
Abstract
Basal cell carcinoma (BCC) is a common malignancy with a good prognosis in the majority of cases. However, some BCC patients develop a more advanced disease that poses significant management challenges. Such cases include locally advanced, recurrent or metastatic BCC, or tumours that occur in anatomical sites where surgical treatment would result in significant deformity. Until recently, treatment options for these patients have been limited, but increased understanding of the molecular basis of BCC has enabled potential therapies, such as hedgehog signalling pathway inhibitors, to be developed. A clear definition of advanced BCC as a distinct disease entity and formal management guidelines have not previously been published, presumably because of the rarity, heterogeneity and lack of treatment options available for the disease. Here we provide a UK perspective from a multidisciplinary group of experts involved in the treatment of complex cases of BCC, addressing the key challenges associated with the perceived definition and management of the disease. With new treatments on the horizon, we further propose a definition for advanced BCC that may be used as a guide for healthcare professionals involved in disease diagnosis and management.
Similar content being viewed by others

Main
Basal cell carcinoma (BCC) is the most common malignancy in Caucasians (Lomas et al, 2012; Samarasinghe and Madan, 2012), with over two million estimated cases diagnosed in the United States of America each year and worldwide incidence continuing to rise on an yearly basis (Samarasinghe and Madan, 2012). Exposure to ultraviolet radiation is the greatest risk factor for the disease, although the relationship between the timing and amount of exposure to ultraviolet radiation and BCC has not been completely established (Wong et al, 2003).
Although the prognosis for patients with BCC is generally good, and metastasis is rare (Ting et al, 2005), a small but significant number of complex cases pose a disproportionate challenge for clinical management. Such cases include locally advanced tumours (particularly those that have developed in difficult-to-treat facial sites), aggressively recurrent tumours, large tumours that may have developed many years before presentation and those in which current treatment options are excluded by clinical or patient-driven criteria (Skvara et al, 2011; Sekulic et al, 2012). In recent years, improved understanding of pathological mechanisms and identification of potential targets for treatment has enabled novel targeted systemic agents to be developed (Skvara et al, 2011; Sekulic et al, 2012), and these are now available for patients diagnosed to have advanced disease.
However, classification of this patient subgroup with advanced disease has been inconsistent, presumably because of the rarity and heterogeneity of complex cases of BCC, and the limited treatment options available. In the scientific literature, a number of terms are used, including ‘severe’, ‘advanced’ and ‘aggressive’ BCC (Fernandes et al, 2010; Weinstock and Still, 2011). In the light of potential new therapeutic options, providing a standardised definition of this subgroup and guidance for identifying cases that may be appropriate for receiving new systemic therapies or clinical trial participation is timely. With this objective in mind, a multidisciplinary panel from the United Kingdom with expertise I dermatology, dermatologic surgery, plastic surgery and medical and clinical oncology was convened to review the published, peer-reviewed literature and, combined with collective clinical experience, to identify factors to be considered in the assessment and management of complex and advanced cases of BCC, including proposing a working clinical definition for this disease subtype.
Current management of BCC
Management of BCC depends on a number of factors including the size, site and histological subtype of the tumour, comorbidities, previous treatment history and patient preference. It is also important to consider whether the intention of treatment is curative or palliative.
