
Abstract
Introduction:
To characterise the nutritional status in children with obesity or wasting conditions, European anthropometric reference values for body composition measures beyond the body mass index (BMI) are needed. Differentiated assessment of body composition in children has long been hampered by the lack of appropriate references.
Objectives:
The aim of our study is to provide percentiles for body composition indices in normal weight European children, based on the IDEFICS cohort (Identification and prevention of Dietary- and lifestyle-induced health Effects in Children and infantS).
Methods:
Overall 18 745 2.0–10.9-year-old children from eight countries participated in the study. Children classified as overweight/obese or underweight according to IOTF (N=5915) were excluded from the analysis. Anthropometric measurements (BMI (N=12 830); triceps, subscapular, fat mass and fat mass index (N=11 845–11 901); biceps, suprailiac skinfolds, sum of skinfolds calculated from skinfold thicknesses (N=8129–8205), neck circumference (N=12 241); waist circumference and waist-to-height ratio (N=12 381)) were analysed stratified by sex and smoothed 1st, 3rd, 10th, 25th, 50th, 75th, 90th, 97th and 99th percentile curves were calculated using GAMLSS.
Results:
Percentile values of the most important anthropometric measures related to the degree of adiposity are depicted for European girls and boys. Age- and sex-specific differences were investigated for all measures. As an example, the 50th and 99th percentile values of waist circumference ranged from 50.7–59.2 cm and from 51.3–58.7 cm in 4.5– to <5.0-year-old girls and boys, respectively, to 60.6–74.5 cm in girls and to 59.9–76.7 cm in boys at the age of 10.5–10.9 years.
Conclusion:
The presented percentile curves may aid a differentiated assessment of total and abdominal adiposity in European children.
Similar content being viewed by others

Introduction
Anthropometric measurements provide essential information regarding body composition in children. They may also herald the presence of cardiovascular risk factors already in childhood as demonstrated in previous studies.1, 2, 3 Thus, a more sophisticated approach to assess body composition early in childhood may improve the prediction of cardiometabolic risk.4
Efforts to obtain detailed information on body composition in children have been impeded by two factors. First, an optimal method for precise assessment of body composition is not available. There are accurate laboratory methods for the analysis of total and abdominal fat, like dual energy X-ray absorptiometry, magnetic resonance imaging or underwater weighing but their routine use for screening purposes is limited.5,6 Traditional field anthropometric measurements are much cheaper and relatively easy to perform, but less precise. Second, the correct interpretation of the obtained results on both individual and population level is hampered by the lack of appropriate reference data7 according to sex, age and ethnicity. The assessment of body composition and body fat distribution is complex in children as the continuous growth and development leads to marked changes in circumferences, skinfold thicknesses8,9 and fat distribution.
BMI is the most widely used indicator for screening of excess adiposity and cardiometabolic risk,10,11 although its limitations, especially in growing children, are well established.12 Internationally accepted body mass index (BMI) reference values are available.13 For this reason, we provide BMI reference curves only for the sake of comparability between our study and other published data.
BMI does not distinguish between fat and lean body mass, which might provide misleading information concerning body composition. There is a high variability in body fat for a given BMI in children.14 The limitations of BMI can be partly overcome by the measurement of other anthropometric parameters and indices. For the assessment of total body fat, skinfold thicknesses,15,16 neck circumference (NC)17 and fat mass index (FMI)7 can be used. Measurement of abdominal fat, waist circumference (WC),18, 19, 20, 21, 22, 23 or waist-to-height ratio24 is recommended to improve the assessment of cardiometabolic risk.
For such anthropometric measures, reference charts have been developed for specific populations like North Americans,25 Canadians26 and Australians,27 which may not be suitable for European children. In Europe, only national standards exist,14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24 which may not be applicable on a European level.
