
Abstract
Background/Objectives:
We estimated the risk of infection associated with the duration of exclusive breastfeeding (EBF).
Subject/Methods:
We analysed the data on 15 809 term, singleton infants from the UK Millennium Cohort Study. Infants were grouped according to months of EBF: never, <2, 2–4, 4–6 and 6 (the latter being World Health Organisation (WHO) policy since 2001: ‘post-2001 WHO policy’). Among those EBF for 4–6 months, we separated those who started solids, but not formula, before 6 months, and were still breastfeeding at 6 months (that is, WHO policy before 2001: ‘pre-2001 WHO policy’), from other patterns. Outcomes were infection in infancy (chest, diarrhoeal and ear).
Results:
EBF was not associated with the ear infection, but was associated with chest infection and diarrhoea. EBF for <4 months was associated with a significantly increased risk of chest infection (adjusted risk ratios (RR) 1.24–1.28) and diarrhoea (adjusted RRs 1.42–1.66) compared with the pre-2001 WHO policy. There was an excess risk of the chest infection (adjusted RR 1.19, 95% confidence interval (CI): 0.97–1.46) and diarrhoea (adjusted RR 1.66, 95% CI: 1.11, 2.47) among infants EBF for 4–6 months, but who stopped breastfeeding by 6 months, compared with the pre-2001 WHO policy. There was no significant difference in the risk of chest infection or diarrhoea in those fed according to the pre-2001 versus post-2001 WHO policy.
Conclusions:
There is an increased risk of infection in infants EBF for <4 months or EBF for 4–6 months who stop breastfeeding by 6 months. These results support current guidelines of EBF for either 4–6 or 6 months, with continued breastfeeding thereafter.
Similar content being viewed by others


Introduction
Breastfeeding has many health benefits, including protection against gastrointestinal and respiratory infections in infants. The World Health Organisation (WHO) and governments worldwide promote exclusive breastfeeding (EBF), although the most appropriate age for solids to be introduced is still debated. Before 2001, the WHO recommended that solids were introduced at 4–6 months, whereas in 2001, the recommendation was changed to 6 months.1 The change was based largely on a systematic review that compared the effect of EBF for 6–7 months with ‘EBF for at least 3–4 months and mixed feeding thereafter (that is, breast milk plus solids and/or formula).2 The review, which was updated in 2012,3 found that in studies from Belarus, Iran and Nigeria, EBF for 6+ months was associated with less gastrointestinal infection and (in Iran and Nigeria) less respiratory infection in infancy compared with EBF for 3–4 months. There were no differences between the two groups with respect to other outcomes.
The WHO policy of 6 months of EBF has been widely adopted by many countries.4, 5, 6 Despite this, the majority of infants are not EBF at 6 months, particularly in developed countries. For example, on average 39% of infants in Organisation for Economic Cooperation and Development countries are EBF for 4 months and 23% are EBF for 6 months.7 The rates of EBF in the UK are even lower: in 2010, 12% were EBF for 4 months and 1% were EBF for 6 months.8
Given that many more infants are fed according to the pre-2001 WHO policy (defined in Table 1) than with the current (hereafter referred to as post 2001) policy, we estimated the risk of infection in infants fed according to the pre-2001 policy compared with infants fed according either to the post-2001 policy, or with shorter periods of EBF (as defined in Table 1). We estimated these risks in a large UK cohort born at a time when the pre-2001 WHO policy was still national policy, and with a sufficient number of infants who were EBF for 4–6 months. In this paper, we define the pre-2001 WHO policy as EBF for 4.0–5.9 months rather than EBF for 4–6 months, so as to enable a direct comparison of two mutually exclusive groups (EBF for 4.0–5.9 months and EBF for 6 months).
Participants and methods
Millennium cohort study
The Millennium Cohort Study is a nationally representative longitudinal study of 18 818 infants born in the UK.9 A random two-stage sample of all infants born in England and Wales between September 2000 and August 2001, and in Scotland and Northern Ireland between November 2000 and January 2002, who were alive and living in the UK at age 9 months was drawn from Child Benefit registers. At the time of the survey, Child Benefit claims in the UK covered virtually all children. Stratified sampling by electoral ward (defined geographical area), with over-sampling of ethnic minority and disadvantaged areas, ensured adequate representation of such areas. The interview response rate was 85%.9 Parents were interviewed for the first time when infants were aged 9 months, and detailed information was collected on socio-economic and health factors.
