
Abstract
Background:
Phosphorus status is inversely correlated with body weight; however, the effect of phosphorus supplementation on body weight in a controlled design has not been studied.
Methods:
This is a double-blind, randomized, placebo-controlled trial of 63 adults aged 18–45 years with a body mass index (BMI) of ⩾25 kg m−2 and normal kidney function at the American University of Beirut. Participants were randomly assigned to the placebo or phosphorus group where daily placebo or phosphorus supplements were ingested with three main meals (breakfast, lunch and dinner) for a period of 12 weeks. Primary outcomes were changes in anthropometric measures, blood metabolites (including lipid profile, glucose and insulin) and subjective appetite scores. The trial is registered with Clinical Trial.gov, NCT02329990.
Results:
Body weight was significantly lower in the phosphorus group when compared with the placebo group (−0.65 kg (95% confidence interval (CI) −1.69 to 0.40) vs 1.13 kg (95% CI 0.19 to 2.06), P=0.01). Similarly, BMI and waist circumference were significantly lower in the phosphorus group when compared with the placebo group (−0.24 kg m−2 (95% CI −0.59 to 0.12) vs 0.42 kg m−2 (95% CI 0.05 to 0.78), P=0.01; −3.62 cm (95% CI−4.90 to −2.33) vs 0.38 cm ( 95% CI−0.44 to 1.20), P<0.001; respectively). Several parameters of subjective appetite scores were decreased in the phosphorus-supplemented group.
Conclusions:
Phosphorus supplementation for 12 weeks significantly decreases body weight, BMI, waist circumference and subjective appetite scores. These findings support a promising role of the mineral phosphorus in the prevention and management of obesity, especially abdominal adiposity. The exact mechanisms of action and longer-term effects still need to be elucidated.
Similar content being viewed by others
Introduction
Obesity is increasing at alarming rates in many high-, medium- and low-income countries.1 This is contributing to the development of many metabolic diseases, including diabetes and cardiovascular disease.2
Modernization, including food industrialization and globalization of food markets, has been correlated with the increased consumption of products containing negligible amounts of phosphorus such as refined cereals (whereby refinement reduces phosphorus content by ∼70%), oils, sugars and sweeteners that are currently contributing to >50% of the food supply (kcal per capita per day) in most countries.3 This has caused a decrease in daily phosphorus ingestion to ∼1–1.5 g day−1,4, 5 as compared with our ancestors’ estimated intake of 2.5 g day−1 (based on primarily raw, unprocessed foods with a 2500 kcal day−1 diet and ∼1 mg phosphorus per kcal).3
Low phosphorus status has been positively associated with increased body weight.3, 6, 7 This may be attributed to the impact of hepatic adenosine triphosphate (ATP), which depends on adequate dietary supply of phosphorus, on suppressing food intake.3, 8, 9 This mechanism is supported by an inverse relation between body weight and hepatic ATP status.10, 11, 12 In line with that, we have previously found that phosphorus addition to carbohydrate preloads significantly reduces ad libitum energy intake at subsequent meal.13
Given the increased prevalence of obesity among individuals consuming abundant quantities of food containing low levels of phosphorus, it is reasonable to postulate that decreased phosphorus intake may be involved in the development of obesity and its metabolic abnormalities. Hence, we conducted a randomized, placebo-controlled trial to examine the effects of 12-week phosphorus supplementation on body weight, body mass index (BMI), waist circumference and subjective appetite scores in overweight and obese adults.
Materials and methods
Participants
After approval of the study by the institutional review board at the American University of Beirut (Beirut, Lebanon), 63 adults aged 18 to 45 years with a BMI ⩾25 kg m−2, who provided signed informed consent, were recruited from the general public using poster advertisements or direct approach. Details about recruitment, randomization and follow-up are presented in Figure 1. Exclusion criteria included glomerular filtration rate <60 ml min−1 per 1.73 m2, presence of any significant medical disease, pregnancy or lactation, regular administration of drugs that affect body weight and weight change of ⩾3% within 3 months before the study. The study was conducted between June 2013 and September 2014 at the American University of Beirut. We computed that the enrollment of 40 subjects (20 per group) would detect a 10% change in weight of the placebo group, assuming the latter having a mean weight of 90 kg and s.d. of 10 kg, with 80% power and an α of 5%. The trial is registered with Clinical Trial.gov, NCT02329990.

