
Abstract
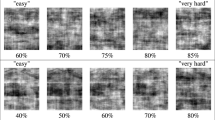
Signal detection theory tests an observer's ability to discriminate between signal and noise. Deciding whether or not a patient's symptoms warrant further investigation or treatment is an example of this task in the clinical setting. Noise can exist within the observer—for example, in the brain of a tired or inexperienced doctor—or can arise from an external source such as the patient. Patients can produce external noise by giving numerous unrelated presenting complaints, providing overly detailed accounts of their symptoms, or simply talking too quickly. The more noise that is present, the harder the signal (such as a new disease or a notable change in an old condition) is to detect. Patients in the neurology clinic seem to be 'noisier' than average, perhaps owing to the long duration of their condition in many cases and the relatively high proportion of patients with medically unexplained symptoms. The ability to interpret such 'noisy' histories often underpins the neurological diagnosis. This Review aims to promote the relevance of signal detection theory to the overworked neurologist on the ward or in the clinic and explores strategies to reduce the noise generated both within the brain of the doctor and by patients.
Key Points
-
Signal detection theory offers a powerful model to explain decision-making processes in the laboratory, and it can also be applied to the setting of clinical consultation
-
Signal becomes harder to distinguish from noise when we are tired or trying to hold too much information in our working memory
-
The way in which patients present information might make important symptoms harder to distinguish from less clinically relevant ones
-
Patients in neurology might be 'noisier' than average, owing to the often long-standing duration of their condition and the greater proportion that have medically unexplained symptoms
-
Strategies to reduce noise include writing down key facts as they emerge, getting patients to self-filter their symptoms, and asking the patients to focus on one presenting complaint at a time
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout





Similar content being viewed by others

References
Heeger D (1997) Signal detection theory [http://www.cns.nyu.edu/~david/sdt/sdt.html]
Chavanet P et al. (2006) Performance of a predictive rule to distinguish bacterial and viral meningitis. J Infect 54: 328–336
McFall RM and Treat TA (1999) Quantifying the information value of clinical assessments with signal detection theory. Annu Rev Psychol 50: 215–241
Green M and Swets J (1966) Signal Detection and Psychophysics. New York: John Wiley & Sons
Théberge I et al. (2005) Volume of screening mammography and performance in the Quebec population-based Breast Cancer Screening Program. CMAJ 172: 195–199
Schriger D et al. (1998) Cranial computed tomography interpretation in acute stroke. JAMA 279: 1293–1296
Chimowitz MI et al. (1990) The accuracy of bedside neurological diagnoses. Ann Neurol 28: 78–85
Morton C and Mackie R (1998) Clinical accuracy of the diagnosis of cutaneous malignant melanoma. Br J Dermatol 138: 283–287
Weideman RA et al. (1999) Pharmacist recognition of potential drug interactions. Am J Health Syst Pharm 56: 1524–1529
See JE et al. (1995) Meta-analysis of the sensitivity decrement in vigilance. Psychol Bull 117: 230–249
Tucker P et al. (2003) Rest breaks and accident risk. Lancet 361: 680
Parasuranam R and Davies D (1977) A taxonomic analysis of vigilance performance. In Vigilance: Theory, Operational Performance, and Psychological Correlates, 559–574 (Ed Mackie RR) New York: Plenium
Koelega H et al. (1989) Processing demands, effort, and individual differences in four different vigilance tasks. Hum Factors 31: 45–62
Garg A et al. (2005) Effects of computerized clinical decision support systems on practitioner performance and patient outcomes—a systematic review. JAMA 293: 1223–1238
Kawamoto K et al. (2005) Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success. BMJ 330: 765–772
Ji D and Wilson MA (2007) Coordinated memory replay in the visual cortex and hippocampus during sleep. Nat Neurosci 10: 100–107
Walker MP and Stickgold R (2004) Sleep-dependent learning and memory consolidation. Neuron 44: 121–133
Friedman RC et al. (1971) The intern and sleep loss. N Engl J Med 285: 201–203
Horne JA et al. (1983) Effects of sleep deprivation on signal detection measures of vigilance: implications for sleep function. Sleep 6: 347–358
Blagrove M et al. (1995) The effects of chronic sleep reduction on the performance of cognitive tasks sensitive to sleep deprivation. Appl Cogn Psychol 9: 21–40
Frey R et al. (2002) Effect of rest on physicians' performance in an emergency department, objectified by electroencephalographic analyses and psychometric tests. Crit Care Med 30: 2322–2329