The main goal of the present investigation is to provide reference standards of body composition measures allowing a differentiated assessment of body composition, that is, total and abdominal fat, in European children. Percentile curves were calculated using the General Additive Model for Location Scale and Shape (GAMLSS).28,29
Subjects and methods
Study subjects
A cohort of 16 228 children aged 2–9 years was examined in a population-based baseline survey in 16 study regions in eight European countries (Sweden, Germany, Hungary, Italy, Cyprus, Spain, Belgium, Estonia) ranging from North to South and from East to West from autumn 2007 to spring 2008. This baseline survey (T0) was the starting point of the largest prospective European children’s cohort established to date. This cohort and additional 2517 children aged 2.0–10.9 years who were newly recruited during a second survey (T1), 2 years later, comprise the study sample of the present analysis, which means that only one measurement per child was included in our analyses. Exactly the same examination modules were deployed at baseline (T0) and at follow-up (T1), but only the entry measurement was considered in case of children who participated in both surveys. In addition to the signed informed consent given by parents, each child was asked to give verbal assent immediately before examination. All measurements were approved by the local Ethics Committees.30,31
Overall 18 745 2.0–10.9-year-old children took part in the study. BMI categories were defined according to IOTF13 to classify overweight, obese and underweight children (N=5915, 31.6%) who were excluded, leaving 12 830 normal weight children for the analysis. The number of children with BMI measurements and the exclusion criteria are exemplarily illustrated in Figure 1. Table 1 summarises the sample size for each measurement stratified by sex and by the eight participating countries. As the children were free to opt out of any module of the examination protocol, the number of children providing anthropometric measurements varied for the different measurements, due to different acceptance proportions for each measure (see also Table 1). In addition, not all skinfold measurements were compulsory elements of the examination protocol (see below). Thus, the number of children with all four skinfold measurements is smaller than the number of children for whom the compulsory skinfolds were measured. Only very minor differences were observed comparing the group of children with all four skinfold measurement with the normal weight study population with respect to mean age, sex distribution and distribution of ISCED (International Standard Classification of Education) level where the maximum level of both parents was considered. The distributions of the triceps and subscapular skinfolds did not change significantly if they were calculated from the data of the smaller sample where all four skinfolds were measured.

Flow chart of the inclusion criteria of 2.0–10.9-year-old normal-weight children.
Anthropometric measurements
All anthropometric measurements were carried out by trained research assistants according to the IDEFICS study protocol. The intra- and inter-observer reliability assessment of the anthropometric measurements was considered as good to very good. For details, we refer to the paper recently published by Stomfai et al.32
Weight was measured using an electronic scale (Tanita BC 420 SMA, Tanita Europe GmbH, Sindelfingen, Germany) to the nearest 0.1 kg. The children wore only an underwear and a T-shirt. Height was measured barefooted, using a telescopic height measuring instrument (Seca 225 stadiometer, seca, Birmingham, UK) to the nearest 0.1 cm. Skinfold thickness (mm) was measured twice on the right side of the body to the nearest 0.2 mm with a skinfold calliper (Holtain, range 0–40 mm, Holtain Ltd, Pembrokeshire, UK). Skinfold measurements were taken at the following sites: (1) triceps, halfway between the acromion and the olecranon process at the back of the arm; (2) biceps, at the same level as the triceps skinfold, in the line of the centre of the cubital fossa; (3) subscapular, about 20 mm below the tip of the scapula, at an angle of 45° to the lateral side of the body; (4) suprailiac, about 20 mm above the iliac crest and 20 mm towards the medial line. In the survey, measurements of triceps and subscapular skinfolds were compulsory for each survey centre, whereas those of biceps and suprailiac were optional (see Table 1). Circumferences (cm) were measured once with an inelastic tape (Seca 200), precision 0.1 cm, range 0–150 cm, with the child in a standing position. Circumference measurements were taken at four sites: arm, waist, hip and neck.32 NC was measured when the child stood upright, head being in Frankfort plane,33 and with the arms at the sides and feet together. The tape was placed around the neck at a point just above the larynx and perpendicular to the long axis of the neck. The measurement of WC was obtained in upright position with relaxed abdomen and feet together, midway between the lowest rib margin and the iliac crest to the nearest 0.1 cm.
Calculation of anthropometric indices
BMI was calculated dividing the body weight in kilograms by the square of body height in metres. Waist-to-height ratio was computed dividing WC by height, both in centimetres.
Body fat mass
Biceps, triceps, subscapular and suprailiac skinfolds were added up to calculate the sum of skinfolds. For the calculation of body fat mass (BFM) from skinfolds, several equations exist worldwide34, 35, 36, 37, 38, 39, 40, 41, 42 for adults and children. Slaughter’s equations39 are preferred for predicting BFM in children.43, 44, 45, 46 Besides their wide acceptance Slaughter’s equations also have the advantage of requiring only two anthropometric measures. We applied these formulas using the sum of subscapular (mm) and triceps (mm) skinfold thicknesses (x) for boys as follows

and for girls

aged between 2.0 and 10.9 years. The FMI was calculated by dividing BFM by the square of height in metres.