Study flow diagram.
Randomization and masking
This double-blind, randomized, controlled study allocated subjects into placebo group (n=21) or phosphorus group (n=26). Participants were requested to take three tablets containing either 375 mg phosphorus or a placebo (Nutricap Labs, Farmingdale, NY, USA) with each main meal (breakfast, lunch and dinner) for 12 weeks. They were asked to maintain regular dietary and physical activity habits during the entire study course and avoid alcohol consumption and any strenuous exercise 24 h before their visits (at baseline, 6 weeks and 12 weeks). Assignment to intervention or control group was made by having the principle investigator (corresponding author) ask the eligible subjects to blindly draw an envelope from a large box of 100 opaque, sealed envelopes (50 for each group), each containing a 2-cm by 2-cm paper with a written code designating intervention or control. There were no detectable differences in size or weight between intervention and control envelopes. In addition, both researchers and participants were blinded for the type of supplements that were similar in size, shape, color and odor.
Procedures
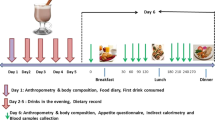
Subjects were asked to attend the research unit at baseline and after 6 and 12 weeks of participation. At baseline, anthropometric measurements and blood samples were collected and a subjective appetite questionnaire based on Wilson et al.14 was completed. Participants were given a 6-week supply of the allocated supplement and were asked to attend the research unit at the end of this period. At 6 weeks, remaining tablets were collected and counted in order to assess adherence to the allocated intervention. Participants were then given a supply of the same type of supplementation for the consequent 6 weeks and were asked to complete the subjective appetite questionnaire. At 12 weeks, data were collected similar to the baseline visit, and remaining tablets were counted to assess compliance. Individuals who consumed >70% of the allocated tablets were excluded.
Body weight and height (without shoes) were measured to the nearest 0.1 kg and 0.1 cm, using a calibrated Seca balance (Hamburg, Germany) and a portable stadiometer, respectively. Blood was withdrawn after overnight fast and samples were centrifuged for 15 min at 3500 r.p.m. at 3 °C for serum and plasma separation. Sample aliquots were stored at −80 °C until analysis. Serum phosphorus, creatinine, C-reactive protein, total cholesterol, high-density lipoprotein cholesterol, triglyceride and glucose levels were measured using the Vitros 350 analyzer (Ortho Clinical Diagnostics, Johnson and Johnson, Buckinghamshire, UK). The Friedwald formula15 was used to calculate low-density lipoprotein cholesterol levels. Fasting insulin concentration was measured using the ELISA kit (Diametra Millipore, Billerica, MA, USA). HOMA-IR (homeostasis model assessment of insulin resistance) was calculated as described by Matthews et al.16 Glomerular filtration rate was calculated using CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) estimated glomerular filtration rate.17
Statistical analysis
Pairwise changes from baseline to 12-week follow-up anthropometric and biochemical variables were tested using paired t-tests, and intergroup assessment was performed using two-sample t-test. Repeated measures analysis of variance test was applied to analyze intragroup variation of appetite scores at different periods of time (baseline, 6 weeks and 12 weeks). Statistical analyses were conducted using SPSS 22 (Chicago, IL, USA).
Role of the funding source
The study was funded by the National Council for Scientific Research, Lebanon. The funding source had no role in the study design or conduct; data collection, analysis, interpretation or reporting of the data; preparation, review or approval of the manuscript; or decision to submit the manuscript for publication.
