
Abstract
Purpose
We investigated the influence of H. pylori infection on intraocular pressure (IOP) in anterior uveitis patients to clarify whether H. pylori infection is related to high IOP in anterior uveitis.
Methods
In this prospective study, 165 Korean anterior uveitis patients were examined. All patients underwent serological analysis to identify the cause of uveitis, including the presence of H. pylori infection by enzyme-linked immunosorbent assay. Serological values were compared between patients with and without high IOP.
Results
Seropositivity for H. pylori was 69.70% of patients with high IOP and 38.38% of patients with normal IOP (P<0.01).
Conclusion
This study suggests that H. pylori infection is associated with high IOP in anterior uveitis.
Similar content being viewed by others

Introduction
Uveitis may cause elevated or reduced intraocular pressure (IOP). Anterior uveitis is the most common form of intraocular inflammation; it is also the most common cause of high IOP in uveitis.1 Well-known causes of increased IOP are herpetic anterior uveitis, Posner–Schlossman syndrome, sarcoid uveitis, toxoplasmic retinochoroiditis, listeria endophthalmitis, syphilitic uveitis, cytomegalovirus infection, HLA-B27-associated uveitis, and others.2 Several mechanisms may be involved in the pathogenesis of increased IOP in the presence of inflammation, including obstruction of the trabecular meshwork by inflammatory cells and proteins by breakdown of the blood–ocular barrier,3 trabeculitis,4 formation of peripheral anterior synechiae, posterior synechiae,1 neovascularization,5 anterior displacement of the lens–iris diaphragm,6 and the use of steroids to treat the uveitis.7
Helicobacter pylori (H. pylori) is a common, curved, spiral, Gram-negative bacteria that has been associated with various extradigestive disorders, in addition to its well-known association with gastrointestinal disorders.8, 9, 10, 11 In the past year, several studies have suggested an association between H. pylori infection and various extradigestive diseases, including cardiovascular and immunological disorders. As the release of large amounts of various proinflammatory and vasoactive substances, such as cytokines, eicosanoids, and acute phase reactant proteins follows gastric colonization by H. pylori, the bacterium may be involved in vascular disorders.9, 10, 11, 12, 13, 14 Moreover, several clinical observations suggest a role for H. pylori infection in various immunological disorders. There have been reports of resolution of various autoimmune diseases (such as Henoch–Schonlein purpura, Sjogren’s syndrome, and autoimmune thrombocytopenia) after H. pylori eradication.8, 9, 10 Kountouras et al14 reported the first link between H. pylori infection and glaucoma. These authors suggested H. pylori infection may influence the pathophysiology of glaucoma by releasing various proinflammatory and vasoactive substances.15
In the current study, we investigated the association between H. pylori infection and IOP in Korean anterior uveitis subjects.
Methods
This prospective case–control study included Korean patients with uveitis seen at Kim’s Eye Hospital, Konyang University from July 2009 to April 2010. The study was approved by the ethics committee of the local institutional review board. Participants were enrolled after obtaining written informed consent.
All cases in our study were newly diagnosed as acute unilateral anterior uveitis (AAU), which had not received prior medical treatment and which developed suddenly with the duration of ≤3 months. We used the term ‘Anterior uveitis’ according to the Standardization of Uveitis Nomenclature classification. Anterior uveitis is thus defined as intraocular inflammation primarily involving the anterior chamber. The severity of intraocular inflammation was assessed according to the recommendations of the Standardization of Uveitis Nomenclature Working Group.16 At the initial visit, a detailed ocular and medical history was collected, including demographic characteristics. All participants underwent a complete ophthalmic examination, including funduscopic examination after pupil dilation, at initial evaluation. All subjects with diabetes mellitus, a myopic refractive error exceeding −8 diopters, subjects who have been diagnosed as or treated for uveitis before, or any active eye diseases other than uveitis were excluded. Patients were excluded from this study who had a history of ocular surgery, including laser surgery, or treatment for ocular trauma, glaucoma or ocular hypertension, narrow angle, large peripheral anterior synechiae (>90 degree), or retinal disorders. No patients received oral medications that could decrease IOP (eg, carbonic anhydrase inhibitors, systemic beta blocker).