Statistical analysis
We calculated percentile curves of the anthropometric measures as a function of age (continuous) stratified by sex using GAMLSS. The GAMLSS method is an extension of the LMS method that models three parameters depending on one explanatory variable: the median (M) of the outcome variable is modelled depending on one explanatory variable and the coefficient of variation (S) accounts for the variation around the mean and adjusts for nonuniform dispersion, whereas the skewness (L) accounts for the deviation from a normal distribution using a Box–Cox transformation. The GAMLSS method is able to particularly model the kurtosis using other distributions and to include more than one covariate. We used the gamlss package (version 4.2–6) of the statistical software R (version 3.0.1). Different distributions, that is, the Box–Cox power exponential, the Box–Cox t or the Box–Cox Cole and Green distribution were fitted to the observed distribution of the anthropometric outcome variables. Moreover, the influence of age (continuous) on parameters of the considered distributions was modelled either as a constant, as a linear function or as a cubic spline of the covariate. Goodness of fit was assessed by the Bayesian Information Criterion and Q–Q plots to select the final model including the fitted distribution of the anthropometric outcome variable and the influence of covariates on distribution parameters.28,29 Worm plots47,48 were used as a diagnostic tool to assess whether adjustment for kurtosis was required. The chosen GAMLSS in boys and girls are listed in Table 2, for example, the final model for waist-to-height ratio in boys consists of a Box–Cox t distribution, where the four parameters were modelled as follows: the location parameter μ as a cubic spline, the scale parameter log(σ) linearly and the shape parameters ν and log(τ) as constants. The chosen models of the anthropometric outcome variables were used to calculate percentile curves for the 1st, 3rd, 10th, 25th, 50th, 75th, 90th, 97th and 99th percentiles. Percentile cutoffs are presented by 0.5-year group in tables.
Results
Body mass index
In 4.5- to <5.0-year-old girls and boys, the 50th and 99th percentiles were 15.5 and 17.2 kg m−2 and 15.6 and 17.3 kg m−2. At the age of 10.5–10.9 years, the corresponding percentiles in girls were 16.9 and 20.1 kg m−2 and 16.8 and 20.1 kg m−2 in boys (Supplementary Table A and Supplementary Figure A). Our curves showed a BMI rebound between 5 and 6.5 years of age for girls and boys.
Skinfolds
Girls showed higher skinfold thicknesses than boys. All skinfolds showed a positive trend with age in girls. In boys this trend was slightly negative until the age of 5–6 years and positive thereafter (Supplementary Tables B–E and Supplementary Figures B–E).
Biceps skinfold
The 50th and 99th percentiles of biceps skinfolds in 4.5- to <5.0-year-old girls were 5.7 and 10.8 mm, and in boys 5.1 and 9.2 mm. The corresponding percentiles at the age of 10.5–10.9 years were 6.2 and 14.1 mm in girls and 5.3 and 19.8 mm in boys, respectively.
Triceps skinfold
In 4.5- to <5.0-year-old girls and boys, the 50th and 99th percentiles were 10.7 and 17.1 mm and 9.2 and 15.1 mm, respectively. At the age of 10.5–10.9 years, the corresponding percentiles were 13.1 and 26.6 mm in girls and 10.5 and 24.6 mm in boys.
Subscapular skinfold
For subscapular skinfolds, the 50th and 99th percentiles in 4.5- to <5.0-year-olds were 6.1 and 11.1 mm in girls and 5.5 and 9.6 mm in boys, respectively. At the age of 10.5–10.9, in girls, the corresponding percentiles were 7.6 and 20.3 mm; in boys, they were 6.2 and 14.8 mm, respectively.
Suprailiac skinfold
The 50th and 99th percentiles in 4.5- to <5.0-year-old girls and boys were 5.6 and 13.3 mm and 4.6 and 10.5 mm, respectively. At the age of 10.5–10.9 years, these percentiles were 7.1 and 27.8 mm in girls and 6.2 and 20.2 mm in boys.
Sum of skinfolds
The sum of skinfolds showed a positive trend with age in girls, whereas in boys there was a slight negative age trend until the age of 6 years, followed by a positive trend thereafter (Table 3 and Figure 2). The 50th and 99th percentiles at the age of 4.5–5.0 years were 28.0 and 46.0 mm in girls, 24.3 and 40.3 mm in boys, whereas in the 10.5–10.9-year-olds it was 36.6 and 90.2 mm in girls and 28.8 and 78.9 mm in boys.

Percentile curves of sum of skinfolds in normal-weight European girls and boys.
Body fat mass
The 50th and 99th percentiles for BFM in 4.5- to <5.0-year-old girls and boys were 16.2 and 23.5 and 14.4 and 22.0%, respectively. At the age of 10–10.9 years, these percentiles were 19.6 and 35.2% in girls and 16.3 and 36.9% in boys (Supplementary Table F and Supplementary Figure F).
Fat mass index
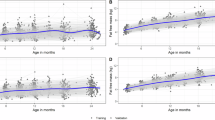
The smoothed percentile curves of FMI for girls and boys are shown in Table 4; Figure 3. FMI showed a continuously negative age trend both in girls and boys, the latter having constantly lower values. However, in boys a slight increase in the upper percentiles (97th and 99th) was observed from the age of 9.5 years onwards. The 50th and 99th percentiles in 4.5- to <5.0-year-old children were 13.8 and 20.7 in girls and 12.0 and 18.9 in boys; and 9.6 and 16.1, and 7.9 and 16.0 in 10.5–10.9-year-old girls and boys, respectively.

