
Abstract
Recently developed heavy ion irradiation therapy using a carbon beam (CB) against systemic malignancy has numerous advantages. However, the clinical results of CB therapy against glioblastoma still have room for improvement. Therefore, we tried to clarify the molecular mechanism of CB-induced glioma cell death. T98G and U251 human glioblastoma cell lines were irradiated by CB, and caspase-dependent apoptosis was induced in both cell lines in a dose-dependent manner. Knockdown of Bax (BCL-2-associated X protein) and Bak (BCL-2-associated killer) and overexpression of Bcl-2 or Bcl-xl (B-cell lymphoma-extra large) showed the involvement of Bcl-2 family proteins upstream of caspase activation, including caspase-8, in CB-induced glioma cell death. We also detected the activation of extracellular signal-regulated kinase (ERK) and the knockdown of ERK regulator mitogen-activated protein kinase kinase (MEK)1/2 or overexpression of a dominant-negative (DN) ERK inhibited CB-induced glioma cell death upstream of the mitochondria. In addition, application of MEK-specific inhibitors for defined periods showed that the recovery of activation of ERK between 2 and 36 h after irradiation is essential for CB-induced glioma cell death. Furthermore, MEK inhibitors or overexpression of a DN ERK failed to significantly inhibit X-ray-induced T98G and U251 cell death. These results suggested that the MEK–ERK cascade has a crucial role in CB-induced glioma cell death, which is known to have a limited contribution to X-ray-induced glioma cell death.
Similar content being viewed by others


Main
Since the first clinical trial in 1994, the efficacy of high linear energy transfer (LET) heavy ion therapy using a carbon beam (CB) has been proven in various cancer treatments, including cases of radioresistant tumors.1, 2 Compared with conventional low-LET radiotherapy, high-LET CB therapy has numerous therapeutic advantages. Furthermore, CB offers ideal energy distribution around the Bragg peak, which induces a maximum ionizing effect in the pathological lesion and less damage to the surrounding normal tissue, leading to better tumor controllability with shorter treatment times and fewer side effects.1, 3, 4, 5
Similar to other radioresistant tumors, the therapeutic approach for cerebral malignant glioma, which has one of the poorest prognoses among systemic tumors because of its extremely high resistance to various chemotherapeutic and radiotherapeutic approaches,6 the use of CB therapy had already started an early phase of development.7 Although intracranial chordoma indicated an excellent outcome after CB treatment (overall survival 89.4% per 3 years) compared with conventional radiotherapy,8 the results of glioma therapy by CB irradiation were not considered to be better.
As CB-irradiation therapy was developed relatively recently and a very limited number of heavy ion accelerators exist across the world, the accumulation of evidence regarding the molecular mechanism of CB-induced tumor cell death is ongoing. A wide variety of modes of glioma cell death induced by conventional radiotherapy have been reported, including apoptosis,9, 10 necrotic cell death,10 and autophagic cell death.11 On the other hand, from several reports showing the mechanism of CB irradiation-induced death of tumor cells, including glioma cells, details of the characteristics/mechanism of CB irradiation-induced glioma cell death are still unknown. Therefore, further understanding of the mechanism of CB irradiation-induced glioma cell death could improve the prospects for clinical glioma therapy using CB irradiation.
In this study, we explored the detailed molecular mechanism of CB irradiation-induced glioma cell death, including the mode of cell death, the involvement of major intracellular cell death signal cascades, and CB irradiation-specific cell death signal transducers, to improve CB-irradiation therapy in glioma treatment and to achieve better clinical outcomes.
Results
CB irradiation induces cell death of human glioma cell lines with apoptotic features in a dose-dependent manner
First, to investigate the characteristics/mechanism of CB irradiation-induced glioma cell death, we determined the conditions of CB irradiation treatment that induced moderate glioma cell death. Therefore, to determine the appropriate irradiation dose, T98G and U251 human glioma cells were irradiated with a 1–10 Gy CB, which is near the clinical CB irradiation dose for glioma therapy.7 As a result, induction of cell death in both cell lines was confirmed in a dose-dependent manner at 48 h after irradiation (Supplementary Figure 1a). Nuclear staining with propidium iodide (PI) for quantitation of cell death also showed the irradiation dose dependency of CB irradiation-induced cell death (Figure 1a, left), as observed in phase-contrast images. Next, to investigate the characteristics of CB irradiation-induced cell death, we tried to detect apoptosis, which is the typical form of programmed cell death,12 by additional staining of the nuclei using Hoechst 33342 and by a DNA ladder formation assay. As a result, cells with apoptotic nuclear morphology corresponding to PI-positive cells also increased in an irradiation dose-dependent manner in both types of CB-irradiated cells (Figure 1a, right), and DNA ladder formation was observed as well (Supplementary Figure 1b). From these results, it was suggested that CB irradiation triggers apoptotic cell death in human glioma cells.

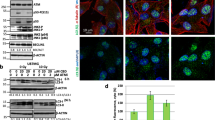
CB irradiation induces multiple caspase-dependent apoptosis in T98G and U251 glioma cells. (a) T98G and U251 cells treated with or without CB irradiation at the indicated doses were stained with Hoechst 33342 or propidium iodide (PI), and the percentages of dead cells and apoptotic/dead cells were counted using a microscope, as described in the ‘Materials and methods’ section at 48 h after irradiation. (b) T98G and U251 cells were CB irradiated (5 Gy) and harvested at the indicated time points after irradiation. The whole-cell lysates obtained were subjected to immunoblotting using the indicated antibodies. As a control of irradiation and DNA damage-induced responses, total cell lysates of T98G and U251 cells obtained at the indicated time periods after X-ray irradiation (20 Gy) or UVC (UV, 200 J) were also subjected to immunoblotting using the same antibodies. The membranes were reprobed using an α-tubulin antibody to confirm equal protein loading. For the detection of cytochrome c release from the mitochondria into the cytosol, T98G and U251 cells were treated by the same stimuli, and then cell lysates obtained at the indicated time points were fractionated into cytosol- and mitochondria-rich fractions as described in the ‘Materials and methods’ section and were subjected to immunoblotting using an anti-cytochrome c antibody. To check for equal protein loading, the membranes were reprobed using organelle-specific antibodies (anti-α-tubulin for the cytosol and anti-HSP60 for the mitochondria). (c) T98G and U251 cells were CB irradiated (5 Gy) and harvested at the indicated time points after irradiation. The total cell lysates obtained were subjected to immunoblotting using anti-caspase-8 and anti-Bid antibodies. As a control for extrinsic pathway activation, whole-cell lysates obtained from T98G and U251 cells 48 h after irradiation by X-ray (X-ray, 20 Gy) or treatment with tumor necrosis factor (TNF) 1000 IU+cycloheximide (CHX) 10 μg/ml were also subjected to immunoblotting using the same antibodies. The membranes were reprobed with an anti-α-tubulin to confirm equal protein loading. (d) T98G and U251 cells pretreated with pan-caspase inhibitors (z-VAD-FMK (VAD, 200 μM) or Boc-D-FMK (Boc, 200 μM)) or specific caspase inhibitors (z-DEVD-CHO (DEVD, 200 μM, for caspase-3), z-LEHD-CHO (LEHD, 200 μM, for caspase-9), or z-IETD-CHO (IETD, 200 μM, for caspase-8)) for 2 h were CB irradiated (5 Gy) and subjected to quantitation of apoptosis and cell death as described in panel at 48 h after irradiation (*P<0.05). Total cell lysates from cells treated in the same manner at 48 h after irradiation were subjected to immunoblotting using anti-caspase-3, anti-caspase-9, anti-caspase-8, and anti-PARP antibodies. The membranes were reprobed using an anti-α-tubulin antibody to confirm equal protein loading
As both T98G cells and U251 cells are p53 mutated, which acts as a DNA damage sensor and has a critical role in DNA damage-induced cell death,13 the above results suggested that CB-induced glioma cell death may not necessarily require the p53 activity. Consistent with this idea, CB irradiation did not increase p53 expression (Supplementary Figure 1c). On the other hand, we asked whether another intracellular damage signal initiator, endoplasmic reticulum (ER) stress,14 could be involved in CB-induced glioma cell death. As shown in Supplementary Figure 1c, CB irradiation did not induce the expression of an ER stress marker GRP78, suggesting that the ER stress response may not have a role in CB-induced glioma cell death.