All subjects underwent routine serologic analysis for uveitis, including the presence of H. pylori infection. A total of 165 consecutive anterior uveitis patients from an outpatient glaucoma clinic and uveitis clinic were enrolled. The IOPs were measured with a Goldmann applanation tonometer (Haag-Streit International, Koeniz, Switzerland), and patients with an IOP greater than 22 mm Hg were classified to the anterior uveitis with high-IOP group. The anterior uveitis with high-IOP group included 66 patients, while the anterior uveitis without high-IOP group consisted of 99 patients.
Laboratory tests
Venous samples were obtained from each subject. Anti-H. pylori immunoglobulin G (IgG) levels were determined quantitatively with an enzyme-linked immunosorbent assay (ELISA). Anti-varicella zoster virus (VZV) IgG, herpes simplex virus (HSV) IgG, toxoplasma IgG, and rheumatoid factor (RA) levels were determined in a similar manner. The presence of the HLA-B27 allele was identified by polymerase chain reaction. Anti-nuclear antibody (ANA) and HIV levels were determined by ELISA. Rapid plasma reagin was also evaluated.
H. pylori serologic analysis
The H. pylori serologic analysis status was determined using ELISA (Green Cross Medical Science Corp, Seoul, South Korea); an assay value<15 U/ml was considered negative, and a value ≥15 U/ml was considered positive. The kit in this study used H. pylori antigen obtained from Korean H. pylori strains, and in Korean adults had a sensitivity and specificity of 97.8% and 92.0%, respectively.17
Statistical analysis
A chi-square test was carried out to compare various categorical factors and progression direction among groups. An independent t-test was used to compare continuous factors among groups. Logistic regression analysis was performed for risk factor analysis. Statistical analysis was carried out using the Statistical Package for Social Sciences version 17.0 (SPSS Inc., Chicago, IL, USA). A P-value <0.05 was considered statistically significant.
Results
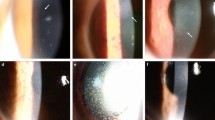
No age or sex differences were observed between with high IOP and without high IOP groups (Table 1). Mean follow-up durations were 34.15±19.75 days in group of uveitis without high IOP and 37.46±24.11 days in group of uveitis with high IOP (P=0.128). No patients had a positive HIV or rapid plasma reagin test. Anterior uveitis patients with a high IOP had significantly more positive H. pylori tests than those without high IOP. Anterior uveitis patients without high IOP had significantly more positive VZV and HSV tests than did those with high IOP. The HLA-B27 allele was detected more frequently in anterior uveitis patients without high IOP. There were no significant differences in positive results of toxoplasma, ANA, and RA levels between the two groups (Table 2, Table 3, Figure 1). To detect the difference between 70% of H. pylori IgG among uveitis patients with high IOP and 40% of H. pylori IgG among uveitis patients without high IOP, we used a two-sided Fisher exact test with an alpha level of 0.05. At a power of 95.8%, there will be 46 uveitis patients with high IOP and 99 without high IOP.

Associations between pathogenic etiologies and IOP in anterior uveitis patients.
Discussion
In the current study, H. pylori were detected more frequently in anterior uveitis patients with high IOP. This suggests that H. pylori infection may have a role in increasing IOP in anterior uveitis patients, though a potential causative role for H. pylori in anterior uveitis is not clear. In anterior uveitis patients without high IOP, VZV, HSV, and HLA-B27 were detected more frequently. There were no significant differences in toxoplasma, ANA, or RA levels between the groups.
Although the cause of AAU is not clearly known, both genetic and exogenous factors are thought to have an important role in the development of AAU. In more than 50% of AAU patients, uveitis is associated with the presence of HLA-B27 antigen.18 In addition, gram-negative bacteria, such as Klebsiella, Salmonella, Shigella, Yersinia, and Chlamydia have been suggested to be involved in the pathophysiology of AAU.19, 20, 21, 22
In general, during uveitis, the blood–ocular barrier is broken down following the influx of immunocompetent cells, inflammatory materials, and proteins. These mediators, including cytokines and chemokines, are thought to have a major impact on secondarily elevating IOP. However, the acute increase in pressure in the early stages of uveitis may be due to inflammation of the trabecular meshwork.23
Previous studies have shown that the effects of H. pylori infection on glaucoma.14, 24, 25, 26 Kountouras et al14 noted that patients with glaucoma had a high frequency of H. pylori infection, and that there was a beneficial effect of H. pylori eradication upon glaucoma progression, suggesting a possible causal link between H. pylori and glaucoma.