Exclusions
This analysis focused on term, singleton infants who did not have major problems at birth. Hence, 3008 infants (16% of the original 18 818) were excluded, sequentially, for the following reasons: multiples (n=522); gestational age <37 weeks or missing (n=1525); admission to intensive care units at birth (n=961); and main respondent not the birth mother (n=1). The analysis was based on the remaining 15 809 infants.
Breastfeeding
Breastfeeding patterns were assessed by maternal report that has been shown to be reliable in other studies10, 11 Breastfeeding initiation was assessed by the question ‘Did you ever try to breastfeed your baby?’. Breastfeeding duration was estimated using the questions about the age of the infant when last given breast milk, and when first given formula, other types of milk and solids. Infants were grouped into 2-month bands according to their duration of EBF: never breastfed, <2, 2–3.9, 4–5.9 and 6+ months (hereafter referred to as never, <2, 2–4, 4–6 and 6+ months). Among the infants who were EBF for at least 4 months, we separated out those fed according to the post-2001 WHO policy (EBF for 6+ months), the pre-2001 WHO policy (EBF for 4–6 months, with solids, but no formula, introduced at 4–6 months and still breastfeeding at 6 months) and infants with other feeding patterns (Table 1).
Infant morbidity
At the 9 months interview, the mothers were asked about medical consultations for their baby’s health: ‘We would like to know about any health problems for which <Jack> has been taken to the GP, Health Centre or Health Visitor, or to Casualty, or you have called NHS Direct’. Several possible health problems were listed, for example, chest infections, ear infections, severe or persistent diarrhoea. Multiple different health problems were recorded, although the same health problem was not recorded more than once. For example, an infant who had had a chest infection, severe diarrhoea and an ear infection at some point in infancy would have all three problems recorded, but an infant who had three chest infections would only have chest infection recorded once; hence, we could not analyse multiple events. We analysed the occurrence of any: chest infections, persistent or severe diarrhoea, and ear infection. Data were not available on when in infancy the health problem occurred.
The mothers were also asked about hospital admissions: ‘Has your baby ever been admitted to a hospital ward because of an illness or health problem?’. Several possible reasons for admission were listed, including ‘gastro-enteritis’ and ‘chest infection or pneumonia’, hereafter referred to as diarrhoea and lower respiratory tract infection (LRTI), respectively. We have previously used time-changing variables to estimate the association between exclusive/partial breastfeeding in the past month and the risk of hospitalisation for these infections during the same month,12, 13 but we have not previously estimated the association between the duration of EBF and these outcomes. We report these associations here for completeness.
Statistical methods
The risk of each outcome during infancy was estimated according to infant feeding group, using those who followed the pre-2001 WHO policy (group 7 in Table 1, n=1122) as the reference.
Risk ratios were estimated using modified Poisson regression.14 All analyses were adjusted for the infant’s age at recruitment (range 8–12 months; 75% were aged 9 months). The risk ratios were also adjusted for the following variables that were associated with the feeding group or the outcome in univariable analysis (P<0.10): infant’s sex; infant’s ethnicity; maternal age; maternal education; social class; marital status; household income; household crowding; gestational age; birthweight; mode of delivery; smoking and alcohol during pregnancy; whether the mother was a current smoker; (for the analysis of chest infection/LRTI) family history of asthma; whether the infant had other siblings; and age when started formal childcare. Owing to the large number of potential confounders, multivariable models were fitted in three stages, adjusting first for socio-demographic variables, then all other variables and finally adjusting for both sets of variables simultaneously. At each stage, variables that were no longer statistically significant (P<0.05, two sided) were dropped. In final models, adjustment was made only for those variables that were significantly (P<0.05, two sided) associated with the outcome after adjustment for other variables in the model (see footnote in Table 2, which also shows the sample size for final models).