Results
Subject characteristics
Baseline characteristics are shown in Table 1, and they were similar between groups. In all, 47 participants (placebo group n=21; phosphorus group n=26) completed the intervention, and all subjects had normal glomerular filtration rate (>60 ml min−1 per 1.73 m2) with a mean of 114.14 (10.19) ml min−1 per 1.73 m2 and 112.24 (13.46) ml min−1 per 1.73 m2 for the placebo and phosphorus groups, respectively. The mean age was 36.67 (9.76) years in the placebo group and 34.04 (11.24) years in the phosphorus group. No side effects were reported by participants over the experimental period.
Anthropometric assessments
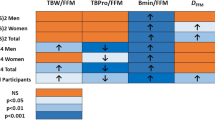
Changes in anthropometric and biochemical characteristics from baseline to 12 weeks are shown in Table 2. Body weight of the placebo group increased significantly from baseline by 1.13 kg (95% confidence interval (CI) 0.19 to 2.06), whereas that of the phosphorus group decreased by 0.65 kg (95% CI −1.69 to 0.40). These variations resulted in a significant difference (P=0.01) in the changes in body weight between the two groups. Consequently, the changes in BMI of the placebo group (0.42 kg m−2, 95% CI 0.05 to 0.78) was significantly different (P=0.01) than that of the phosphorus group (−0.24 kg m−2, 95% CI −0.59 to 0.12). Simultaneously, waist circumference of the phosphorus group was significantly reduced by 3.62 cm (95% CI −4.90 to −2.33), and this reduction was significantly different (P<0.001) from the small increase of 0.38 cm (95% CI −0.44 to 1.20) in the waist circumference of the placebo group.
Biochemical assessments
Placebo or phosphorus treatment for 12 weeks did not affect serum levels of phosphorus, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglyceride, glucose and C-reactive protein. Serum levels of insulin and HOMA-IR were similar between the two treatments at baseline and at 12 weeks, although a mild but significant difference was detected in their changes. This mild change is not believed to be of clinical significance (Table 2).
Subjective appetite scores
Baseline subjective appetite scores were similar between groups. The changes in several parameters of subjective appetite scores were found to decrease as the experiment progressed including that of appetite, quantity of food to reach fullness, hunger and number of snacks. However, changes in appetite, quantity of food to reach fullness, taste of food and number of snacks were significantly reduced in the phosphorus group as compared with the placebo as shown in Table 3.
Discussion
Several dietary patterns and interventions were reported to improve body weight.18, 19, 20, 21, 22 High protein diets were constantly found to induce weight loss, probably because of their capacity to decrease energy intake and increase energy expenditure.18, 23, 24 Consumption of dairy products was also shown to be inversely related to body weight, whereby its increased intake among overweight individuals was reported to lower body weight,19, 25 irrespective of its calcium content.26 Moreover, the intake of whole grains was shown to be negatively associated with the risk of different components of the metabolic syndrome, including body weight;20, 21 however, the mechanism of such effect remains uncertain.27 This raises the questions on the role of macronutrients in weight reduction, especially as these dietary patterns or interventions have varied macronutrient profiles.22 The common feature between these diets seems to be their phosphorus content, as proteins, dairy products and whole grains are rich sources of phosphorus.28 This was the rationale for our proposed hypothesis on the involvement of low phosphorus status in the development of obesity and metabolic syndrome.3, 29
Our study found that the ingestion of 375 mg phosphorus with each main meal, over a period of 12 weeks, was able to prevent weight gain and to reduce waist circumference among overweight and obese adults. However, minimal alterations were observed in the measured biochemical parameters (lipid profile, glucose and so on) that may be attributed to the modest baseline abnormalities in these parameters, short experimental duration and/or to the modest anthropometric changes. The absence of change in fasting plasma phosphorus further confirms that it is not a good marker of phosphorus intake.30
The anthropometric changes in the phosphorus group are in line with other studies in which phosphorus status was reported to be inversely related to body weight3, 6, 7, 29 and waist circumference.3, 31, 32 The mechanism(s) by which phosphorus affected body weight may have been related to its involvement in food intake control and/or energy metabolism.3 Phosphorus availability is known to stimulate ATP production, in particular hepatic ATP,8, 33 that is believed to transmit afferent neural signals to the central nervous system resulting in a decrease in food intake8 through the stimulation of satiation. Such effect was believed to be behind the impact of phosphorus addition to different carbohydrate preloads on the suppression of ad libitum energy intake at subsequent meal.13 In agreement, as reported in the subjective appetite questionnaires, satiation indicated by the quantity of food to reach fullness was reduced in the phosphorus group; however, the number of main meals, which is an indicator of satiety, was not reduced. Sustenance of hepatic ATP production over the postprandial and postabsorptive periods may have contributed to the observed reduction in appetite and number of snacks and these may have been translated by subjects into taste changes. Conversely, the similarity in the scores of hunger (that is, physiological controlled by depletion of energy stores) and the number of main meals between the phosphorus and placebo groups may be explained by a limited availability of hepatic ATP substrates beyond postprandial and postabsorptive periods, and thus an inability to impact the initiation of the next main meal. In brief, the impact of phosphorus supplement on energy intake seems to be related to its capacity to reduce the size of main meals (low appetite and high fullness) as well as intake between meals (number of snacks).