According to their interpretation, if H. pylori exists in or an immunologic response to H. pylori, or has a harmful effect on, the trabecular meshwork, a decreased outflow capacity induced by inflammation may cause ocular hypertension and glaucoma. Choi et al27 suggested that one of the causes of high IOP in glaucomatocyclitic crisis may be H. pylori.
This present study relied on serological analysis for documentation of H. pylori infection. Serological testing by ELISA permits detection of prior exposure by measuring antibody levels and provides excellent sensitivity and specificity.28 Although ELISA requires sampling of blood and does not discriminate between current and prior infection, this method is inexpensive, quick to perform, and known to be a sensitive and specific test in most populations;24 thus, we selected serological analysis as an effective method readily acceptable to study participants. As serological testing by ELISA is useful in detecting exposure to chronic infections, given that most patients remain seropositive after treatment, if H. pylori exposure or the presence of H. pylori IgG increase the risk of increased IOP, serological testing for IgG is more likely to reflect evidence of a risk factor than other tests specific for acute infection or prior infections. Possible alternative tests for diagnosing H. pylori infection include endoscopy and the urea breath test. Endoscopy is associated with potential complications, discomfort, and considerable expense. The urea breath test has sensitivity and specificity comparable to those of endoscopy29 and is less expensive; they are also noninvasive and global in nature. However, the urea breath test is limited in its ability to detect H. pylori infection. To consider causative mechanisms, such as immunological reactions, we regarded serological tests as more appropriate for use in the current study.
Prevalence of H. pylori infection has been known to vary by country, ethnicity, place of birth, and by socioeconomic factors among people living in the same country.30 In Korea, 56% of the 15 916 population-based subjects were seropositive for anti-H. pylori IgG in a study done in 2005, but the prevalence of asymptomatic subjects was less in a study done in 1998 (59.6% vs 66.9%).31, 32
Many possible mechanisms regarding uveitis and increased IOP related to H. pylori have been proposed. Antigenic similarities,33 cross mimicry with Lewis X antigen,34 and autoimmune reactions35 are possible mechanisms of uveitis caused by H. pylori. As the nature of H. pylori stimulating reactive oxygen metabolite production in gastric mucosa,36, 37 oxidative stress in the trabecular meshwork by H. pylori can also induce decreased outflow capacity and increased IOP. With regard to potential autoimmune reactions, H. pylori infection induces humoral and cellular immune responses following activation of macrophages and produces proinflammatory cytokines (including a variety of interleukins).14 These cytokines can be released into the aqueous humor of patients with anterior uveitis and may lead to increased IOP.
In the current study, the HLA-B27 allele was present at a low level in the uveitis with high-IOP group. HLA-B27 and some Gram-negative bacteria share a common cross-reactive peptide.38, 39, 40 Antigen similarities between bacteria and host can lead to the development of uveitis. This mechanism may be a cause of anterior uveitis; however, the relationship between IOP and bacterial infection in anterior uveitis patients is not clear. To elucidate whether bacterial infection has a causal role in increased IOP, further studies are required.
H. pylori is a systemic problem; however, uveitis is a localized disease. The exact causal mechanism can be difficult to explain, especially in unilateral cases. H. pylori itself may cause direct effects on uveitis and increasing IOP. In this potential mechanism, the route of infection may be external, often traveling from mouth to hand to eye.41 Verification of this mechanism is difficult, and may be not very likely. Secondary effects are more plausible. H. pylori and/or its antibodies circulate in the blood and may eventually enter the anterior chamber through breakdown of the blood–aqueous barrier in eyes affected by uveitis. Alternately, preexisting H. pylori or its antibodies can act after triggering uveitis, contributing to secondary aggravating effects that cause decreased outflow capacity and increased IOP.