All analyses allowed for the clustered, stratified sample using the ‘survey commands’ in Stata version 13 (Stata Corporation, College Station, USA). Hence, all proportions and risk ratios are weighted, and all confidence intervals (CI) are adjusted for clustering. Missing data was minimal, hence all results are based on complete case analysis.
Data deposition
Our study is a secondary analysis of Millennium Cohort Study (MCS) data sets that have been deposited in the UK data archive.
Ethical approval
Informed consent was obtained from all included parents in the original study. Ethical approval to conduct the original study was granted by the South West (MREC/01/6/19), London (MREC/03/2/022), London (05/MRE02/46) and Northern/Yorkshire (07/MRE03/32) Multi-Centre Medical Research Ethics Committees.
Results
Of the 15 809 infants in the study, 34.0% were never breastfed, 35.7% were EBF for <2 months and 14.8% were EBF for 2–4 months (Table 1). A further 7.1% and 1.2% were fed according to the pre-2001 (group 7) and post-2001 WHO (group 8) policy, respectively. Among the 190 infants, who were EBF for at least 6 months, 140 (74%) were EBF for 6 months, whereas 24 (13%) and 26 (14%) were EBF for 7 and 8-9 months, respectively. As group 6 was too small to allow meaningful comparisons, it has been omitted from all further tables.
Characteristics associated with EBF
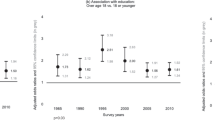
There were striking differences in the characteristics of the feeding groups (Tables 3 and 4); P<0.001 for an overall difference between the seven groups for all characteristics except gestational age in weeks (P=0.003) and parental asthma (P=0.086). In general, the infants who were never breastfed were more likely to have the most disadvantaged socio-economic profile (for example, neither parent had a professional occupation, the mother was not university educated and had no formal qualifications; Table 3; Figure 1a). A longer duration of EBF was associated with a more advantaged socio-economic profile, although the groups who EBF for at least 4 months (particularly groups 5, 7 and 8, who were all EBF for at least 4 months and still being breastfed at 6 months) tended to be more similar to each other than to the groups who EBF for <4 months.

(a) Distribution of household occupation and mother’s education according to the duration of exclusive breastfeeding. (b) Distribution of mother’s smoking status at 9 months and infant’s childcare according to the duration of exclusive breastfeeding.
The infants who were never breastfed had the highest prevalence of maternal smoking in pregnancy (35.8%) and currently (44%); these prevalences decreased with the duration of EBF, although again there was very little difference between groups 5, 7 and 8 (Table 4; Figure 1b). The majority of infants in groups 7 and 8 (60.6% and 67.2%, representing the pre-2001 and post-2001 WHO policy, respectively) were not in formal childcare at age 9 months.
Risk ratios for medical consultation for infection
Overall, the proportion of infants who had at least one episode of each outcome was 10.2% for ear infection, 28.8% for chest infection and 9.2% for persistent or severe diarrhoea. Overall, 3.5% and 1.4% of infants were hospitalised for LRTI and diarrhoea, respectively.
The risk of ear infection varied only slightly according to the duration of EBF and none of the risk ratios were statistically significant (Table 2). In contrast, the risk of chest infection and diarrhoea varied significantly according to the duration of EBF (Table 2; Figure 2); for chest infection, there was a clear dose response effect. Infants who were EBF for <4 months (groups 1–3) had a significantly increased risk of chest infection (adjusted risk ratios varying between 1.24 and 1.28) and diarrhoea (adjusted risk ratios varying between 1.42 and 1.66) compared with infants who were fed according to the pre-2001 WHO policy. There was an excess risk of diarrhoea (adjusted risk ratio 1.66, 95% CI: 1.11, 2.47, P=0.015) among those infants who were EBF for at least 4 months, but stopped any breastfeeding before 6 months (group 4), compared with those who were fed according to the pre-2001 WHO policy.

Adjusted risk ratios for chest infection and persistent/severe diarrhoea comparing duration of EBF with the pre-2001 WHO policy.