Furthermore, the favorable differences in body weight and waist circumference in the phosphorus group may have been partially related to an effect of phosphorus on energy metabolism. The addition of phosphorus to orange juice was reported to increase postprandial thermogenesis among obese but not lean subjects.34, 35 In addition, phosphorus supplementation in a weight reducing program was found to increase resting metabolic rate of obese subjects.36, 37 The pronounced reduction in waist circumference in the face of the modest reduction in body weight may have been attributed to changes in body composition. Weight gain under phosphorus-deficient diet was reported to be largely attributed to an increase in adipose tissue, whereas nitrogen retention was impaired,38 and this seems to mimic that of low-protein (low-phosphorus) diet.23 Changes in body fat were reported to be related to energy intake, whereas changes in lean body mass were related to the intake of protein,23 known to be high in phosphorus and this raises a question of whether the effect of protein on weight gain is linked to its content of phosphorus. It is not clear whether phosphorus supplementation favored lean body mass retention that ultimately masked the effect on changes in body weight because of its capacity to retain water. In any case, the observed reduction in waist circumference was similar to that reported in subjects under low-fat diets,22 and is believed to be of clinical significance as it is an indicator of abdominal obesity (visceral fat) that is known to be a risk factor of type 2 diabetes and cardiovascular disease.39, 40
Many concerns were raised on the relation between phosphorus status and cardiovascular disease and mortality,41, 42 although the nature of the relation with phosphorus intake is far from clear and requires further scrutiny,43 especially as fasting serum phosphorus does not reflect intake30, 44 as confirmed by our results. The fact that fasting but not nonfasting (that reflects intake rather than clearance) serum phosphorus levels were associated with increased mortality45 and fasting serum phosphorus level but not dietary intake were associated with coronary artery calcification46 may imply that factors behind or associated with elevated fasting serum phosphorus rather than phosphorus intake may have attributed to these detrimental effects. The recent reported weak association between dietary phosphorus intake and all-cause mortality44 was questioned as varied dietary habits or profiles were seen among the different dietary phosphorus intake quartiles. Moreover, such association may have been cofounded by the source of phosphorus in the diet, especially as dietary heme iron intake (derived from animal source that is also high in phosphorus) was shown to increase the risk of cardiovascular disease.47 It is believed that the need of phosphorus especially for carbohydrate metabolism may have been compromised by modernization (refinement and so on), particularly in staple carbohydrate-rich foods (rice, wheat and so on). The impact of such a compromise is expected to depend on the contribution of staple food to total energy intake and may partially be behind the drastic increase in obesity in developing countries, in particular as carbohydrate contribution to total energy intake is inversely related to income.48
The weaknesses of the study include: the lack of biomarker for phosphorus intake, the use of the subjective self-reported visual analog scale (VAS) for the determination of appetite scores and the lack of analyses for body composition and energy expenditure.
The strength of our study was that a rigorous system of training and certification of study personnel was developed and implemented for collecting all data. In addition, our study is pragmatic, randomized, double blinded and placebo controlled that required the use of tablets without requesting behavioral or dietary changes to avoid the problem of adherence.