Multiple caspases are involved in CB irradiation-induced cell death
Usually, caspases have a crucial role in the final step of apoptosis; therefore, we investigated the activation of various caspases in CB irradiation-induced cell death. Time kinetics analysis of caspase-9, caspase-3, and caspase-8 showed not only the activation of caspase-9 and caspase-3, which are mainly implicated in the intrinsic pathway, but also that of caspase-8, which is mainly implicated in the extrinsic pathway,12 and these caspases were activated from 48 h after irradiation (Figure 1b and c). In addition, processing of the major effector caspase substrate poly-ADP ribose polymerase (PARP), cytochrome c release to the cytosol from the mitochondria, and processing of the caspase-8 substrate Bcl-2 interacting domain death agonist (Bid) were also observed (Figure 1b and c). Taken together, multiple caspases are activated upon the induction of glioma cell death by CB irradiation. Next, to investigate the functional involvement of these caspases, we used pan-caspase inhibitors or specific inhibitors of each caspase and evaluated their effect on CB irradiation-induced T98G and U251 cell death. As a result, pan-caspase inhibitors blocked CB irradiation-induced caspase activation, processing of PARP, apoptosis, and cell death of T98G and U251 effectively, whereas each specific caspase inhibitor suppressed CB irradiation-induced glioma cell death efficiently but not as much as pan-caspase inhibitors (Figure 1d). These results suggested that caspases are functionally essential for CB irradiation-induced T98G and U251 glioma cell death.
Bcl-2 family proteins regulate CB-induced caspase activation and apoptosis of glioma cells at the mitochondrial level
In considering the caspase activation mechanism, the mitochondria are the key intracellular organelle that relays caspase cascade-activating signals. Therefore, we investigated the involvement of the mitochondria. As proapoptotic Bcl-2 family proteins, especially multidomain type proapoptotic Bcl-2 family proteins BCL-2-associated X protein (Bax) and BCL-2-associated killer (Bak), have an essential role in cell death triggered by diverse cell death stimuli through the mitochondria,12, 15 we monitored Bax and Bak activation, which is necessary for mitochondrial outer membrane permeabilization and transduction of the cell death signal by the mitochondria. Upon activation, Bax translocates from the cytosol to the mitochondrial outer membrane and forms a self-oligomer, and Bak, which is originally localized to the mitochondrial outer membrane, also forms a pore-forming oligomer in the mitochondrial outer membrane.16 Therefore, we monitored Bax translocation and Bax or Bak oligomerization. As a result, in response to CB irradiation, Bax translocation from the cytosol to the mitochondria was detected, and self-oligomerization of Bax and Bak was also confirmed (Figure 2a). Next, to determine whether Bax and/or Bak is essential for CB-induced glioma cell death, we knocked down Bax and/or Bak with siRNAs and also established T98G/U251 cells stably overexpressing Bcl-2 and B-cell lymphoma-extra large (Bcl-xl), which antagonize Bax and Bak,12 and examined their effect on CB-induced caspase activation and cell death. Both in microscopic images and quantitation by nuclear staining, CB irradiation-induced glioma cell death was effectively suppressed not only by Bcl-2 or Bcl-xl overexpression but also by the double knockdown of Bax and Bak, whereas single knockdown of Bax or Bak caused partial inhibition. Essentially similar results were obtained with respect to CB-induced cytochrome c release from the mitochondria and caspase activation including caspase-8 activation (Figure 2b). Thus, it was indicated that both Bax and Bak are essential for CB irradiation-induced glioma cell death and that caspases, including caspase-8, are activated downstream of mitochondrial proapoptotic Bcl-2 family protein activation. In this study, we also sought to further examine the contribution of caspases upstream of mitochondrial Bax and Bak activation. Therefore, self-oligomerization of Bax and Bak after CB irradiation in the presence of pan-caspase inhibitors or specific caspase inhibitors was monitored. As a result, in T98G cells, CB irradiation-induced oligomerization of Bax was not affected by either pan-caspase or specific caspase inhibitors, whereas pan-caspase inhibitors suppressed Bax oligomerization in U251 cells (Supplementary Figure 2).

