Period. Pediatr Res 42, 690–699 (1997). https://doi.org/10.1203/00006450-199711000-00023
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199711000-00023
This article is cited by
-
Ultrasound imaging of preterm brain injury: fundamentals and updates
Pediatric Radiology (2022)
-
Cerebral oxygen saturation and autoregulation during hypotension in extremely preterm infants
Pediatric Research (2021)
-
Reduction of brain volumes after neonatal cardiopulmonary bypass surgery in single-ventricle congenital heart disease before Fontan completion
Pediatric Research (2018)
-
The Instrumented Fetal Sheep as a Model of Cerebral White Matter Injury in the Premature Infant
Neurotherapeutics (2012)
-
Cerebral Blood Flow Heterogeneity in Preterm Sheep: Lack of Physiologic Support for Vascular Boundary Zones in Fetal Cerebral White Matter
Journal of Cerebral Blood Flow & Metabolism (2008)