There was no significant difference in the risk of chest infection or diarrhoea in those who followed the pre-2001 versus the post-2001 WHO policy, although the latter group was small (n=190).
Risk ratios for hospitalisation for infection
The association between the duration of EBF and hospitalisation for LRTI was similar to that for non-hospitalised chest infection, although the number of events was relatively small and the effects were not always statistically significant (Table 2). For hospitalisation due to diarrhoea, the number of events in the reference group (those fed according to the pre-2001 WHO policy) was too low (2 out of 1122) to allow robust estimates of risk ratios.
Discussion
In this large UK cohort, infants who were EBF for any period of time that was <4 months—even for 2–4 months—had a significantly increased risk of chest infection and diarrhoea compared with infants who were fed according to the pre-2001 WHO policy (EBF for 4–6 months, introduced solids but no formula before 6 months, still breastfeeding at 6 months). There was even an excess risk of diarrhoea among those infants who were EBF for at least 4 months, but stopped all breastfeeding before 6 months, compared with those who were fed according to the pre-2001 WHO policy. The lowest risk of chest infection and diarrhoea was in infants who were EBF for at least 4 months, with partial breastfeeding for at least 6 months, that is, those who were fed according to the pre-2001 or post-2001 WHO policy. Our study did not have a large enough number of infants who followed the post-2001 WHO policy to allow meaningful comparison of outcomes with the pre-2001 WHO policy.
The main strengths of our study are the large sample size, adjustment for numerous confounders and detailed data on infant feeding. As there were enough infants who followed the pre-2001 WHO policy (n=1122), these formed the reference group, thus enabling us to estimate the risks associated with a shorter duration of EBF compared with the recommended UK policy at that time. This is in contrast to most other studies which estimate the benefits of different breastfeeding durations compared with the ‘never breastfed’ group.
The main limitation is that data on infant feeding and infection were obtained through maternal report. In particular, the feeding patterns in our study, which are based on the infant’s age when last breastfed, or first given solids or formula, will be prone to rounding error, particularly as many responses were given in months rather than days or weeks. Several studies have shown that mothers accurately report breastfeeding duration within 1 month, up to 3 years after delivery, although data on the introduction of solids or formula are less valid.10, 11 The data on breastfeeding duration and introduction of solids in our study are similar to those reported in the UK Infant Feeding Survey of infants born in August to October 2000,15 on average, 6 months before the MCS babies: the proportion of infants breastfed for at least 6 months was 22% in the MCS and 21% in the Infant Feeding Survey; in both studies, 85% of infants had started solids by 4 months.
Maternal report of hospitalisation, a serious and rare event, is likely to be accurately recalled during this 9 month period, but the number of events was relatively small. Maternal report of infection that required a medical consultation during the past 9 months is likely to be remembered with reasonable accuracy,16 although these subjective responses may be prone to diagnostic misclassification, for example, mother’s report of the chest infection may include a range of respiratory conditions and, similarly, mother’s perceptions of ‘severe or persistent diarrhoea’ may vary. Another limitation is that the MCS did not collect data on the timing of the infection. Hence, we cannot rule out reverse causality, nor ascertain whether infection occurred after the period of EBF (indicating that EBF is protective) or during the period of EBF.
Several studies have shown that EBF, particularly when it is prolonged, is associated with a lower risk of infection.17, 18, 19, 20, 21 Few studies have used a relatively long period of EBF, as recommended in the pre-2001 or post-2001 WHO policy, as the reference group. A study from Spain19 used EBF for at least 4 months, as the reference group and observed a higher risk of hospitalisation for infection in infants, who were never breastfed (adjusted RR=4.91) or EBF for <4 months (adjusted RR=2.45). Similarly, a Dutch study20 observed a higher risk of LRTI (adjusted Odds ratio=2.0) and a higher risk of gastrointestinal infection (Odds ratio=2.44) in infants, who were never breastfed compared with those who were EBF for 4 months and partially breastfed thereafter. Our findings on the risks associated with not breastfeeding compared with EBF for 4–6 months are consistent with both of these studies.