CB irradiation induces mitochondrial Bax and Bak activation upstream of caspase activation, including caspase-8, in T98G and U251 glioma cells. (a) (Upper panels) T98G and U251 cells were treated with or without CB irradiation (5 Gy), and after 48 h, the cell lysates obtained were fractionated into cytosol- and mitochondria-rich fractions. Each fractionated protein sample was then subjected to immunoblotting using anti-Bax and anti-Bak antibodies to monitor the cytosol–mitochondrial translocation of Bax and Bak. To confirm equal protein loading of each fraction, the membranes were reprobed using an anti-α-tubulin (for the cytosol) or anti-HSP60 (for the mitochondria) antibody. As a control of irradiation- or DNA damage-induced responses, cell lysates of T98G and U251 cells obtained at the indicated time points after irradiation by X-ray (20 Gy) or UV-C (UV, 200 J) were fractionated and subjected to immunoblotting in the same manner. (Lower panels) T98G and U251 cells were treated as indicated, and the cell lysates obtained were subjected to an in vitro cross-linking assay using the BMH cross-linker, as described in the ‘Materials and methods’ section. The cross-linked protein lysates were then subjected to immunoblotting using anti-Bax and anti-Bak antibodies for the detection of Bax and Bak oligomers. As a protein loading control, immunoblotting of proteins from the same samples treated with vehicle (DMSO) instead of cross-linker using anti-Bax and anti-Bak antibodies was also performed. (b) T98G and U251 cells transfected with control siRNA (Si-control), Bax siRNA (Si-Bax), Bak siRNA (Si-Bak), or Bax and Bak siRNAs (Si-Bax+Bak) as described in the ‘Materials and methods’ section, or stably overexpressing empty vector (PCDNA3), Bcl-2 (PCDNA3 Bcl-2), or Bcl-xl (PCDNA3 Bcl-xl) were subjected to CB irradiation (5 Gy). After 48 h, cells were harvested and total cell lysates were subjected to immunoblotting using the indicated anti-caspase antibodies. Immunoblotting of the same samples using anti-Bax, anti-Bak, anti-Bcl-2, and anti-Bcl-xl antibodies was also performed to monitor the efficiency of knockdown or overexpression of each protein. The membranes were reprobed using an anti-α-tubulin antibody to confirm equal protein loading (upper). Quantitation of cell death was also performed (lower), as described in panel b (*P<0.05)
The MEK–ERK cascade positively regulates CB irradiation-induced cell death
As the involvement of MAPKs has been highlighted recently in various cell death-inducing models, including conventional irradiation-induced glioma cell death,17 we next explored the involvement of MAPKs in CB irradiation-induced glioma cell death. First, we investigated by immunoblotting analysis the phosphorylation (=activation) status of three major MAPKs: extracellular signal-regulated kinase (ERK), p38 MAPK, and c-Jun N-terminal kinase (JNK), which have been reported previously as being correlated with cell death induction. As a result, the dynamic activation of ERK and p38, but not of JNK, was observed during 96 h after CB irradiation (Figure 3a). Therefore, we presumed that ERK or p38 MAPK is involved in CB-induced glioma cell death. To test this idea, we conducted knockdown experiments using siRNAs against p38alpha, which constitutes the major p38 isoform, and against mitogen-activated protein kinase kinase (MEK)1 and MEK2, which act immediately upstream of ERK activation.18 As shown in Supplementary Figure 3a, knockdown of p38alpha or MEK1/2 specifically downregulated the expression of its respective target and also suppressed the activation of p38MAPK and ERK1/2, respectively. In addition, MEK1/2 knockdown inhibited CB irradiation-induced glioma cell death at 48 h, although p38alpha knockdown rather increased CB-induced T98G and U251 cell death (Figure 3b). Next, because we wanted to ask whether the kinase activity of ERK is essential for CB-induced glioma cell death, we established T98G and U251 cells stably expressing a dominant-negative (DN) ERK2 (Supplementary Figure 3b). T98G and U251 cells stably expressing the DN ERK2 effectively inhibited CB-induced cell death compared with nontransfected cells or cells stably transfected with the empty vector (Figure 3c). Collectively, these data suggest that the kinase activity of ERK is essential for glioma cell death. On the basis of these results, we further examined the impact of MEK1/2 and p38alpha knockdown on mitochondria-mediated CB-induced glioma cell death signaling. MEK1/2 knockdown, but not p38alpha knockdown, inhibited caspases activation, Bax and Bak activation, and cytochrome c release at 48 h in both cell lines (Figure 3d). Together with these results, it was considered that the MEK–ERK pathway regulates CB irradiation-induced glioma cell death upstream of the mitochondria.

The MEK–ERK pathway is essential for CB irradiation-induced T98G and U251 glioma cell death. (a) T98G and U251 cells were treated with or without CB irradiation (5 Gy), and the cells were harvested at the indicated time points. Total cell lysates were then subjected to immunoblotting using the indicated antibodies. As a positive control of JNK activation, total cell lysates of both cell lines obtained 10 min after UV-C (200 J) irradiation were also analyzed by immunoblotting. The membranes were reprobed using an anti-α-tubulin antibody to confirm equal protein loading. (b) T98G and U251 cells transfected with the indicated siRNAs were treated with or without CB irradiation (5 Gy) and subjected to quantitation of cell death 48 h after irradiation (*P<0.05). (c) T98G and U251 cells untransfected or stably transfected with a control vector (Vector) or a dominant-negative ERK2 expression vector were treated with or without CB irradiation (5 Gy) and subjected to quantitation of cell death 48 h after irradiation. (d) T98G and U251 cells transfected with control siRNA, MEK1, and MEK2 siRNA (set1), or p38alpha siRNA (set1) were treated with CB irradiation (5 Gy), and after 48 h, the total cell lysates obtained were analyzed by immunoblotting as described in panel b for the detection of caspase activation (upper). Cross-linked or noncross-linked cell lysates were assayed by immunoblotting for the detection of Bax or Bak oligomers (middle). The obtained cell lysates were fractionated and analyzed by immunoblotting for the detection of cytochrome c release from the mitochondria into the cytosol (lower)
Recovery of activation at 2–36 h, but not later than 36 h after CB irradiation, of ERK is essential for CB irradiation-induced cell death
As ERK activation in CB-irradiated glioma cells changed dynamically, we hypothesized that the kinetics of ERK activation has different roles in CB irradiation-induced glioma cell death. We noticed three different peaks (0–2, 2–48, and after 48 h) of ERK phosphorylation in CB-irradiated glioma cells (Figure 3a), and, to test our hypothesis, we tried to suppress each peak of ERK activation using two different MEK-specific inhibitors, as shown schematically in Figure 4a. Consistent with earlier results (Figure 3), these inhibitors, when present in the culture medium throughout the assay period (protocol 4), blocked CB irradiation-induced glioma cell death signal upstream of the mitochondria and, consequently, cell death itself (Figure 4b). We then found that CB irradiation-induced Bax oligomerization, cytochrome c release from the mitochondria into the cytosol, caspase-3 activation, and cell death are efficiently inhibited by protocol 2 (15 min to 36 h treatment by inhibitors) and slightly by protocol 3 (treatment by inhibitors after 36 h) in both glioma cell lines (Figure 4c). Collectively, these results suggested that the recovery of ERK activation during the first 36 h after CB irradiation is the most important period for CB irradiation-induced glioma cell death.

Recovered activation of ERK at 2–36 h after CB irradiation is essential for CB-induced T98G and U251 glioma cell death. (a) Treatment protocols for MEK inhibitors (U0126 (U0, 20 μM) or PD98059 (PD, 20 μM)). Protocol 1 (for selective inhibition of ERK activity at the time of CB irradiation): the inhibitors were present in the culture medium from 2 h before and to 30 min after irradiation. Protocol 2 (for selective inhibition of ERK activity recovery occurring 2–36 h after irradiation): the inhibitors were present 15 min to 36 h after irradiation. Protocol 3 (for selective inhibition of ERK activity later than 36 h after irradiation): the inhibitors were added to the medium at 36 h after irradiation. Protocol 4 (for inhibition of ERK activity throughout the assay period): the inhibitors were added to the culture medium 2 h before irradiation. (b) T98G and U251 cells treated and harvested as indicated in protocol 4 were subjected to quantitation of cell death (*P<0.05), and were also analyzed for caspase-3 activation, Bax and Bak oligomerization, and cytochrome c release from the mitochondria into the cytosol. (c) T98G and U251 cells were treated as shown in protocols 1–3. A cell death assay (*P<0.05), analysis for the detection of caspase-3 activation, Bax oligomerization, and cytochrome c release from the mitochondria into the cytosol were thereafter carried out
Stimulation of the ERK cascade enhances CB irradiation-induced glioma cell death
With a therapeutic view to these results, it was important to verify whether glioma cells are killed by CB irradiation more efficiently by applying an ERK-mediated mechanism. Therefore, to test this idea, we used an ERK cascade initiator, epidermal growth factor (EGF),19 and monitored whether EGF enhanced CB irradiation-induced glioma cell death. As a result, CB-irradiated glioma cells pretreated with EGF indicated a continuous activation of ERK compared with CB treatment alone (Figure 5a). In addition, cell death, Bax oligomerization, and caspase-3 activation were significantly enhanced by EGF pretreatment, which was effectively inhibited by different MEK inhibitors (Figure 5b and c; Supplementary Figure 4). Thus, it was suggested that stimulation of the ERK cascade could augment CB irradiation-induced glioma cell death.