Philibert I (2005) Sleep loss and performance in residents and nonphysicians: a meta-analytic examination. Sleep 28: 1351–1353
Firth-Cozens J and Cording H (2004) What matters more in patient care? Giving doctors shorter hours of work or a good night's sleep? Qual Saf Health Care 13: 165–166
Fletcher KE et al. (2004) Systematic review: effects of resident work hours on patient safety. Ann Intern Med 141: 851–857
Benowitz NL (1990) Clinical pharmacology of caffeine. Annu Rev Med 41: 277–288
Battig K and Buzzi R (1986) Effect of coffee on the speed of subject-paced information processing. Neuropsychobiology 16: 126–130
Frewer LJ and Lader M (1991) The effects of caffeine on two computerized tests of attention and vigilance. Hum Psychopharmacol 6: 119–128
MayoClinic.com: tools for healthier lives: how much caffeine is in your daily habit? [https://www.mayoclinic.com/health/caffeine/AN01211]
Angelucci ME et al. (1999) The effect of caffeine in animal models of learning and memory. Eur J Pharmacol 373: 135–140
Angelucci ME et al. (2002) Effects of caffeine on learning and memory in rats tested in the Morris water maze. Braz J Med Biol Res 35: 1201–1208
Foulds J et al. (1996) Cognitive performance effects of subcutaneous nicotine in smokers and never-smokers. Psychopharmacology (Berl) 127: 31–38
Pashler HE (1998) The Psychology of Attention. Cambridge: MIT Press
Gorea A and Sagi D (2000) Failure to handle more than one internal representation in visual detection tasks. Proc Natl Acad Sci USA 97: 12380–12384
Gorea A and Sagi D (2002) Natural extinction: a criterion shift phenomenon. Vis Cogn 9: 913–936
Speier C et al. (1997) The effects of task interruption and information presentation on individual decision making. In Proceedings of the 18th International Conference on Information Systems: 1997 December 14–17; Atlanta, 21–35 (Eds. DeGross JI and Kumar K) New York: Association for Computing Machinery
Seymour J et al. (1995) Response of headaches to nonnarcotic analgesics resulting in missed intracranial hemorrhage. Am J Emerg Med 13: 43–45
Reuber M et al. (2004) Failure to recognize psychogenic nonepileptic seizures may cause death. Neurology 62: 834–835
Gander P et al. (2007) Work patterns and fatigue related-risk among junior doctors. Occup Environ Med 64: 733–738
Smit AS et al. (2004) Mental effort causes vigilance decrease due to resource depletion. Acta Psychol (Amst) 115: 35–42
Neuchterlein KH et al. (1983) Visual sustained attention: image degradation produces rapid sensitivity decrement over time. Science 220: 327–329
Sarter M et al. (2001) The cognitive neuroscience of sustained attention: where top-down meets bottom-up. Brain Res Brain Res Rev 35: 146–160
Jones JW et al. (1988) Stress and medical malpractice: organizational risk assessment and intervention. J Appl Psychol 4: 727–735
Firth-Cozens J (2001) Interventions to improve physicians' well-being and patient care. Soc Sci Med 52: 215–222
Schon F et al. (2002) Is clinical neurology really so difficult? J Neurol Neurosurg Psychiatry 72: 557–559
Dacre J et al. (2003) MRCP(UK) Part 2 Clinical Examination (PACES): a review of the first four examination sessions (June 2001–July 2002). Clin Med 3: 452–459
Nahm FKD (2001) Neurology, technology, and the diagnostic imperative. Perspect Biol Med 44: 99–107
Caplan L and Hollander J (2001) The Effective Clinical Neurologist, edn 2. Oxford: Butterworth-Heinemann
Dubos F et al. (2006) Clinical decision rules to distinguish between bacterial and aseptic meningitis. Arch Dis Child 91: 647–650
Swets JA et al. (1979) Assessment of diagnostic technologies. Science 205: 753–759
Reuber M et al. (2005) Functional symptoms in neurology: questions and answers. J Neurol Neurosurg Psychiatry 76: 307–314
Nimnuan C et al. (2001) Medically unexplained symptoms: an epidemiological study in seven specialities. J Psychosom Res 51: 361–367
Scrag A et al. (2004) Reliability of self-reported diagnoses in patients with neurologically unexplained symptoms. J Neurol Neurosurg Psychiatry 75: 608–611
Ridsdale L et al. Royal College of General Practitioners Curriculum Statement 15.7: Neurological Problems [http://www.rcgp-curriculum.org.uk/PDF/curr_15_7_Neurological_problems.pdf] (accessed 29 February 2008)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Supplementary information
Supplementary Box 1
The ability of neurologists, radiologists and emergency physicians to detect infarction or hemorrhage on cranial CT. (DOC 55 kb)
Supplementary Box 2
The ability of clinicians to detect malignant melanoma. (DOC 24 kb)
Supplementary Box 3
Signal detection: clinical observation versus radiological investigation. (DOC 26 kb)
Rights and permissions
About this article
Cite this article
Oliver, R., Bjoertomt, O., Greenwood, R. et al. 'Noisy patients'—can signal detection theory help?. Nat Rev Neurol 4, 306–316 (2008). https://doi.org/10.1038/ncpneuro0794
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ncpneuro0794