In the current study, HSV was more prevalent in the low-IOP group, which differs from some reports.42, 43, 44 We selected our subjects from newly diagnosed patients. So the results could have been different if patients who had a relapse were selected. Falcon and Williams45 suggested that the patients in their study had suffered from recurrent HSV disease before presenting with high IOP, and the consequences of prior damage to the trabecular meshwork might be the cause of the increasing IOP.46 Another point is the growth of H. pylori and HSV can be mitigated by serological interaction between each organism. However, this was not determined by the current study. Tsamakidis et al47 showed that there was an inverse association between HSV-1 and H. pylori infection in patients with gastrointestinal tract ulcers. However, Baccaglini et al48 suggested that HSV-1 seropositivity was associated with a higher H. pylori seroprevalence. Ethnic differences can be also relevant. Further study is required.
The present study has several limitations. We could not identify a causal role of H. pylori infection in the pathogenesis of uveitis and high IOP. Also, we measured only seropositivity of H. pylori infection. As previously mentioned, we believe that serological methods for detecting H. pylori are sufficient for our study, and we excluded patients who had undergone eradication therapy for H. pylori infection. Additionally, we assessed the nature of the association between H. pylori infection and uveitis by cross-sectional analysis, which could not determine a temporal relationship between the two. Patients who had anti-inflammatory or IOP-lowering treatment were excluded to avoid inaccurate comparisons. It should be kept in mind that the exclusion criteria for patient selection can act to create a bias. Also, we did not demonstrate proof of the presence of H. pylori in the trabecular meshwork or aqueous humor. If we demonstrated proof of H. pylori in human eyes, these results have more relevance. As this study analyzed only anterior uveitis patients, our findings may not be relevant to patients with intermediate or posterior uveitis. In this study, the patients with narrow angle were excluded to analysis. We did not analyze the effects of anterior angle states on increased IOP phase. If we provided that, it would enhance our study. Finally, subjects of this study were hospital-based; further population-based studies are required.
In conclusion, we found an association between H. pylori infection and increased IOP in anterior uveitis patients. H. pylori may have a role in uveitis with high IOP as a secondary contributing factor. To fully elucidate whether H. pylori has a role in causing increased IOP in uveitis patients, further studies are required.

References
Moorthy RS, Mermoud A, Baerveldt G, Minckler DS, Lee PP, Rao NA . Glaucoma associated with uveitis. Surv Ophthalmol 1997; 41 (5): 361–394.
Siverio CD, Imai Y, Cunningham ET . Diagnosis and management of herpetic anterior uveitis. Int Ophthalmol Clin 2002; 42 (1): 43–48.
Ladas JG, Yu F, Loo R, Davis JL, Coleman AL, Levinson RD et al. Relationship between aqueous humor protein level and outflow facility in patients with uveitis. Invest Ophthalmol Vis Sci 2001; 42 (11): 2584–2588.
Amano S, Oshika T, Kaji Y, Numaga J, Matsubara M, Araie M . Herpes simplex virus in the trabeculum of an eye with corneal endothelitis. Am J Ophthalmol 1999; 127 (6): 721–722.
Salmon JF, Ursell PG, Frith P . Neovascular Glaucoma as a complication of retinal vasculitis in Crohn disease. Am J Ophthalmol 2000; 130 (4): 528–530.
Panek WC, Holland GN, Lee DA, Christensen RE . Glaucoma in patients with uveitis. Br J Ophthalmol 1990; 74 (4): 223–227.
Thoe Schwartzenberg GW, Buys YM . Glaucoma secondary to topical use of steroid cream. Can J Ophthalmol 1999; 34 (4): 222–225.
Reinauer S, Megahed M, Goerz G, Ruzicka T, Borchard F, Susanto F et al. Schonlein- Henoch purpura associated with gastric Helicobacter pylori infection. J Am Acad Dermatol 1995; 33 (5 part 2): 876–879.
Figura N, Giordano N, Burroni D, Macchia G, Vindigni G, Gemari C et al. Sjogren’s syndrome and Helicobacter pylori infection. Eur J Gastroenterol Hepatol 1994; 6 (2): 321–322.
Gasbarrini A, Franceschi F, Tartaglione R, Landolfi R, Pola P, Gasbarrini G et al. Regression of autoimmune thrombocytopenia after eradication of Helicobacter pylori. Lancet 1998; 352 (9131): 878.
Mendall MA, Goggin PM, Molineaux N, Levy J, Toosy T, Strachan D et al. Relation of helicobacter pylori infection and coronary heart disease. Br Heart J 1994; 71 (5): 437–439.