Forced sustained activation of ERK by EGF stimulation enhances CB irradiation-induced T98G and U251 glioma cell death. (a) T98G and U251 cells were treated by CB irradiation (5 Gy) with or without EGF (100 ng/ml). The cells were then harvested at the indicated time points, and the total cell lysates obtained were analyzed by immunoblotting to monitor the status of ERK activation. (b) T98G and U251 cells were treated by CB irradiation (5 Gy) with or without EGF treatment (100 ng/ml) in the presence or absence of vehicle (DMSO), U0126 (U0, 20 μM), or PD98059 (PD, 20 μM). At 48 h after irradiation, analysis for the detection of caspase-3 activation or Bax oligomerization was performed. (c) T98G and U251 cells were treated by CB irradiation (5 Gy) with or without EGF (100 ng/ml) in the presence or absence of U0126 (U0, 20 μM) or PD98059 (PD, 20 μM). After 72 h, photomicrographs of phase-contrast images ( × 100) were then obtained using a microscope (left), and cell death was assayed (*P<0.05)
Limited dependence of X-ray-induced glioma cell death on the MEK–ERK pathway
One of the most important questions in CB irradiation-induced glioma therapy is whether CB irradiation kills glioma cell by a different mechanism compared with X-ray or photon radiotherapies. As a preliminary study, we found that 20 Gy of X-ray induced T98G and U251 cell death at 72 h after irradiation, which was nearly the same as 48 h after 5 Gy of CB irradiation in glioma cell death induction (data not shown). Therefore, we used this condition of X-ray irradiation. To investigate the contribution of MEK–ERK cascade to X-ray-induced glioma cell death, we first monitored the activation status of ERK1/2 after X-ray irradiation. The activation status of ERK changes dynamically for 72 h after X-ray irradiation in both T98G and U251 cells (Figure 6a), although the time kinetics were different from those of CB irradiation (Figure 3a). From this result, we presumed that the MEK–ERK cascade might also be involved in X-ray-induced glioma cell death similar to CB-induced glioma cell death. Therefore, as a next step, we tested the effect of MEK inhibitors on X-ray-induced glioma cell death. When X-ray-irradiated T98G/U251 cells were concomitantly treated with MEK inhibitors, cell death was not affected significantly in either glioma cell line, which was not same as the case of CB irradiation (Figure 6b). Furthermore, T98G and U251 cells stably expressing a DN ERK2 did not show significantly reduced caspase-3 activation and cell death after X-ray-irradiation compared with control cells (Figure 6c). These results suggested that the MEK–ERK cascade may have a predominant role in CB-induced glioma cell death compared with X-ray-induced glioma cell death.

The MEK–ERK pathway may not be essential for X-ray irradiation-induced T98G and U251 cell death. (a) T98G and U251 cells were treated with or without X-ray irradiation (20 Gy), and the cells were harvested at the indicated time points. Total cell lysates were then subjected to immunoblotting using an anti-total ERK1/2 or phospho-ERK1/2 antibody. Results of different exposure times of phospho-ERK1/2 blot are presented for U251. The membranes were reprobed using an anti-α-tubulin antibody to confirm equal protein loading. (b) T98G and U251 cells were treated with or without X-ray irradiation (20 Gy) in the presence or absence of vehicle (DMSO), U0126 (U0, 20 μM), or PD98059 (PD, 20 μM). At 72 h after irradiation, quantitation of cell death was then performed. (c) T98G and U251 cells stably expressing a dominant-negative ERK2 (DN1, DN2) and their control transfectants were treated with X-ray irradiation (20 Gy). At 72 h after irradiation, quantitation of cell death was then performed (upper), or obtained total cell lysates were subjected to immunoblotting using an anti-caspase-3 antibody (lower). The membranes were reprobed using an anti-α-tubulin antibody to confirm equal protein loading
Discussion
Although the clinical efficacy of CB-irradiation therapy has been proven by numerous studies,1, 2 examination of the detailed molecular effect of CB irradiation on glioma cells is still unclear. In this study, we showed that CB irradiation-mediated glioma cell death, especially within 48 h after irradiation, is pure apoptosis by ERK phosphorylation, mitochondrial proapoptotic Bcl-2 family protein activation, followed by the activation of caspases. In addition, to the best of our knowledge, this is the first report on the detailed molecular mechanism of CB irradiation-induced glioma cell death, including the type of cell death and the detailed molecular induction mechanism.
In the case of conventional irradiation, in most cases, irradiated tumor cells have been reported to undergo apoptosis.9 Histological analysis of human tumor specimens also showed necrotic changes as a result of high-dose irradiation.10 Furthermore, the involvement of autophagic cell death was found in photon irradiation-induced glioma cell suicide.11 Therefore, in addition to apoptosis, we first expected that such changes would also occur in CB-irradiated glioma cells. However, at least within the first few days after CB irradiation, necrotic cell death did not occur in glioma cells. Despite increases in autophagic changes being confirmed in CB-irradiated T98G cells, inhibition of autophagy did not affect cell death (AT and CK, unpublished observation). Therefore, we considered that the majority of characteristics of CB irradiation-induced glioma cell death are consistent with apoptosis.
The involvement of transcription factor p53 in conventional radiation-induced tumor cell growth arrest/death is generally recognized, and the efficacy of the p53 gene in the case of CB irradiation has also already been shown.20, 21 However, tumor cells with wild-type p53 could have the potential to be treated effectively by conventional radiation. Furthermore, radioresistant gliomas have been reported to have a tendency for mutations in the p53 gene.22 Therefore, we used p53-mutated glioma cell lines in this study to also investigate the detailed molecular mechanism associated with one of the advantages of CB irradiation reported previously;23, 24, 25 how CB irradiation kills p53-mutated tumor cells efficiently.
The activation of specified caspase cascades after various cell stress stimulation is still ambiguous. In the case of conventional irradiation especially, the involvement of the intrinsic pathway, the extrinsic pathway, or both have already been reported.9 In the meantime, only the apoptotic pathway induced by CB irradiation by intrinsic caspase-9 and caspase-3 activation in p53 wild-type/mutant cells has been reported.23 In addition, studies on the involvement of extrinsic caspase-8 and supra-mitochondrial involvement of caspases in CB irradiation-induced tumor cell death had not been examined before this study, to the best of our knowledge. One difficult result to comprehend is that pan-caspase inhibitors blocked not only caspase activation but also Bax activation in CB irradiation-induced U251 cell death. To clear this question, two hypotheses were suggested. First, these pan-caspase inhibitors block an unknown caspase(s) that works upstream of the mitochondria in multiple cell death-inducing systems of U251 cells, and second, these inhibitors work by an unexpected mechanism other than caspase inhibition in U251 cells, as indicated in previous reports.26, 27, 28 Neither of these potential mechanisms was demonstrated in the present experimental system, but there is little doubt that major known caspases are not involved in the regulation of CB irradiation-induced glioma cell death upstream of the mitochondria in T98G or U251 cells. Another interesting finding about the caspase-activation mechanism in this study was caspase-8 activation downstream of the mitochondria. Recently, caspase-6 was reported to mediate caspase-3-induced caspase-8 activation downstream of the mitochondria.29 Therefore, in the present system, involvement of the same caspase-8-activating mechanism could be considered.