Percentile curves of fat mass index in normal-weight European children girls and boys.
Waist circumference
WCs showed a positive trend with age with slightly higher values in boys than in girls (Table 5 and Figure 4). The 50th and 99th percentiles of WC ranged from 50.7 and 59.2 cm and 51.3 and 58.7 cm in 4.5- to <5.0-year-old girls and boys, respectively to 60.6 and 74.5 cm in girls and to 59.9 and 76.7 cm in boys at the age of 10.5–10.9 years.

Percentile curves of waist circumference in normal-weight European girls and boys.
Waist-to-height ratio
The waist-to-height ratio showed a declining trend by age in both sexes (Table 6 and Figure 5). In terms of percentiles there was no major difference between the sexes. The 50th and 99th percentiles of waist-to-height ratio in the age group 4.5 to <5.0 years were 0.47 and 0.52 in girls and 0.47 and 0.53 in boys, whereas in the age group 10.5–10.9 years the 50th and 99th percentiles of waist-to-height ratio were 0.42 and 0.51 in girls and 0.42 and 0.50 in boys.

Percentile curves of waist-to-height ratio in normal-weight European girls and boys.
Neck circumference
The age-dependent changes in the percentiles in boys and girls are illustrated in Table 7 and Figure 6. The values showed a positive trend until the age of 8.5 years in both sexes, then the curves levelled off. The 50th and 99th percentile values in 4.5- to <5.0-year-old girls were 24.7 and 27.9 cm, in boys the corresponding values were 27.6 and 28.8 cm. At the age of 10.5–10.9 years, the 50th and 99th percentile values were 27.6 and 31.1 cm in girls, while in boys the values were 28.8 and 31.8 cm.

Percentile curves of neck circumference in normal-weight European girls and boys.
The percentile curves of the examined anthropometric variables including underweight, overweight and obese children and the corresponding tables are available online (Supplementary Figures G–Q, Supplementary Tables G–Q). In addition, the sample sizes for the total population analogously to Table 1 and the fitted models analogously to Table 2 are available online (Supplementary Tables R and S).
Discussion
The present paper provides age- and sex-specific reference percentiles for standard anthropometric parameters and indices obtained in children from eight European countries, contributing to the IDEFICS cohort. To the authors’ knowledge, there are no previous studies establishing reference values for anthropometric parameters from such a large sample of normal weight children spanning a wide geographical range across Europe.
It was our main goal to provide reference anthropometric values of normal weight European children which is supported by the ambitions of the WHO. While creating growth charts for children aged 0–71 months, the following was stated:49 ‘To avoid the influence of unhealthy weights for length/height, observations falling above +3 s.d. and below −3 s.d. of the sample median were excluded before constructing the standards. For the cross-sectional sample, the +2 s.d. cutoff (that is, 97.7 percentile) was applied instead of +3 s.d.’. Only children receiving optimal feeding practice and living in a supporting environment were eligible.
In addition, we would like to stress that this approach is similar to the approach used when the results of longitudinal follow-up surveys and panel studies (FELS, NHANES) are compared with those reference standards obtained at the beginning of the survey, thus avoiding the cohort effect of growing obesity epidemic. By restricting our sample to the normal weight population, we expand this approach. As reference values are expected to reflect as much as possible the biological variation in a disease free population, it was a logical methodological consideration to exclude underweight, overweight and obese individuals from the analysis group.
Figure 7 exemplarily demonstrates how the inclusion of overweight and obese children shifts the percentile values of waist circumference (especially in the higher percentile range) grossly upwards, indicating that the restriction of the sample to normal weight children was a logical decision.

Percentile curves of waist circumference in girls and boys based on all children and for normal-weight children only.
There are numerous national anthropometric reference values for WC,18,20, 21, 22, 23, 24,50 waist-to-height ratio,51 skinfold thicknesses,15,16,52 sum of skinfolds,53 BFM54,55 and FMI.7,56 As these data are based on samples including underweight, overweight, as well as obese children, they cannot be directly compared with our results. Due to the restriction of our sample to normal-weight children, generally the upper percentiles of the present study tend to fall below those of above-mentioned reference studies whereas the lower percentiles tend to exceed them.
The few papers investigating normal-weight children’s anthropometric data were focusing on neck and WCs.