Conclusion
In summary, this 12-week randomized, placebo-controlled trial showed that phosphorus supplementation (375 mg per main meal) halted weight gain and BMI while significantly decreasing waist circumference. This may have been related to favorable changes in body composition. At the same time, these changes were associated with early satiation, whereas satiety (number of main meals) and hunger were not altered. Our findings support a promising role of the mineral phosphorus in preventing obesity, especially abdominal adiposity. Therefore, after extensive investigations, phosphorus utilization could be considered for the future development of weight maintenance or reduction supplements or implementation of flour fortification. Additional research is warranted to examine the exact mechanisms of actions and longer-term effects of phosphorus.
References
Tesauro M, Iantorno M, Campia U . Obesity-related metabolic syndrome and vascular complications. Int J Endocrinol 2013; 2013: 534056.
Tsai AG, Wadden TA . In the clinic: obesity. Ann Intern Med 2013; 159, ITC3-1-ITC3-15; quiz ITC3-16.
Obeid O . Low phosphorus status might contribute to the onset of obesity. Obes Rev 2013; 14: 659–664.
Ervin RB, Wang CY, Wright JD, Kennedy-Stephenson J . Dietary intake of selected minerals for the United States population: 1999–2000. Energy 2004; 1: 6.
Gattineni J, Baum M . Genetic disorders of phosphate regulation. Pediatr Nephrol 2012; 27: 1477–1487.
Håglin L . Hypophosphataemia: cause of the disturbed metabolism in the metabolic syndrome. Med Hypotheses 2001; 56: 657–663.
Foley RN, Collins AJ, Herzog CA, Ishani A, Kalra PA . Serum phosphorus levels associate with coronary atherosclerosis in young adults. J Am Soc Nephrol 2009; 20: 397–404.
Friedman MI . Obesity and the hepatic control of feeding behavior. Drug News Perspect 2007; 20: 573–578.
Langhans W, Scharrer E . Metabolic control of eating. World Rev Nutr Diet 1992; 70: 1.
Nair S, P Chacko V, Arnold C, Diehl AM . Hepatic ATP reserve and efficiency of replenishing: comparison between obese and nonobese normal individuals. Am J Gastroenterol 2003; 98: 466–470.
Wlodek D, Gonzales M . Decreased energy levels can cause and sustain obesity. J Theor Biol 2003; 225: 33–44.
Schmid AI, Szendroedi J, Chmelik M, Krssák M, Moser E, Roden M . Liver ATP synthesis is lower and relates to insulin sensitivity in patients with type 2 diabetes. Diabetes Care 2011; 34: 448–453.
Obeid O, Dimachkie S, Hlais S . Increased phosphorus content of preload suppresses ad libitum energy intake at subsequent meal. Int J Obes 2010; 34: 1446–1448.
Wilson MMG, Thomas DR, Rubenstein LZ, Chibnall JT, Anderson S, Baxi A et al. Appetite assessment: simple appetite questionnaire predicts weight loss in community-dwelling adults and nursing home residents. AJCN 2005; 82: 1074–1081.
Friedewald WT, Levy RI, Fredrickson DS . Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972; 18: 499–502.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC . Homeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985; 28: 412–419.
National Kidney Disease Education Program (NKDEP). GFR MDRD Calculator for Adults (SI units) 2015. Accessed online on 13 January 2015; Available from http://nkdep.nih.gov/lab-evaluation/gfr-calculators/adults-SI-units.asp.
Pioli K, Barbieri C, Cann T, Mackie R, Beverly J . High protein diet reduces food intake and adiposity and alters GI microbiome. FASEB J 2013; 27: 1056.14.
Pereira MA, Jacobs Jr DR, Van Horn L, Slattery ML, Kartashov AI, Ludwig DS . Dairy consumption, obesity, and the insulin resistance syndrome in young adults: the CARDIA Study. JAMA 2002; 287: 2081–2089.