The role of ERK in cell death often focuses on its prosurvival function by the downstream transcription of antiapoptotic genes and downregulation of proapoptotic genes. However, the proapoptotic action of ERK has been also reported in different systems. Among these proapoptotic ERK mechanisms, the relationship with reactive oxygen species (ROS)-mediated cell death induction, which is explained by ROS-induced ERK activation after cell death, has been most frequently mentioned.18, 19, 20, 21, 22, 24, 25, 26, 27, 28, 29, 30, 31 However, in the present model, neither ROS production (Supplementary Figure 5a) nor the inhibitory effect of antioxidants in CB irradiation-induced glioma cell death was confirmed (Supplementary Figure 5b). Thus, unlike cell death induced by other high-dose DNA damage stresses, which induce ROS-dependent cell death, it was suggested that gliomas do not produce ROS even after a maximum clinical dose of CB irradiation, which may be related to the refractory nature against standard radiotherapy.
In this study, the recovered activation of ERK observed 2–48 h after CB irradiation was considered to have an essential role in CB irradiation-induced glioma cell death (Figure 4). However, it should be noted that this peak is not hyperactivation but recovery of activity up to the baseline (unstimulated) level in both glioma cell lines. A previous report indicated a time-dependent increase in ERK activity from the baseline level corresponding to its cell death-inducing ability.32 Furthermore, in the present data, even the complete suppression of ERK by U0126 did not prevent cell death completely (Figure 4b), whereas pan-caspase inhibitors inhibited CB irradiation-induced glioma cell death nearly completely (Figure 1d). Thus, at least in the present model, it was suggested that an ERK-independent pathway could also contribute to CB irradiation-induced glioma cell death.
In considering the mechanism of radiation-induced cell death, the involvement of receptor-mediated extrinsic cell death signals, especially those related to Fas-mediated cell death, have been demonstrated previously,33 and ERK-dependent regulation of Fas-mediated cell death was also demonstrated.32 Thus, we expected the involvement of the Fas-mediated extrinsic pathway of apoptosis in the present system. In addition, we found that the Fas-mediated signal was activated both in T98G and in U251 cells on CB irradiation and was regulated by an ERK-dependent mechanism (Supplementary Figure 6a). However, an antagonistic-Fas antibody failed to prevent CB irradiation-induced cell death in T98G or U251 cells (Supplementary Figure 6b). Therefore, in the present system, the CB irradiation-induced Fas-mediated extrinsic pathway of apoptosis was not essential for cell death induction.
Our data on the EGF-mediated enhancement of CB irradiation-induced glioma cell killing (Figure 6) was surprising because in many cases, higher expression of its receptor EGFR has been described to reflect cell refractoriness to radiotherapy and chemotherapy.7, 34 Usually, EGF stimulation-mediated cell survival mechanisms are explained as being ERK dependent.35 However, as described above, ERK activation has the potential to have a different role in cell fate against cell stress by different stimuli, even when using the same cells. Indeed, the preliminary data showed that UV-C induced both hyperactivation of ERK and cell death in T98G and U251 cells, but this was not prevented by MEK inhibitors (data not shown), and X-ray-induced cell death of both glioma cell lines was also only minimally sensitive to ERK pathway inhibition (Figure 6). Thus, ERK-mediated augmentation of glioma cell killing may be specific to CB irradiation, and applying a novel ERK-dependent CB irradiation-induced glioma cell death mechanism in this study, namely the addition of an ERK agonist treatment to CB therapy (Figure 7), may improve the clinical outcome of malignant glioma treatment compared with treatment by CB irradiation alone.

Schematic summary of the present findings. On the basis of the results of the current study, we propose that CB irradiation triggers reactivation of the MEK–ERK pathway subsequent to initial downregulation, which then initiates the mitochondrial pathway of caspase cascade activation, culminating in apoptotic death of glioma cells. Molecules involved in this cell death signaling pathway could be new targets for augmentation of CB therapy against gliomas. For instance, EGF may be used for MEK–ERK pathway activation, ABT-737 for the activation of mitochondrial apoptosis, and SMAC mimetics for caspase cascade activation
In conclusion, we found in this study that p53-independent glioma cell death induced by CB irradiation is regulated through an MEK–ERK–mitochondria–caspase cascade that may be key to improvement in the clinical outcome of glioma therapy by radiation. Recently, effective Bcl-2-specific antagonists36 or inhibitors of IAP family proteins,37 which abrogate caspase activation downstream of the mitochondria, have been developed. Therefore, treatment by CB irradiation concomitant with ERK agonists alone or in combination with these inhibitors (Figure 7) could be a more effective method of treating radioresistant glioma.
Materials and Methods
Reagents and antibodies
U0126 was purchased from A. G. Scientific (San Diego, CA, USA). Human recombinant EGF was purchased from R&D System (Minneapolis, MN, USA). Hoechst 33342 and PD98059 were purchased from Sigma (St Louis, MO, USA). Tumor necrosis factor-α was purchased from Genzyme-Techne (Minneapolis, MI, USA). A23187, Boc-Asp-fmk, cycloheximide, N-acetylcysteine, Trolox, anti-β-tubulin antibody, and anti-p53 antibody were obtained from Calbiochem (San Diego, CA, USA). Anti-ERK2 antibody, polyclonal anti-Bak antibody (G-23), polyclonal anti-Bax antibody (N-20), anti-Bcl-2 antibody (N-19), anti-total JNK2 antibody, and horseradish peroxidase-conjugated anti-goat IgG secondary antibodies were from Santa Cruz Biotechnology (Santa Cruz, CA, USA). Anti-Bid antibody, anti-Bip (GRP78) antibody, anti-cytochrome c antibody, anti-caspase-3 antibody, anti-caspase-8 antibody, anti-caspase-9 antibody, anti-total ERK1/2 antibody, anti-phospho-ERK1/2(Thr180/Tyr182) antibody, anti-MEK1 antibody, anti-MEK2 antibody, anti-total p38MAPK antibody, anit-phospho-p38MAPK(Thr202/Tyr204) antibody, anti-phospho-JNK(Thr183/Tyr185) antibody, and anti-PARP antibody were from Cell Signaling Technology (San Jose, CA, USA). Bismaleimidohexane (BMH) and a bicinchoninic acid (BCA) protein assay kit were from Thermo Scientific (Rockford, IL, USA). Anti-Fas antibody and anti-FADD antibody were purchased from BD Transduction Laboratories (Mississauga, ON, Canada). z-VAD-FMK, Ac-DEVD-CHO, AC-LEHD-CHO, and AC-IETD-CHO were purchased from Peptide Institute Inc. (Osaka, Japan). Antagonistic anti-Fas antibody was from MBL (Nagoya, Japan). PI solution, 2′,7′-dichlorodihydrofluorescein diacetate (DCFDA) was from Invitrogen (Eugene, OR, USA). Lipofectamin 2000 was from Qiagen (Hilden, Germany). QuikChange II site-directed mutagenesis kit was from Stratagene (La Jolla, CA, USA). Human placenta total RNA was from Clontech (Mountain View, CA, USA).