Waist circumference
In adults, WC is widely used as a surrogate of central fat distribution, but in children it may be influenced by growth and puberty, reducing its accuracy in estimating visceral adipose tissue.57 Brambilla et al.57 assessed the relationship between anthropometry and visceral adipose tissue and subcutaneous adipose tissue as measured by magnetic resonance imaging in children aged 7–16 years. They found that WC can be considered a good predictor of abdominal adiposity referring to its relationship with visceral adipose tissue measured by magnetic resonance imaging, one of the most precise methods of assessing visceral adiposity.
Mellerio et al.58 established percentile reference data of WC for 7–20-year-old (N=1976, 1004 female and 972 male participants) healthy children and young adults in France. Their noninclusion criteria were rather similar to those used in this examination. Individuals with obesity or at least grade 2 thinness were excluded. The following percentile values were estimated based on their graphical presentation. The 50th and 90th percentiles were 55.0 and 62.0 cm in 8.0- to <8.5-year-old girls and 57.0 and 64.0 cm in boys, respectively. In our population, the 50th and 90th percentiles were 55.5 and 60.8 cm in girls and 56.3 and 61.2 cm in boys of the same age. The observed differences between the studies may be due to that overweight children were not excluded in the French study. The positive trend with age is similar in the two studies and the WC was lower in girls than in boys in both studies.
A study conducted in Turkey measured WC of 7–17-year-old children (N=4770, 2433 boys, 2337 girls).20 In this study children exceeding the 97th percentile of body weight were excluded (that is, only obese), but in contrary to our study, underweight children remained included. In both age strata and both sexes, our 50th percentile values are higher whereas our 90th percentiles are lower as compared with the Turkish study with the exception of 10-year-old boys where the 50th percentile is also lower in our study. In both studies the WC was lower in girls than in boys. The magnitude of difference in the 90th percentile values ranged from 0.4–1.4 cm in girls and from 1.9–4.7 cm in boys. The differences can be explained by the different exclusion criteria (overweight children were included and underweight children were not excluded from the Turkish study).
Fernandez et al.59 established reference values for WC in European–American children, underweight, overweight and obese children were not excluded from this sample. In girls, both the 50th and 90th percentile values of WC were lower in the IDEFICS sample as compared with the European–American population. The largest difference was 10.9 cm in the 90th percentile value at the age of 11.
In boys, with the exception of the 50th and 90th percentile, values were lower in the IDEFICS population. The maximum difference (14.9 cm) was observed at the age of 11 for the 90th percentile value. From this comparison it becomes obvious that the European–American WC values should not directly be applied to a European population.
Neck circumference
NC can be an additional measure to identify children with overweight and obesity as suggested by Nafiu et al.60 Hatipoglu et al.,61 validating the NC against WC and BMI, also reported that the NC is an easy way to determine overweight and obesity in children, demonstrating good correlation with cardiovascular risk markers. NC has advantages over WC. Especially busy primary care settings can benefit from the omission of the need to undress. Moreover, NC is not influenced by pre- and postprandial effects.59
NC was measured in 5841 6–18-year-old children in Turkey during 2008 to 2009.17 Children below the 3rd and above the 97th percentile of body weight were excluded from the analysis. The 50th and 90th NC values showed little differences between the two studies with slightly higher values in the IDEFICS sample, except the 90th percentile value of girls, which was 0.6 cm higher in the Turkish sample. The largest difference between the two studies was 6.5% in boys and 6.3% in girls.
Height, weight and BMI are pragmatic measures to screen for obesity or underweight and to assess the nutritional status of children, for example, with regard to stunting and wasting. To overcome the well-known limitations of BMI, additional anthropometric parameters and indices referring to body fat content and distribution are also recommended. To the best of our knowledge, such standards for European children have not been published so far. The main strengths of our study are the size of the cohort and the wide geographical scope covered. In addition, the most meticulous standardization of measurements and subsequent procedures for quality control were applied. The general limitations of the IDEFICS study were extensively discussed in a previous paper.31 Here we discuss those which might be relevant to the present paper. The participation proportion was just above 50% and a non-response bias towards higher or lower social classes might be present. Socioeconomic factors influence the prevalence of obesity and thinness, but obese and underweight children were excluded from our analysis, therefore this limitation should not have a major effect on our results. Pubertal stages were not assessed. Some of the older children may have entered puberty at the time of their examination. Body composition changes during puberty but since we wanted to provide age-specific reference values for the whole population non-consideration of pubertal development is a strength rather than a limitation.
Conclusion
The presented reference values may improve the interpretation of anthropometric measurements in the context of routine medical practice. The measurement of skinfold thickness, sum of skinfolds, BFM, waist and neck circumference, and the calculation of FMI and waist-to-height ratio may refine the individual evaluation of the nutritional status of children, and serve as a useful tool for public health screening with regard to European children. They may also allow comparisons of future national and international epidemiological studies, as well as the prevention and recognition of malnutrition, overweight and obesity at an early age.