The Cochrane review3 identified few studies from developed countries that compared the risk of respiratory infection,20, 22, 23 gastrointestinal infection,18, 20 and otitis media18, 24 in those who EBF for 6–7 months with those who EBF for at least 3–4 months. Our results are broadly consistent with these, although our estimated effect for diarrhoea is weaker (adjusted RR 0.97, 95% CI: 0.45–2.09) than in the Cochrane review 0.61 (95% CI: 0.41–0.93), possibly because the infants in our reference group had a longer period of EBF (4–6 months) than in the Belarus study (3–6 months).
Breast milk has many immunological properties that are likely to protect against infection in infancy.25 Infection may also occur due to contamination of bottles, teats, milk and food in infants, who are not exclusively breastfed. Both of these may contribute to a higher risk of chest infection and diarrhoea in infants, who were never breastfed compared with those who were EBF for at least 4–6 months. However, we also observed a significantly higher risk of diarrhoea in infants, who were EBF for 4–6 months, but who stopped breastfeeding before 6 months, which suggests that there are benefits of continued partial breastfeeding after solids have been introduced.
The WHO recommendation of 6 months of EBF has been widely adopted, but the evidence for the policy has been questioned26 and some experts have promoted a less stringent recommendation that is more akin to the pre-2001 WHO policy.27, 28 In our cohort, the pre-2001 WHO policy is associated with significantly less chest infection and diarrhoea compared with EBF for up to 4 months. Importantly, we have not assessed the effect on other outcomes in infancy and childhood. Given that many more infants are fed according to the pre-2001 rather than the post-2001 WHO policy, future research should continue to strengthen the evidence base for the optimal duration of EBF. The pre-2001 and post-2001 WHO policies can only be directly compared with studies that have detailed data on EBF and a sufficiently large number of infants fed according to the two policies. Current feeding guidelines should continue to promote EBF for either 4–6 or 6 months, with continued breastfeeding thereafter. Recommendations for prolonged breastfeeding need to be accompanied by policies that enable prolonged maternity leave, and support breastfeeding in public places and after returning to work.
References
World Health Organization The Optimal Duration of Exclusive Breastfeeding: Report of an Expert Consultation. World Health Organization: Geneva, 2001.
Kramer MS, Kakuma R . Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev 2002; Cd003517.
Kramer MS, Kakuma R . Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev 2012; 8: Cd003517.
Department of Health UK. Infant feeding recommendation, 2003.
Gartner LM, Morton J, Lawrence RA, Naylor AJ, O'Hare D, Schanler RJ et al. Breastfeeding and the use of human milk. Pediatrics 2005; 115: 496–506.
National Health and Medical Research Council. Infant feeding guidelines for health workers. Commonwealth of Australia, 2003.
OECD OECD Family Database. OECD: Paris, 2015.
McAndrew F, Thompson J, Fellows L, Large A, Speed M, Renfrew MJ . Infant Feeding Survey 2010. Health and Social Care Information Centre: Leeds, 2012.
Plewis I, Calderwood L, Hawkes D, Hughes G, Joshi H . Millennium Cohort Study: Technical Report on Sampling. Institute of Education, University of London: London, 2004; 16.
Eaton-Evans J, Dugdale AE . Recall by mothers of the birth weights and feeding of their children. Hum Nutr Appl Nutr 1986; 40: 171–175.
Li R, Scanlon KS, Serdula MK . The validity and reliability of maternal recall of breastfeeding practice. Nutr Rev 2005; 63: 103–110.
Quigley MA, Kelly YJ, Sacker A . Breastfeeding and hospitalization for diarrheal and respiratory infection in the United Kingdom Millennium Cohort Study. Pediatrics 2007; 119: e837–e842.
Quigley MA, Kelly YJ, Sacker A . Infant feeding, solid foods and hospitalisation in the first 8 months after birth. Arch Dis Child 2009; 94: 148–150.
Zou G . A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol 2004; 159: 702–706.
Hamlyn B, Brooker S, Oleinikova K, Wands S, Infant feeding 2000: A survey conducted on behalf of the Department of Health, the Scottish Executive, the National Assembly for Wales and the Department of Health, Social Services and Public Safety in Northern Irelan. TSO, London, 2002.