siRNAs
Control siRNA, Bax siRNA, MEK1 siRNA, MEK2 siRNA, and p38α siRNA were purchased from Invitrogen. The sequences of siRNAs for the indicated target genes were as follows;
Bax: 5′-UUGAGCACCAGUUUGCUGGCAAAGU-3′;
MEK1 no.1: 5′-AAUUCCAGACUGAACACUCCACUGG-3′;
MEK1 no.2: 5′-AAAGUCGUCAUCCUUCAGUUCUCCC -3′;
MEK2 no.1: 5′-UUUAUUGACAAACUCCUGGAAGUCG-3′;
MEK2 no.2: 5′-UUGUGAGCAUCUUCAGGUCCGCCCG-3′;
p38α no.1: 5′-AAACAAUGUUCUUCCAGUCAACAGC-3′;
p38α no.2: 5′-UUAGGUCCCUGUGAAUUAUGUCAGC-3′.
Bak siRNA was purchased from Qiagen. The sequence was 5′-AAGCGAAGTCTTTGCCTTCTC-3′.
Cell lines and cell culture
Human glioblastoma cell lines T98G (purchased from Riken Bioresource Center, Tsukuba, Ibaragi, Japan) and U251 (a kind gift from Dr. Mark L Rosenblum, UCSF, San Francisco, CA, USA) seeded in a T25 flask (Corning, NY, USA) were cultured at 37°C in a humidified 5% CO2 incubator and were grown in standard Dulbecco's modified Eagle's medium supplemented with 10% (v/v) fetal bovine serum and antibiotics (100 Units/ml penicillin, 100 μg/ml streptomycin) at Yamagata University School of Medicine (Yamagata, Japan). On the day before CB irradiation, cell growing-flasks were boxed in thermal cases and carefully carried to the National Institute of Radiologic Science (NIRS) by express delivery. The cells were then cultured in a CO2 incubator at NIRS continuously before irradiation.
For X-ray irradiation, cells were cultured in 10 cm culture dishes at Yamagata University School of Medicine.
Irradiation
CB irradiation (290 MeV, 6 cm spread-out Bragg peak (SOBP)) was performed using the heavy ion accelerator in Chiba (HIMAC) at the NIRS as described previously.23 Cell culture flasks were fixed vertically in the center of the SOBP, and accelerated carbon ions (1–10 Gy) were irradiated using the protocol compatible with the flask structure by horizontal beam. After irradiation, cells scheduled for assay 24 h or later after irradiation were immediately trypsinized and passaged into culture dishes, which were kept culturing again in a CO2 incubator for the following experiments. Cells scheduled for assay within 24 h after irradiation were kept maintained in the irradiated flask in a CO2 incubator.
The reference radiation was X-rays and the radiation dose was measured using an ionization chamber, and UV-C was delivered automatically in a Spectrolinker XL-1000 (Spectronics Corporation, Westburg, NY, USA) after aspiration of the culture medium.
Construction of plasmids
An expression vector for DN MAPK kinase (MEK–ERK–KR) was constructed as described previously with slight modifications.38 Human placenta total RNA was reverse transcribed. cDNAs encoding the ERK2 and MEK1 were subcloned into pcDNA3 vector. Mutagenesis of K54 in the human ERK2 to arginine and of the four leucine residues in the human MEK1 nuclear export sequence to alanine was performed using a QuikChange II site-directed mutagenesis kit. Expression vectors for Bcl-2 and Bcl-xl were constructed as described previously.39
Transfection
Transfection of siRNAs or plasmids into glioma cells was performed using Lipofectamin 2000 in accordance with the manufacturer's protocol. When transfection was performed combined with CB irradiation, transfection was performed 6 h before CB irradiation, and in the case of UV irradiation, it was performed 24 h before UV irradiation. For siRNA transfection, a 150 nM siRNA per array was used. Stable T98G or U251 transfectants by transfecting both cells with pcDNA3 vectors, and selection of transfectants was carried out using G418. For each transfectant, multiple clones expressing the intended protein were subjected to the subsequent analyses, and essentially similar results were obtained from multiple clones. Therefore, for each transfectants, results from two representative clones are presented.
Cell death and apoptosis assays
Cell death and apoptosis were assayed at the time points indicated in the figure legends after treatment with cell death stimuli. Cell death was detected based on the inability of cells to exclude vital dye PI. In brief, 4.0 μg/ml PI and 100 μM Hoechst 33342 were added to the cell culture medium directly at the time point of the assay, and the cells were cultured in a CO2 incubator for 10 min. The cellular nuclei were then stained with Hoechst 33342 and PI were counted independently using a fluorescence microscope (CKX41; Olympus, Tokyo, Japan; at least 500 cells per sample were assayed), and the percentage of PI-positive cells to total Hoechst-positive cells was calculated. For quantitation of apoptosis, cells were stained with Hoechst 33342 and PI as described above, and the percentage of apoptotic cells, in which the nuclei were PI positive in addition to being condensed and fragmented, to total Hoechst-positive cells was determined (at least of 500 cells per sample were assayed).
Preparation of cell lysate, cell fractionation, and immunoblotting
Whole-cell lysates were obtained as described previously.16 Cell fractionation was also performed as described previously16 with minor modifications. In brief, pelleted cells were permeabilized for 1 min in isotonic buffer containing 0.03% digitonin for 5 min on ice and then centrifuged at 15 000 × g for 10 min. The supernatant (cytosolic fraction) and the pellet (mitochondrial fraction) were collected, and the pellet was further lysed as the final mitochondrial lysate. For immunoblotting, the protein concentration of the lysates was determined using a BCA protein assay kit in accordance with the manufacturer's instructions. Equal amounts of protein were separated by 8–15% SDS-PAGE and then transferred onto a PDVF membrane. Membranes were blocked at room temperature for 1 h in blocking buffer (5% skim milk and 0.1% Tween 20 in TBS (TBS-T), 1:500 dilution) and then incubated overnight with a primary antibody (1:1500 dilution) diluted in blocking buffer at 4°C. The membranes were then washed three times with TBS-T, incubated with a peroxidase-conjugated secondary antibody diluted in the antibody buffer (1:10 000 dilution) at room temperature for 1 h, and washed three times with TBS-T. Membrane-bound antibodies were visualized using western chemiluminescent HRP substrate.