References
Srinivasan SR, Berenson GS . Relation of circumferences and skinfold thicknesses to lipid and insulin concentrations in children and adolescents: the Bogalusa Heart Study 1.2.3. Am J Clin Nutr 1999; 2: 308–317.
Adaki ACR, Tinico ALA, Mendes EL, Junior RA, Hills AP, Amorim PRS . Anthropometry and physical activity level in the prediction of metabolic syndrome in children. Public Health Nutr 2013; 24: 1–8.
Revenga-Frauca J, González-Gil EM, Bueno-Lozano G, De Miguel-Etayo P, Velasco Martínez P, Rey-López JP et al. Abdominal fat and metabolic risk in obese children and adolescents. J Physiol Biochem 2009; 4: 415–420.
Rose G . Incubation period of coronary heart disease. Int J Epidemiol 2005; 34: 242–244.
Wells JC, Fewtrell MS . Measuring body composition. Arch Dis Child 2006; 7: 612–617.
Wells JCK, Fewtrell MS . Is body composition important for paediatricians? Arch Dis Child 2008; 93: 168–172.
Wells JC, Williams JE, Chomtho S, Darch T, Girjalva-Eternod C, Kennedy K et al. Body-composition reference data for simple and reference techniques and 4-component model: a new UK reference child. Am J Clin Nutr 2012; 6: 1316–1326.
Westrate JA, Deurenberg P . Body composition in children: proposal for a method for calculating body fat percentage from total body density or skinfold-thickness measurements. Am J Clin Nutr 1989; 5: 1104–1115.
Moreno LA, Fleta J, Mur L, Feja C, Sarria A, Bueno M . Indices of body fat distribution in Spanish children aged 4.0 to 14.9 years. J Paediatr Gastroenterol Nutr 1997; 25: 175–181.
Sarría A, Moreno LA, García-Llop LA, Fleta J, Bueno M . Body mass index. triceps skinfold and waist circumference in screening for adiposity in male children and adolescents. Acta Paediatr 2001; 90: 387–392.
Moreno LA, Pineda I, Rodríguez G, Fleta J, Sarría A, Bueno M . Waist circumference for the screening of the metabolic syndrome in children. Acta Paediatr 2002; 91: 1307–1312.
Wells JCK . A Hattori chart analysis of body mass index in infants and children. Int J Obes 2000; 24: 325–329.
Cole TJ, Lobstein T . Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes 2012; 4: 284–294.
Wells JCK, Fewtrell MS, Williams JE, Haroun D, Lawson MS, Cole TJ . Body composition in normal weight, overweight and obese children: matched case-control analysis of total and regional tissue masses, and body composition trends in relation to relative weight. Int J Obes 2006; 30: 1506–1513.
Moreno LA, Fleta J, Mur I, Feja C, Sarria A, Bueno M . Indices of body fat distribution in Spanish children aged 4.0 to 14.9 years. J Pediatr Gastroenterol Nutr 1997; 25: 175–181.
Jawrowski M, Kulaga Z, Pludowsky P, Grajda A, Gurcowska B, Napieralska E et al. Population-based centile curves for triceps. subscapular and abdominal skinfold thicknesses in Polish children and adolescents-the OLAF Study. Eur J Pediatr 2012; 171: 1215–1221.
Maziczioglu MM, Kurtoglu S, Ozturk A, Hatipoglu N, Ustunbas HB . Percentiles and mean values for neck circumference in Turkish children aged 6-18 years. Acta Paediatr 2010; 12: 1847–1853.
McCarthy HD, Jarrett KV, Crawley HF . The development of waist circumference percentiles in British children aged 5.0-16.9 y. Eur J Clin Nutr 2001; 55: 902–907.
Haas GM, Liepold E, Schwandt P . Percentile curves for patterning in German adolescents. World J Pediatr 2011; 7: 16–23.
Hatipoglu N, Ozturk A, Mazicioglu MM, Kurtoglu S, Seyhan S, Lokoglu F . Waist circumference percentiles for 7-17-year-old Turkish children and adolescents. Eur J Ped 2007; 4: 383–389.
Frideriks AM, van Buuren S, Fekkes M, Verloove-Vanhorick SP, Wit JM . Are age references from waist circumference. hip circumference and waist-to-hip ratio in Dutch children useful in clinical practice? Eur J Pediatr 2005; 164: 216–222.
Galcheva SV, Iotova VM, Yotov YT, Grodzeva KP, Stratev VK, Tzaneva VI . Waist circumference percentile curves for Bulgarian children and adolescents aged 6-18 years. Int J Ped Obes 2009; 4: 381–388.