Nodular BCCs, which make up over 60% of cases (Scrivener et al, 2002), are generally treated surgically, with clinical excision margins of 4 mm or more (Baxter et al, 2012). Superficial BCCs are treated using surgical or nonsurgical approaches, including topical agents such as 5-fluorouracil or imiquimod, that normally yield good clearance rates (Miller, 2000; Telfer et al, 2008). More recently, photodynamic therapy (PDT) with methylaminolaevulinate has been compared with topical imiquimod and topical fluorouracil in a randomised, single-blind study of 601 patients with superficial BCC. Imiquimod was shown to be superior to PDT, while topical fluorouracil was non-inferior to PDT, although 1-year tumour-free survival rates were approximately 70–80% in all groups. Cosmetic outcomes following treatment did not appear to differ significantly between therapies (Artis et al, 2013; Dummer, 2013). More invasive BCC subtypes, such as infiltrative or morphoeic BCC, or large lesions and those in cosmetically sensitive sites in which tissue sparing is critical, can be treated with Mohs’ micrographic surgery, which results in reduced recurrence rates compared with other treatment options (Rowe et al, 1989; Mosterd et al, 2008). Radiation therapy provides an alternative treatment for some patients in whom surgery is not suitable or is not desired by the patient, or in the postoperative adjuvant setting if resection margins are positive and no further surgery is possible. The cosmetic result of radiation therapy can worsen over time, and this treatment method is therefore used predominantly in patients over 55 years of age (Miller, 2000; Telfer et al, 2008). Zagrodnik et al (2003) reviewed the efficacy of radiotherapy in 154 patients with BCC (181 tumours, many of which were at high risk) and found a mean overall 5-year recurrence rate of 15.8%. Recurrence rates varied with subtype, ranging from 8.2% for nodular BCCs to 27.7% for sclerosing (morphoeic/infiltrative) BCCs. The authors also noted development of additional skin tumours in 62% of patients following radiotherapy. A randomised trial of facial BCCs, with a diameter of 4 cm or less, showed a lower recurrence rate with surgery than with radiation therapy (0.7% vs 7.5%, P=0.003; Avril et al, 1997). Radiotherapy techniques used in this study included brachytherapy, a method which is uncommon in most irradiation centres owing to complexity of planning and radiation protection issues. The cure rate with radiation therapy, however, is still high, and it remains a valuable treatment option in selected patients.
Complex cases of BCC
In some cases of BCC, treatment is particularly challenging (Figure 1). These complex BCCs include locally advanced, recurrent and metastatic tumours and the evidence base for optimal management is not well established.

Example cases of complex BCCs. (A–C) Advanced facial lesions, (D) large ulcerated head lesion, (E) MRI of the patient in D demonstrating skull destruction and local invasion of the cerebellum, and (F) multiple trunk lesions.
Locally advanced BCC, in which tumours have become greatly enlarged, can result in significant tissue invasion and morbidity (Figure 1A–E). Surgical management of these tumours can be extensive and may result in considerable deformity, particularly in the cases of facial BCC, including pinnectomy or rhinectomy. In such extreme cases, the cosmetic implications of treatment and impact on quality of life can make surgery an unattractive option for the patient.
Recurrent BCC also poses a significant management problem and may require multiple operations (Figure 1F). However, in patients with inherited conditions resulting in multiple tumours (such as those with Gorlin’s syndrome), repeated surgical interventions may become untenable, and radiation therapy may be contraindicated because of the high risk of patients developing further BCCs (Leger et al, 2011).
Although metastatic BCC is rare, the prognosis for these patients is poor, with high morbidity and mortality (Ting et al, 2005). Large primary tumours or those with aggressive histological phenotypes (morphoeic, infiltrating and basosquamous) are the most likely to metastasise, with metastases commonly developing in the lymph nodes, skin, bones and lungs (Ting et al, 2005; Gropper et al, 2012). The 1-year overall survival probability after diagnosis of metastatic BCC was 75.7% (95% CI, 67.2–84.2%; McCusker et al, 2012). A review of case reports of metastatic BCC identified 101 published cases between 1981 and 2011. Among the 96 cases with information on treatment, more patients with distant metastases than with disease limited to the lymph nodes received chemotherapy (25% vs 9%, respectively), while fewer patients with distant metastases received surgery than those with lymph-node-only disease (52% vs 85%, respectively). These cases reveal that optimal treatment pathways for metastatic BCC are poorly defined and management approaches are inconsistent, generally relying on systemic chemotherapy (Weinstock and Still, 2011).
In summary, a number of treatment modalities are used in the management of complex BCCs, depending on the individual patient circumstances and tumour characteristics, and no evidence-based management guidelines have been published.
Factors influencing BCC complexity
Clinical factors to consider when assessing the complexity of BCC include the size, location and histological subtype of the tumour, its location on the body, and patient factors such as age and the presence of comorbidities. Aggressive subtypes of BCC, such as infiltrative or morphoeic tumours, and those with perineural or perivascular involvement, confer a higher risk of recurrence than nodular and superficial subtypes (Telfer et al, 2008). Large or giant tumours, classified as those with a diameter >5 cm (Eibenschutz et al, 2008), are often the result of delayed presentation and can result in extensive local invasion and disfigurement (Figure 1C–E). Giant BCCs located on the trunk are often treatable using surgery; however, facial tumours present a challenge, particularly those located in the high-risk ‘mask’ or ‘H-zone’ area (i.e., eyelids, nose, ear, chin, lips, mandible, temple and periorbital, preauricular and postauricular skin; Miller, 2000). Periorbital tumours most commonly involve the lower eyelid and can invade the orbit, leading to blindness in advanced cases. Tumours arising in the medial canthus are often deeply invasive, leading to perineural extension (Figure 1B). Similarly, tumours around the nose and ear can become highly invasive if not managed at an early stage (Figure 1A). The treatment option for high-risk facial tumours has typically been Mohs’ surgery; however, in advanced cases this can result in extreme deformity and risk of recurrence (Silverman et al, 1992). In this setting, surgery may not be deemed appropriate, either in terms of clinical prognosis or cosmetic outcome. Radiation therapy may be offered as an alternative treatment for complex cases of BCC, either with curative or palliative intent. However, this can have significant acute and late toxicity. Patients often have a view regarding the acceptability of surgery or radiation therapy and this may necessitate consideration of other treatment options.