In vitro cross-linking for the detection of Bax and Bak oligomers
In vitro cross-linking of associated Bax or Bak monomers was performed according to the method reported previously16 with some modifications. In brief, collected cells were lysed in cross-linking buffer (10 mM HEPES (pH 7.5), 10 mM KCl, 1.5 mM MgCl2, 1 mM EDTA, 1 mM EGTA, 1 mM dithiothreitol, 250 mM sucrose, 2% CHAPS) on ice for 30 min, and then BMH dissolved in DMSO was added to a final concentration of 10 mM. After incubation for 30 min at room temperature with rotation, the lysate was centrifuged at 15 000 × g for 10 min. The supernatant was collected as cross-linked lysate, and after determination of the protein concentration using a BCA protein assay kit, the lysate was subjected to immunoblotting analysis using polyclonal anti-Bax and anti-Bak antibodies. Formation of homo-oligomers was judged by their molecular weight.16
Quantitation of active caspase-3/Bax oligomerization
For quantitation of caspase-3 activation and Bax oligomerization, densitometric analysis of cleaved caspase-3 and Bax oligomerized (dimer) bands was performed using Quantity One software (Bio-Rad, Tokyo, Japan). The results were normalized to α-tubulin for cleaved caspase-3 and to HSP60 (heat-shock protein 60) for Bax dimer.
DNA ladder formation assay
DNA ladder formation assay was performed as described previously.40 A total of 1 × 107 cells were used for each sample.
Measurement of the levels of intracellular ROS
Detection of intracellular ROS by DCFDA was performed as we reported previously.16 Visualization and calculation of intracellular ROS was performed using a fluorescence microscope (CKX41; Olympus, Tokyo, Japan) and DPController software (Olympus) using a manual protocol (single exposure, exposure time 0.1 s).
Statistical analysis
For all experiments with quantitative results, data are expressed as mean and S.D. from three identical experiments. Difference of means was tested by Student's t-test using Microsoft Excel 2007 software (Microsoft Corp., Richmond, WA, USA). P-values <0.05 were considered statistically significant.
Abbreviations
- Bak:
-
BCL-2-associated killer
- Bax:
-
BCL-2-associated X protein
- Bcl-2:
-
B-cell CLL/lymphoma 2
- Bcl-xl:
-
B-cell lymphoma-extra large
- Bid:
-
Bcl-2 interacting domain death agonist
- Boc:
-
Boc-D-FMK
- CB:
-
carbon beam
- DEVD:
-
Ac-DEVD-CHO
- DN:
-
dominant negative
- EGF:
-
epidermal growth factor
- ERK:
-
extracellular signal-regulated kinase
- HSP60:
-
heat-shock protein 60
- IETD:
-
Ac-IETD-CHO
- JNK:
-
C-JUN N-terminal kinase
- LEHD:
-
Ac-LEHD-CHO
- MAPK:
-
mitogen-activated protein kinase
- MEK:
-
mitogen-activated protein kinase kinase
- PARP:
-
poly(ADP-ribose) polymerase
- PD:
-
PD98059
- U0:
-
U0126
- UV:
-
ultraviolet
- VAD:
-
z-VAD-FMK
References
Fukumura A, Tsujii H, Kamada T, Baba M, Tsuji H, Kato H et al. Carbon-ion radiotherapy: clinical aspects and related dosimetry. Radiat Prot Dosimetry 2009; 137: 149–155.
Tsujii H, Mizoe JE, Kamada T, Baba M, Kato S, Kato H et al. Overview of clinical experiences on carbon ion radiotherapy at NIRS. Radiother Oncol 2004; 73 (Suppl 2): S41–S49.
Blakely EA, Kronenberg A . Heavy-ion radiobiology: new approaches to delineate mechanisms underlying enhanced biological effectiveness. Radiat Res 1998; 150 (5 Suppl): S126–S145.
Masunaga S, Ando K, Uzawa A, Hirayama R, Furusawa Y, Koike S et al. Radiobiologic significance of response of intratumor quiescent cells in vivo to accelerated carbon ion beams compared with gamma-rays and reactor neutron beams. Int J Radiat Oncol Biol Phys 2008; 70: 221–228.
Suzuki M, Kase Y, Yamaguchi H, Kanai T, Ando K . Relative biological effectiveness for cell-killing effect on various human cell lines irradiated with heavy-ion medical accelerator in Chiba (HIMAC) carbon-ion beams. Int J Radiat Oncol Biol Phys 2000; 48: 241–250.
Noda SE, Lautenschlaeger T, Siedow MR, Patel DR, El-Jawahri A, Suzuki Y et al. Technological advances in radiation oncology for central nervous system tumors. Semin Radiat Oncol 2009; 19: 179–186.
Mizoe JE, Tsujii H, Hasegawa A, Yanagi T, Takagi R, Kamada T, et al., Organizing Committee of the Central Nervous System Tumor Working Group. Phase I/II clinical trial of carbon ion radiotherapy for malignant gliomas: combined X-ray radiotherapy, chemotherapy, and carbon ion radiotherapy. Int J Radiat Oncol Biol Phys 2000; 69: 390–396.
Mizoe JE, Hasegawa A, Takagi R, Bessho H, Onda T, Tsujii H . Carbon ion radiotherapy for skull base chordoma. Skull Base 2009; 19: 219–224.
Belka C, Jendrossek V, Pruschy M, Vink S, Verheij M, Budach W . Apoptosis-modulating agents in combination with radiotherapy-current status and outlook. Int J Radiat Oncol Biol Phys 2004; 58: 542–554.
Perry A, Schmidt RE . Cancer therapy-associated CNS neuropathology: an update and review of the literature. Acta Neuropathol 2006; 111: 197–212.
Yao KC, Komata T, Kondo Y, Kanzawa T, Kondo S, Germano IM . Molecular response of human glioblastoma multiform cells to ionizing radiation: cell cycle arrest, modulation of the expression of cyclin-dependent kinase inhibitors, and autophagy. J Neurosurg 2003; 98: 378–384.
Hotchkiss RS, Strasser A, McDunn JE, Swanson PE . Cell death. N Engl J Med 2009; 361: 1570–1583.
Afshar G, Jelluma N, Yang X, Basila D, Arvold ND, Karlsson A et al. Radiation-induced caspase-8 mediates p53-independent apoptosis in glioma cells. Cancer Res 2006; 66: 4223–4232.
Rasheva VI, Domingos PM . Cellular responses to endoplasmic reticulum stress and apoptosis. Apoptosis 2009; 14: 996–1007.
Wei MC, Zong WX, Cheng EH, Lindsten T, Panoutsakopoulou V, Ross AJ et al. Proapoptotic BAX and BAK: a requisite gateway to mitochondrial dysfunction and death. Science 2001; 292: 727–730.
Tomiyama A, Serizawa S, Tachibana K, Sakurada K, Samejima H, Kuchino Y et al. Critical role for mitochondrial oxidative phosphorylation in the activation of tumor suppressors Bax and Bak. J Natl Cancer Inst 2006; 98: 1462–1473.
Dent P, Yacoub A, Fisher PB, Hagan MP, Grant S . MAPK pathways in radiation responses. Oncogene 2003; 22: 5885–5896.
Cagnol S, Chambard JC . ERK and cell death: mechanisms of ERK-induced cell death – apoptosis, autophagy and senescence. FEBS J 2009; 277: 2–21.
Ramos JW . The regulation of extracellular signal-regulated kinase (ERK) in mammalian cells. Int J Biochem Cell Biol 2008; 40: 2707–2719.