Savva SC, Tornaritis M, Savva ME, Kourides Y, Panagi A, Silikiotou N et al. Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors than body mass index. Int J Obes Relat Metab Disord 2000; 24: 1453–1458.
Brambilla P, Begdoni G, Heo M, Pietrobelli A . Waist circumference-to-height ratio predicts adiposity better than body mass index in children and adolescents. Int J Obes 2013; 37: 943–946.
Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Guo SS, Wei R et al. CDC growth charts: United States. Adv Data 2000; 314: 1–27.
Shields M, Tremblay MS . Canadian childhood obesity estimates based on WHO. IOTF and CDC cut points. Int J Pediatr Obes 2010; 3: 265–273.
Australian Paediatric Endocrine Group (APEG). Australian and New Zealand Growth Charts, 2014. http://www.apeg.org.au/clinicalresourceslinks/growthgrowthcharts/tabid/101/default.aspx (last access April 2014).
Rigby RA, Stasinopoulos DM . Generalized additive models for location, scale and shape. J R Stat Soc Series C Appl Stat 2005; 3: 507–554.
Stasinopoulos DM, Rigby RA . Generalized additive models for location, scale and shape (GAMLSS) in R. J Stat Softw 2007; 7: 1–46.
Ahrens W, Bammann K, Siani A, Buchecker K, De Henauw S, Iacoviello L et al. IDEFICS Consortium. The IDEFICS cohort: design, characteristics and participation in the baseline survey. Int J Obes (Lond) 2011; 35 (Suppl 1): S3–S15.
Lanfer A, Hebestreit A, Ahrens W, Krogh V, Sieri S, Lissner L et al. IDEFICS consortium. Reproducibility of food consumption frequencies derived from the Children's Eating Habits Questionnaire used in the IDEFICS study. Int J Obes 2011; 35 (Suppl 1): S61–S68.
Stomfai S, Ahrens W, Bammann K, Kovacs E, Marild S, Michels N et al. IDEFICS Consortium. Intra- and interobserver reliability in anthropometric measurements in children. Int J Obes 2011; 35 (Suppl 1): S45–S51.
Chang HP . Assessment of anteroposterior jaw relationship. Am J Orthodont and Dentofac Orthop 1987; 92: 117–122.
Durnin JV, Womersley J . Body fat assessed from total body density and its estimation from skinfold thickness measurements on 481 men and women aged 16–72 years. Br J Nutr 1974; 32: 77–97.
Deurenberg P, Pieters JJL, Hautvast JG . The assessment of the body fat percentage by skinfold thickness measurements in childhood and young adolescence. Br J Nutr 1990; 63: 293–303.
Sarrıa A, Garcıa-Llop LA, Moreno LA, Fleta J, Morello MP, Bueno M . Skinfold thickness measurements are better predictors of body fat percentage than body mass index in male Spanish children and adolescents. Eur J Clin Nutr 1998; 52: 573–576.
Sloan AW, Burt JJ, Blyth CS . Estimation of body fat in young women. J Appl Physiol 1962; 17: 967–970.
Wilmore JH, Behnke AR . An anthropometric estimation of body density and lean body weight in young women. Am J Clin Nutr 1970; 23: 267–274.
Slaughter MH, Lohman TG, Boileau RA, Horswill CA, Stillman RJ, van Loan MD et al. Skinfold equations for estimation of body fatness in children and youths. Hum Biol 1988; 60: 709–723.
Lean MEJ, Han TS, Deurenberg P . Predicting body composition by densitometry from simple anthropometric measurements. Am J Clin Nutr 1996; 63: 4–14.
Bray GA, DeLany JP, Harsha DW, Volaufova J, Champagne CC . Evaluation of body fat in fatter and leaner 10-y-old African American and white children: the Baton Rouge Children’s Study. Am J Clin Nutr 2001; 73: 687–702.
de Ridder CM, de Boer RW, Seidell JC, Nieuwenhoff CM, Jeneson JA, Bakker CJ et al. Body fat distribution in pubertal girls quantified by magnetic resonance imaging. Int J Obes 1992; 16: 443–449.
Eisenmann JC, Heelan KA, Welk GJ . Assessing body composition among 3- to 8-year-old children: anthropometry, BIA, and DXA. Obes Res 2004; 12: 1633–1639.
Treuth MS, Butte NF, Wong WW, Ellis KJ . Body composition in girls: comparison of six methods. Int J Obes 2001; 25: 1352–1359.
Freedman DS, Horlick M, Brenson GS . A comparison of Slaughter skinfold-thickness equations and BMI in predicting body fatness and cardiovascular disease risk factor levels in children. Am J Clin Nutr 2013; 98: 1417–1424.