Pless CE, Pless IB . How well they remember. The accuracy of parent reports. Arch Pediatri Adolesc Med 1995; 149: 553–558.
Howie PW, Forsyth JS, Ogston SA, Clark A, Florey CD . Protective effect of breast feeding against infection. BMJ 1990; 300: 11–16.
Kramer MS, Guo T, Platt RW, Sevkovskaya Z, Dzikovich I, Collet JP et al. Infant growth and health outcomes associated with 3 compared with 6 mo of exclusive breastfeeding. Am J Clin Nutr 2003; 78: 291–295.
Paricio Talayero JM, Lizan-Garcia M, Otero Puime A, Benlloch Muncharaz MJ, Beseler Soto B, Sanchez-Palomares M et al. Full breastfeeding and hospitalization as a result of infections in the first year of life. Pediatrics 2006; 118: e92–e99.
Duijts L, Jaddoe VW, Hofman A, Moll HA . Prolonged and exclusive breastfeeding reduces the risk of infectious diseases in infancy. Pediatrics 2010; 126: e18–e25.
Ajetunmobi OM, Whyte B, Chalmers J, Tappin DM, Wolfson L, Fleming M et al. Breastfeeding is associated with reduced childhood hospitalization: evidence from a Scottish Birth Cohort (1997-2009). J Pediatr 2015; 166: 620–5.e4.
Kramer MS, Chalmers B, Hodnett ED, Sevkovskaya Z, Dzikovich I, Shapiro S et al. Promotion of Breastfeeding Intervention Trial (PROBIT): a randomized trial in the Republic of Belarus. JAMA 2001; 285: 413–420.
Oddy WH, Sly PD, de Klerk NH, Landau LI, Kendall GE, Holt PG et al. Breast feeding and respiratory morbidity in infancy: a birth cohort study. Arch Dis Child 2003; 88: 224–228.
Duncan B, Ey J, Holberg CJ, Wright AL, Martinez FD, Taussig LM . Exclusive breast-feeding for at least 4 months protects against otitis media. Pediatrics 1993; 91: 867–872.
Lawrence RA, Lawrence RM . Breastfeeding: a guide for the medical professional: Elsevier Health Sciences, 2010.
Fewtrell M, Wilson DC, Booth I, Lucas A . Six months of exclusive breast feeding: how good is the evidence? BMJ 2011; 342: c5955.
Agostoni C, Decsi T, Fewtrell M, Goulet O, Kolacek S, Koletzko B et al. Complementary feeding: a commentary by the ESPGHAN Committee on Nutrition. J Pediatr Gastroenterol Nutr 2008; 46: 99–110.
British Dietetic Association. Complementary feeding: introduction of solid food to an infant's diet, 2013.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Author contributions
MQ analysed the data, drafted the initial manuscript and approved it for submission. CC, AS and YK contributed to the interpretation of data, critically reviewed and revised the manuscript, and approved it for submission.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Quigley, M., Carson, C., Sacker, A. et al. Exclusive breastfeeding duration and infant infection. Eur J Clin Nutr 70, 1420–1427 (2016). https://doi.org/10.1038/ejcn.2016.135
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejcn.2016.135
This article is cited by
-
Association between breastfeeding duration and diabetes mellitus in menopausal women: a machine-learning analysis using population-based retrospective study
International Breastfeeding Journal (2024)
-
Determinants and spatial factors of anemia in women of reproductive age in Democratic Republic of Congo (drc): a Bayesian multilevel ordinal logistic regression model approach
BMC Public Health (2024)
-
Development of SARS-CoV-2 specific IgG and IgA antibodies in serum and milk with different SARS-COV-2 vaccines in lactating women
International Breastfeeding Journal (2023)
-
No such thing as a free lunch: The direct marginal costs of breastfeeding
Journal of Perinatology (2023)
-
Relationship of Breastfeeding Self-Efficacy with Self-Esteem and General Health in Breastfeeding Mothers Referred to Health Centers of Falavarjan City-Iran, 2015
Community Mental Health Journal (2019)