Recurrent BCC poses a significant challenge in disease management, and cure rates are lower than those for primary disease (Rowe et al, 1989). Wide surgical margins are required to improve outcome, although recurrent facial tumours remain at high risk of further recurrence (Telfer et al, 2008). The number of tumours that BCC patients develop is another important factor to consider in disease management; genodermatoses including Gorlin’s syndrome, xeroderma pigmentosum, Bazex–Dupré–Christol syndrome and Rombo syndromes commonly result in multiple and recurrent BCC, and patients may require many operations as new lesions develop (Castori et al, 2012). The risk of BCC is also significantly increased in immunocompromised populations, such as solid organ transplant recipients (Rangwala and Tsai, 2011) and those receiving immunosuppressants for rheumatoid arthritis or inflammatory bowel disease (Chakravarty et al, 2005; Long et al, 2010). For example, renal transplant recipients have an estimated 10-fold increased incidence of BCC compared with immunocompetent individuals (Rangwala and Tsai, 2011) and are prone to developing multiple BCCs (Dreno, 2003). At some stage in the course of treatment, surgery may become an inappropriate option for patients with recurrent or multiple cases of BCC and the availability of novel treatment options would be invaluable.
In addition to disease phenotype, patient comorbidities and other clinical factors such as age and performance status may affect management decisions. For example, elderly or frail patients may not be suitable candidates for invasive surgery, and radiation therapy may not be favoured for young patients (Ting et al, 2005).
Patient-driven factors are also critical in guiding treatment of BCC. Those with large tumours that have often advanced through neglect may be fearful of seeking treatment or averse to invasive treatments (Gropper et al, 2012; Zoccali et al, 2012). Alternatively, negative experiences of previous treatments may make some individuals less receptive to repeat procedures. Patients may also have a strong opinion for other reasons on particular treatment options. Consideration of quality-of-life outcomes is also essential, and the level of deformity resulting from surgery, particularly for lesions affecting the face, may justify a decision not to operate. In such cases a diagnosis of advanced BCC may be made.
Defining advanced BCC
Providing a robust, objective definition of BCC cases of sufficient complexity to be classified as advanced is challenging, not only because of the heterogeneity of the disease, but because of variation in clinical practice and availability of treatment options. Patient opinion on treatment is also a defining factor in the diagnosis of advanced BCC, as a patient may be unwilling to undergo treatment that is technically feasible, but would be disfiguring or negatively affect their quality of life. Given the subjective nature of these factors, as well as the relatively small size of the patient group, there is currently a lack of clinical evidence on which to base a definition. However, such a definition is urgently required with the recent availability of novel treatments. After consideration by the UK-based group of multidisciplinary experts, the following definition of advanced BCC was proposed based on their review of the published literature and clinical experience.
‘Basal cell carcinoma of American Joint Committee on Cancer (AJCC) stage II or above (Edge et al, 2010), in which current treatment modalities are considered potentially contraindicated by clinical or patient-driven factors’ (Table 1).
The expert group also agreed that standardising the terminology used for cases of BCC included in this definition would provide clarity to the medical community for classification of this patient population. The group proposed the use of the term ‘advanced basal cell carcinoma’ for this purpose. Furthermore, with new treatment options becoming available, the patients’ population best suited to receiving them needs to be clearly defined.