Kristensen M, Toubro S, Jensen MG, Ross AB, Riboldi G, Petronio M et al. Whole grain compared with refined wheat decreases the percentage of body fat following a 12-week, energy-restricted dietary intervention in postmenopausal women. J Nutr 2012; 142: 710–716.
Ye EQ, Chacko SA, Chou EL, Kugizaki M, Liu S . Greater whole-grain intake is associated with lower risk of type 2 diabetes, cardiovascular disease, and weight gain. J Nutr 2012; 142: 1304–1313.
Bazzano LA, Hu T, Reynolds K, Yao L, Bunol C, Liu Y et al. Effects of low-carbohydrate and low-fat diets: a randomized trial. Ann Intern Med 2014; 161: 309–318.
Bray GA, Smith SR, de Jonge L, Xie H, Rood J, Martin CK et al. Effect of dietary protein content on weight gain, energy expenditure, and body composition during overeating: a randomized controlled trial. JAMA 2012; 307: 47–55.
Ebbeling CB, Swain JF, Feldman HA, Wong WW, Hachey DL, Garcia-Lago E et al. Effects of dietary composition on energy expenditure during weight-loss maintenance. JAMA 2012; 307: 2627–2634.
Murphy KJ, Crichton GE, Dyer KA, Coates AM, Pettman TL, Milte C . Dairy foods and dairy protein consumption is inversely related to markers of adiposity in obese men and women. Nutrients 2013; 5: 4665–4684.
Yanovski JA, Parikh SJ, Yanoff LB, Denkinger BI, Calis KA, Reynolds JC et al. Effects of calcium supplementation on body weight and adiposity in overweight and obese adults: a randomized trial. Ann Intern Med 2009; 150: 821–829.
Slavin J . Why whole grains are protective: biological mechanisms. Proc Nutr Soc 2003; 62: 129–134.
Takeda E, Yamamoto H, Yamanaka-Okumura H, Taketani Y . Dietary phosphorus in bone health and quality of life. Nutr Rev 2012; 70: 311–321.
Obeid O, Hachem D, Ayoub J . Refeeding and metabolic syndromes: two sides of the same coin. Nutr Diabetes 2014; 4: e120.
de Boer IH, Rue TC, Kestenbaum B . Serum phosphorus concentrations in the third National Health and Nutrition Examination Survey (NHANES III). Am J Kidney Dis 2009; 53: 399–407.
Lind L, Lithell H, Hvarfner A, Pollare T, Ljunghall S . On the relationships between mineral metabolism, obesity and fat distribution. Eur J Clin Invest 1993; 23: 307–310.
Park W, Kim BS, Lee JE, Huh JK, Kim BJ, Sung KC et al. Serum phosphate levels and the risk of cardiovascular disease and metabolic syndrome: a double-edged sword. Diabetes Res Clin Pract 2009; 83: 119–125.
Morris Jr RC, Nigon K, Reed EB . Evidence that the severity of depletion of inorganic phosphate determines the severity of the disturbance of adenine nucleotide metabolism in the liver and renal cortex of the fructose-loaded rat. J Clin Invest 1978; 61: 209.
Jaedig S, Lindgärde F, Arborelius M . Increased postprandial energy expenditure in obese women after peroral K-and Mg-phosphate. Miner Electrolyte Metab 1994; 20: 147–152.
Jaedig S, Henningsen NC . Increased metabolic rate in obese women after ingestion of potassium, magnesium-and phosphate-enriched orange juice or injection of ephedrine. Int J Obes 1991; 15: 429–436.
Kaciuba-Uściłko H, Nazar K, Chwalbińska-Moneta J, Ziemba A, Kruk B, Szczepanik J et al. Effect of phosphate supplementation on metabolic and neuroendocrine responses to exercise and oral glucose load in obese women during weight reduction. J Physiol Pharmacol 1993; 44: 425–440.
Nazar K, Kaciuba-Uściłko H, Szczepanik J, Zemba AW, Kruk B, Chwalbińska-Moneta J et al. Phosphate supplementation prevents a decrease of triiodothyronine and increases resting metabolic rate during low energy diet. J Physiol Pharmacol 1996; 47: 373–383.