Duan X, Zhang H, Liu B, Li XD, Gao QX, Wu ZH . Apoptosis of murine melanoma cells induced by heavy-ion radiation combined with Tp53 gene transfer. Int J Radiat Biol 2008; 84: 211–217.
Liu B, Zhang H, Duan X, Hao J, Xie Y, Zhou Q et al. Adenovirus-mediated wild-type p53 transfer radiosensitizes H1299 cells to subclinical-dose carbon-ion irradiation through the restoration of p53 function. Cancer Biother Radiopharm 2009; 24: 57–66.
Gross MW, Kraus A, Nashwan K, Mennel HD, Engenhart-Cabillic R, Schlegel J . Expression of p53 and p21 in primary glioblastomas. Strahlenther Onkol 2005; 181: 164–171.
Yamakawa N, Takahashi A, Mori E, Imai Y, Furusawa Y, Ohnishi K et al. High LET radiation enhances apoptosis in mutated p53 cancer cells through caspase-9 activation. Cancer Sci 2008; 99: 1455–1460.
Mori E, Takahashi A, Yamakawa N, Kirita T, Ohnishi T . High LET heavy ion radiation induces p53-independent apoptosis. J Radiat Res (Tokyo) 2009; 50: 37–42.
Iwadate Y, Mizoe J, Osaka Y, Yamaura A, Tsujii H . High linear energy transfer carbon radiation effectively kills cultured glioma cells with either mutant or wild-type p53. Int J Radiat Oncol Biol Phys 2001; 50: 803–808.
Gamen S, Anel A, Pérez-Galán P, Lasierra P, Johnson D, Piñeiro A et al. Doxorubicin treatment activates a Z-VAD-sensitive caspase, which causes deltapsim loss, caspase-9 activity, and apoptosis in Jurkat cells. Exp Cell Res 2000; 258: 223–235.
Navakauskiene R, Treigyte G, Savickiene J, Gineitis A, Magnusson KE . Alterations in protein expression in HL-60 cells during etoposide-induced apoptosis modulated by the caspase inhibitor ZVAD. fmk. Ann N Y Acad Sci 2004; 1030: 393–402.
Navarro P, Valverde AM, Conejo R, Benito M, Lorenzo M . Inhibition of caspases rescues brown adipocytes from apoptosis downregulating BCL-XS and upregulating BCL-2 gene expression. Exp Cell Res 1999; 246: 301–307.
Inoue S, Browne G, Melino G, Cohen GM . Ordering of caspases in cells undergoing apoptosis by the intrinsic pathway. Cell Death Differ 2009; 16: 1053–1061.
Chen YC, Chow JM, Lin CW, Wu CY, Shen SC . Baicalein inhibition of oxidative-stress-induced apoptosis via modulation of ERKs activation and induction of HO-1 gene expression in rat glioma cells C6. Toxicol Appl Pharmacol 2006; 216: 263–273.
Kim HJ, Chakravarti N, Oridate N, Choe C, Claret FX, Lotan R . N-(4-hydroxyphenyl)retinamide-induced apoptosis triggered by reactive oxygen species is mediated by activation of MAPKs in head and neck squamous carcinoma cells. Oncogene 2006; 25: 2785–2794.
Liu J, Mao W, Ding B, Liang CS . ERKs/p53 signal transduction pathway is involved in doxorubicin-induced apoptosis in H9c2 cells and cardiomyocytes. Am J Physiol Heart Circ Physiol 2008; 295: H1956–H1965.
Huang HL, Fang LW, Lu SP, Chou CK, Luh TY, Lai MZ . DNA-damaging reagents induce apoptosis through reactive oxygen species-dependent Fas aggregation. Oncogene 2003; 22: 8168–8177.
Cancer Genome Atlas Research Network. Comprehensive genomic characterization defines human glioblastoma genes and core pathways. Nature 2008; 455: 1061–1068.
McCubrey JA, Steelman LS, Chappell WH, Abrams SL, Wong EW, Chang F et al. Roles of the Raf/MEK/ERK pathway in cell growth, malignant transformation and drug resistance. Biochim Biophys Acta 2007; 1773: 1263–1284.
Oltersdorf T, Elmore SW, Shoemaker AR, Armstrong RC, Augeri DJ, Belli BA et al. An inhibitor of Bcl-2 family proteins induces regression of solid tumours. Nature 2005; 435: 677–681.
Beauparlant P, Shore GC . Therapeutic activation of caspases in cancer: a question of selectivity. Curr Opin Drug Discov Devel 2003; 6: 179–187.
Robinson MJ, Stippec SA, Goldsmith E, White MA, Cobb MH . A constitutively active and nuclear form of the MAP kinase ERK2 is sufficient for neurite outgrowth and cell transformation. Curr Biol 1998; 8: 1141–1150.
Kitanaka C, Namiki T, Noguchi K, Mochizuki T, Kagaya S, Chi S et al. Caspase-dependent apoptosis of COS-7 cells induced by Bax overexpression: differential effects of Bcl-2 and Bcl-xL on Bax-induced caspase activation and apoptosis. Oncogene 1997; 15: 1763–1772.
Sellins KS, Cohen JJ . Gene induction by gamma-irradiation leads to DNA fragmentation in lymphocytes. J Immunol 1987; 139: 3199–3206.
Acknowledgements
We thank Dr. Takeshi Murakami at the National Institute of Radiological Sciences for continuous support. This study was performed as part of the Research Project of Heavy Ion Medical Accelerator in Chiba at the National Institute of Radiological Sciences (No. 19B349), and was supported by Grants-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology of Japan, by a Grant-in-Aid from the Global COE program of the Japan Society for the Promotion of Science, by a Grant-in-Aid for Cancer Research from the Ministry of Health, Labor, and Welfare of Japan, and by a grant from the Brain foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Edited by A Finnazzi-Agro
Supplementary Information accompanies the paper on Cell Death and Disease website
Supplementary information
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Tomiyama, A., Tachibana, K., Suzuki, K. et al. MEK–ERK-dependent multiple caspase activation by mitochondrial proapoptotic Bcl-2 family proteins is essential for heavy ion irradiation-induced glioma cell death. Cell Death Dis 1, e60 (2010). https://doi.org/10.1038/cddis.2010.37
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/cddis.2010.37
Keywords
This article is cited by
-
Dual blockade of EGFR and PI3K signaling pathways offers a therapeutic strategy for glioblastoma
Cell Communication and Signaling (2023)
-
Tau binding protein CAPON induces tau aggregation and neurodegeneration
Nature Communications (2019)
-
Hypoxia inducible factor-1α/B-cell lymphoma 2 signaling impacts radiosensitivity of H1299 non-small cell lung cancer cells in a normoxic environment
Radiation and Environmental Biophysics (2019)
-
Carbon Ion-Irradiated Hepatoma Cells Exhibit Coupling Interplay between Apoptotic Signaling and Morphological and Mechanical Remodeling
Scientific Reports (2016)
-
Carbon ion beam triggers both caspase-dependent and caspase-independent pathway of apoptosis in HeLa and status of PARP-1 controls intensity of apoptosis
Apoptosis (2015)