Gasbarrini A, Massari I, Serricchio M, Tondi P, De Luca A, Franceschi F et al. Helicobacter pylori and Raynaud phenomenon. Gastroenterol Int 1997; 21 (4): 765–770.
Gasbarrini A, De Luca A, Fiore G, Gambrielli M, Franceschi F, Ojetti V et al. Beneficial effects of Helicobacter pylori eradication on migraine. Hepatogastroenterology 1998; 21 (4): 765–770.
Kountouras J, Mylopoulos N, Boura P, Bessas C, Chatzopoulos D, Venizelos J et al. Relationship between Helicobacter pylori and glaucoma. Ophthalmology 2001; 108 (3): 599–604.
Kountouras J, Zavos C, Chatzopoulos D . Induction of apoptosis as a proposed pathophysiological link between glaucoma and Helicobacter pylori infection. Med Hypotheses 2004; 62 (3): 378–381.
Jabs DA, Nussenblatt RB, Rosenbaum JT . Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol 2005; 140 (3): 509–516.
Kim SY, Ahn JS, Ha YJ, Doh HJ, Jang MH, Chung SI et al. Serodiagnosis of Helicobacter pylori infection in Korean patients using enzyme-linked immunosorbent assay. J Immunoassay 1998; 19 (4): 251–270.
Brewerton DA, Caffrey M, Nicholls A, Walters D, James DCO . Acute anterior uveitis and HL-A27. Lancet 1973; 302 (7836): 994–996.
Blankenberg-Sprenkels SH, Fielder M, Feltkamp TE, Tiwana H, Wilson C, Ebringer A . Antibodies to Klebsiella pneumoniae in Dutch patients with ankylosing spondylitis and acute anterior uveitis and to Proteus mirabilis in rheumatoid arthritis. J Rheumatol 1998; 25 (4): 743–747.
Mattila L, Leirisalo-Repo M, Koskimies S, Granfors K, Siitonen A . Reactive arthritis following an outbreak of Salmonella infection in Finland. Br J Rheumatol 1994; 33 (12): 1136–1141.
Wakefield D, Stahlberg TH, Toivanen A, Granfors K, Tennant C . Serologic evidence of Yersinia infection in patients with anterior uveitis. Arch Ophthalmol 1990; 108 (2): 219–221.
Wakefield D, Penny R . Cell-mediated immune response to chlamydia in anterior uveitis: role of HLA B27. Clin Exp Immunol 1983; 51 (2): 191–196.
Falcon MG, William HP . Herpes simplex keratouveitis and glaucoma. Trans Ophthalmol Soc UK 1978; 98: 101–104.
Galloway PH, Warner SJ, Morshed MG, Mikelberg FS . Helicobacter pylori infection and the risk for open-angle glaucoma. Ophthalmology 2003; 110 (5): 922–925.
Kurtz S, Regenbogen M, Goldiner I, Horowitz N, Moshkowitz M . No association between Helicobacter pylori infection or Cag A bearing strains and glaucoma. J Glaucoma 2008; 17 (3): 223–226.
Kim JM, Kim SH, Park KH, Han SY, Shim HS . Investigation of the association between Helicobacter pylori infection and normal tension glaucoma. Invest Ophthalmol Vis Sci 2011; 52 (2): 665–668.
Choi CY, Kim MS, Kim JM, Park SH, Park KH, Hong C . Association between Helicobacter pylori infection and Posner-Schlossmann Syndrome. Eye 2010; 24 (1): 64–69.
Cutler AF, Prasad VM . Long-term follow-up of helicobacter pylori serology after successful eradication. Am J Gastroenterol 1996; 91 (1): 85–88.
Dill S, Payne-James JJ, Misiewicz JJ, Grimble GK, McSwiggan D, Pathak K et al. Evaluation of C urea breath test in the detection of H. pylori and in monitoring the effect of tripotassium dicitratobisnuthate in nonulcer dyspepsia. Gut 1990; 31 (11): 1237–1241.
Perez-Perez GI, Rothenbacher D, Brenner H . Epidemiology of Helicobacter pylori infection. Helicobacter 2004; 9 (Suppl 1): 1–6.
Kim N . Epidemiology and transmission route of Helicobacter pylori infection. Korean J Gastroenterol 2005; 46 (3): 153–158.