Silva DR, Riberio AS, Pavao FH, Rongue ER, Avelar A, Silva AM et al. Validity of the methods to assess body fat in children and adolescents using multi-compartment models as the reference method: a systematic review. Rev Assoc Med Bras 2013; 59: 475–486.
van Buuren S, Fredriks AM . Worm plot: a diagnostic device for modelling growth reference curves. Stat Med 2001; 20: 1259–1277.
Cole TJ, Stanojevic S, Stocks J, Coates AL, Hankinson JL, Wade AM . Age- and size-related reference ranges: a case study of spirometry through childhood and adulthood. Stat Med 2009; 28: 880–898.
WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Pædiatr Suppl 2006; 450: 76–85.
Moreno LA, Fleta J, Mur L, Rodriguez G, Sarria A, Bueno M . Waist circumference values in Spanish children-Gender related differences. Eur J Clin Nutr 1999; 53: 429–433.
Sung RYT, So HK, Choi KC, Nelson EAS, Li AM, Yin JAT et al. Waist circumference and waist to height ratio of Hong Kong Chinese children. BMC Public Health 2008; 8: 324.
Addo OY, Himes JH . Reference curves for triceps and subscapular skinfold thicknesses in US children and adolescents. Am J Clin Nutr 2010; 91: 635–642.
Abdulrazzaq YM, Nagelkerke N, Moussa MA . UAE population reference standards for body mass index and skinfold thickness at ages 0-18 years. Int J Food Sci Nutr 2011; 6: 692–702.
Scwandt P, von Eckardstein A, Haas GM . Percentiles of percentage body fat in German children and adolescents: an international comparison. Int J Prev Med 2012; 12: 846–852.
Laurson KR, Eisenmann JC, Welk GJ . Body fat percentile curves for U.S. children and adolescents. Am J Prev Med 2011; 41 (4 Suppl 2): S87–S92.
Khadilkar AV, Sanwalka NJ, Chiplonkar SA, Khadilkar VV, Pandit D . Body fat reference percentiles on healthy affluent Indian children and adolescents to screen for adiposity. Int J Obes 2013; 37: 947–953.
Brambilla P, Bedogni G, Moreno LA, Goran MI, Gutin B et al. Crossvalidation of anthropometry against magnetic resonance imaging for the assessment of visceral and subcutaneous adipose tissue in children. Int J Obes 2006; 30: 23–30.
Mellerio H, Alberti C, Druet C, Capelier F, Mercat I, Josserand E et al. Novel modeling of reference values of cardiovascular risk factors in children aged 7 to 20 years. Pediatrics 2012; 129: e1020–e1029.
Fernandez JR, Redden DT, Pietrobelli A, Allison DB . Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J Pediatr 2004; 145: 439–444.
Nafiu OO, Burke C, Lee J, Voepel-Lewis T, Malviya S, Tremper KK . Neck circumference as a screening measure for identifying children with high body mass index. Pediatrics 2012; 126: e306–e310.
Hatipoglu N, Mazicioglu MM, Kurtoglu S, Kendirci M . Neck circumference: an additional tool of screening overweight and obesity in childhood. Eur J Ped 2010; 169: 733–739.
Acknowledgements
This work was done as part of the IDEFICS Study (www.idefics.eu). We gratefully acknowledge the financial support of the European Community within the Sixth RTD Framework Programme Contract No. 016181 (FOOD). IS is financially supported by the Research Foundation—Flanders (Grant no: 1.2.683.14.N.00). We are grateful to the Volkswagen Foundation that financially supported the production of this supplement. LL has received grant support from VR, FORTE and FORMAS (research councils in Sweden).
DISCLAIMER
The information in this document reflects the author's view and is provided as is.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on International Journal of Obesity website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Nagy, P., Kovacs, E., Moreno, L. et al. Percentile reference values for anthropometric body composition indices in European children from the IDEFICS study. Int J Obes 38 (Suppl 2), S15–S25 (2014). https://doi.org/10.1038/ijo.2014.131
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2014.131
This article is cited by
-
Pregnancy homocysteine and cobalamin status predict childhood metabolic health in the offspring
Pediatric Research (2023)
-
Genetic associations vary across the spectrum of fasting serum insulin: results from the European IDEFICS/I.Family children’s cohort
Diabetologia (2023)
-
Establishing international optimal cut-offs of waist-to-height ratio for predicting cardiometabolic risk in children and adolescents aged 6–18 years
BMC Medicine (2023)
-
Media use trajectories and risk of metabolic syndrome in European children and adolescents: the IDEFICS/I.Family cohort
International Journal of Behavioral Nutrition and Physical Activity (2021)
-
Trajectories of objectively measured physical activity and childhood overweight: longitudinal analysis of the IDEFICS/I.Family cohort
International Journal of Behavioral Nutrition and Physical Activity (2021)