Rudman D, Millikan WJ, Richardson TJ, Bixler TJ 2nd, Stackhouse J, McGarrity WC . Elemental balances during intravenous hyperalimentation of underweight adult subjects. J Clin Invest 1975; 55: 94–104.
Rader DJ . Effect of insulin resistance, dyslipidemia, and intra-abdominal adiposity on the development of cardiovascular disease and diabetes mellitus. Am J Med 2007; 120: S12–S18.
Bays H . Central obesity as a clinical marker of adiposopathy; increased visceral adiposity as a surrogate marker for global fat dysfunction. Curr Opin Endocrinol Diabetes Obes 2014; 21: 345.
Kestenbaum B, Sampson JN, Rudser KD, Patterson DJ, Seliger SL, Young B et al. Serum phosphate levels and mortality risk among people with chronic kidney disease. J Am Soc Nephrol 2005; 16: 520–528.
Tonelli M, Sacks F, Pfeffer M, Gao Z, Curhan G, Cholesterol And Recurrent Events Trial Investigators. Relation between serum phosphate level and cardiovascular event rate in people with coronary disease. Circulation 2005; 112: 2627–2633.
Gutiérrez MO . The connection between dietary phosphorus, cardiovascuoar disease, and mortality: where we stand and what we need to know. Adv Nutr 2013; 4: 723–729.
Chang AR, Lazo M, Appel LJ, Gutiérrez OM, Grams ME . High dietary phosphorus intake is associated with all-cause mortality: results from NHANES III. Am J Clin Nutr 2014; 99: 320–327.
Chang AR, Grams ME . Serum phosphorus and mortality in the Third National Health and Nutrition Examination Survey (NHANES III): effect modification by fasting. Am J Kidney Dis 2014; 64: 567–573.
Kwak SM, Kim JS, Choi Y, Chang Y, Kwon MJ, Jung JG et al. Dietary intake of calcium and phosphorus and serum concentration in relation to the risk of coronary artery calcification in asymptomatic adults. Arterioscler Thromb Vasc Biol 2014; 34: 1763–1769.
Fang X, An P, Wang H, Wang X, Shen X, Li X et al. Dietary intake of heme iron and risk of cardiovascular disease: a dose–response meta-analysis of prospective cohort studies. Nutr Metabol Cardiovasc Dis 2015; 25: 24–35.
Popkin BM, Gordon-Larsen P . The nutrition transition: worldwide obesity dynamics and their determinants. Int J Obes 2004; 28: S2–S9.
Acknowledgements
The study was funded by the National Council for Scientific Research, Lebanon.
Author contributions
Conception and design: OA Obeid; analysis and interpretation of the data: OA Obeid, JJ Ayoub, MS Bassil, SA Hlais and MJ Abou Samra; drafting of the article: JJ Ayoub and MJ Abou Samra; critical revision of the article for important intellectual content: OA Obeid, MS Bassil and SA Hlais; final approval of the article: OA Obeid; provision of study materials or patients: JJ Ayoub and MJ Abou Samra; statistical expertise: SA Hlais and OA Obeid; obtaining of funding: OA Obeid and MS Bassil; administrative, technical or logistic support: OA Obeid, JJ Ayoub and MJ Abou Samra; collection and assembly of data: JJ Ayoub and MJ Abou Samra.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Ayoub, J., Samra, M., Hlais, S. et al. Effect of phosphorus supplementation on weight gain and waist circumference of overweight/obese adults: a randomized clinical trial. Nutr & Diabetes 5, e189 (2015). https://doi.org/10.1038/nutd.2015.38
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nutd.2015.38
This article is cited by
-
Serum TSH, 25(OH) D and phosphorus levels predict weight loss in individuals with diabetes/prediabetes and morbid obesity: a single-center retrospective cohort analysis
BMC Endocrine Disorders (2022)
-
Automated and personalized meal plan generation and relevance scoring using a multi-factor adaptation of the transportation problem
Soft Computing (2022)