Yim JY, Kim N, Choi SH, Kim YS, Cho KR, Kim SS et al. Seroprevalence of Helicobacter pylori in South Korea. Helicobacter 2007; 12 (4): 333–340.
Granfors K . Host-microbe interaction in reactive arthritis: does HLA-B27 have a direct effect? J Rheumatol 1998; 25 (9): 1659–1661.
Appelmelk BJ, Simoons-Smit I, Negrini R, Moran AP, Aspinall GO, Forte JG et al. Potential role of molecular mimicry between Helicobacter pylori lipopolisaccharide and host Lewis blood group antigens in a autoimmunity. Infect Immun 1996; 64 (6): 2031–2040.
Ogiso M, Takehana M, Kobayashi S, Hoshi M . Expression of sialylated Lewis x gangliosides in cultured lens epithelial cells from rhesus monkey. Exp Eye Res 1998; 66 (6): 765–773.
Davies GR, Simmonds NJ, Stevens TR, Sheaff MT, Banatvala N, Laurenson IF et al. Helicobacter pylori stimulates antral mucosal reactive oxygen metabolite production in vivo. Gut 1994; 35 (2): 179–185.
Siomek A, Rytarowska A, Szaflarska-Poplawska A, Gackowski D, Rozalski R, Dziaman T et al. Helicobacter pylori infection is associated with oxidativelydamaged DNA in human leukocytes and decreased level of urinary 8-oxo-7,8-dihydroguanine. Carcinogenesis 2006; 27 (3): 405–408.
Lahesmaa R, Skurnik M, Vaara M, Leirisalo-Repo M, Nissilä M, Granfors K et al. Molecular mimicry between HLA-B27 and Yersinia, Salmonella, Shigella and Klebsiella within the same region of HLA alpha-I helix. Clin Exp Immunol 1991; 86 (3): 399–404.
Granfors K, Märker-Hermann E, de Keyser F, Khan MA, Veys EM, Yu DT . The cutting edge of spondylarthropathy research in the millennium. Arthritis Rheum 2002; 46 (3): 606–613.
Otasevic L, Zlatanovic G, Stanojevic-Paovic A, Miljkovic-Selimovic B, Dinic M, Djordjevic-Jocic J et al. Helicobacter pylori: An underestimated factor in acute anterior uveitis and spondyloarthropathies? Ophthalmologica 2007; 221 (1): 6–13.
Saccà SC, Pascotto A, Venturino GM, Prigione G, Mastromarino A, Baldi F et al. Prevalence and treatment of Helicobacter pylori in patients with blepharitis. Invest Ophthalmol Vis Sci 2006; 47 (2): 82–85.
Saouli N, Brézin AP . Ocular hypertension and uveitis. Study of 374 cases of uveitis. J Fr Opthalmol 1999; 22 (9): 943–949.
Santos C . Herpes simplex uveitis. Bol Asoc Med P R 2004; 96 (2): 71–74 77–83.
Sungur GK, Hazirolan D, Yalvac IS, Ozer PA, Aslan BS, Duman S . Incidence and prognosis of ocular hypertension secondary to viral uveitis. Int Ophthalmol 2010; 30 (2): 191–194.
Falcon MG, Williams HP . Herpes simplex keratouveitis and glaucoma. Trans Ophthalmol Soc UK 1978; 98 (1): 783–787.
Jones R, Pasquale LR, Pavan-Langston D . Herpes simplex virus: An important etiology for secondary glaucoma. Int Ophthalmol Clin 2007; 47 (2): 99–107.
Tsamakidis K, Panotopoulou E, Dimitroulopoulos D, Xinopoulos D, Christodoulou M, Papadokostopoulou A et al. Herpes simplex virus type 1 in peptic ulcer disease: an inverse association with Helicobacter Pylori. World J Gastroenterol 2005; 11 (42): 6644–6649.
Baccaglini L, Schoenbach VJ, Poole C, McKaig RG, Ibrahim J, Baric RS et al. Association between herpes simplex virus type 1 and helicobacter pylori in US adolescents. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 101 (1): 63–69.
Acknowledgements
This study was supported by a grant of the Korea Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A101727).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Kim, J., Park, K., Choi, M. et al. The effects of Helicobacter pylori infection on intraocular pressure in anterior uveitis. Eye 26, 1503–1510 (2012). https://doi.org/10.1038/eye.2012.206
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2012.206