New treatment options
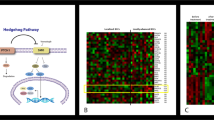
There are currently few treatment options for patients with advanced BCC. Research into new therapies has increasingly focused on targeted therapies, in particular inhibitors of the hedgehog signalling pathway, which has a key role in tumour growth and embryonic development (Lin and Matsui, 2012). Somatic mutations in this pathway are present in the vast majority of sporadic BCCs, as well as being present in the germline in Gorlin’s syndrome. Vismodegib, LDE225 and IPI926 are inhibitors of the hedgehog pathway signal transducer smoothened (Smo; Figure 2).

The hedgehog inhibitor pathway. (A) In the absence of the sonic hedgehog ligand, the patched receptor (PTCH) inhibits the activity of smoothened (Smo), allowing suppressor of fused (SUFU) to bind to and inactivate GLI transcription factors. (B) Binding of the sonic hedgehog ligand to PTCH allows activation of Smo, inhibiting the binding of SUFU to GLI. The GLI transcription factors are then able to enter the nucleus and modulate transcription of hedgehog pathway-associated genes. (C) Vismodegib and LDE225 inhibit Smo activation, preventing inhibition of SUFU binding and subsequent changes in hedgehog pathway-associated gene transcription.
The efficacy and tolerability of vismodegib in advanced BCC was first shown in a phase I study that included 33 patients with metastatic or locally advanced disease, with objective responses observed in 18 patients, stable disease in 11 patients and progressive disease in 4 patients. The most frequent grade 3 or greater adverse events were fatigue, hyponatraemia, weight loss and dyspnoea (Von Hoff et al, 2009). In the ensuing phase II trial, vismodegib demonstrated a 43% objective response rate in 63 patients with locally advanced BCC, with complete responses in 21% of patients, while of 33 patients with metastatic BCC, 30% achieved partial responses (Sekulic et al, 2012; Lear, 2012). Overall, tumour shrinkage was observed in more than 80% of the study patients. The most common adverse events reported were muscle spasms, alopecia, dysgeusia, weight loss and fatigue. A follow up of 18 months after the primary analysis showed that the efficacy and safety of vismodegib were maintained, with objective response rates of 49and 60%, and median durations of response of 14.7 and 20.3 months, in patients with metastatic and locally advanced BCC, respectively (Sekulic et al, 2013). A randomised phase II study in patients with Gorlin’s syndrome showed a significant reduction in the number of new surgically eligible BCCs and the size of existing tumours with vismodegib compared with placebo (Lear, 2012; Tang et al, 2012). A further open-label study is ongoing to assess the safety of vismodegib in patients with advanced or metastatic BCC (the STEVIE trial), which will recruit 1200 patients (Grob et al, 2013).
Vismodegib was approved by the US Food and Drug Administration in January 2012 and by the European Medicines Agency in July 2013 for the treatment of symptomatic metastatic BCC or locally advanced BCC in patients who are inappropriate for surgery or radiation therapy.
Clinical evaluation of oral LDE225 is ongoing, including a phase II study in patients with locally advanced or metastatic BCC and a randomised, double-blind, placebo-controlled study in Gorlin’s syndrome patients. In a phase I dose-escalation study in 76 patients with advanced solid tumours, oral LDE225 appeared to be generally well tolerated at dosages up to 800 mg once daily, with the most frequent adverse events being nausea, vomiting, dysgeusia, decreased appetite, myalgia, muscle spasms and fatigue. One complete response with histological clearance and four partial responses were observed in patients with advanced BCC, whereas two patients with advanced BCC had stable disease (Tawbi et al, 2011). A trial is also under way to assess the efficacy of LDE225 in patients with advanced BCC that has progressed during treatment with other hedgehog pathway inhibitors, such as vismodegib.
IPI926 has been assessed in a phase I dose-escalation study in 94 patients with advanced solid tumours, 39 of whom had a diagnosis of BCC (Jimeno et al, 2013). IPI926 appeared to be generally well tolerated; the most common adverse events were fatigue, nausea and alopecia, with the majority being grade 1–2 in severity. Preliminary assessment of efficacy in patients with BCC showed an objective response in eight patients with locally advanced disease, consisting of a complete response in two patients and a partial response in six patients.
Although hedgehog pathway inhibitors appear to be promising new therapies for advanced BCC, there are currently many clinical uncertainties regarding their efficacy and tolerability during long-term use in patients with advanced BCC, particularly in patients with genodermatoses such as Gorlin’s syndrome. In a post-hoc analysis of seven patients with Gorlin’s syndrome enroled in a randomised study of vismodegib (Tang et al, 2012), the rate of development of new surgically eligible BCC lesions following cessation of vismodegib treatment appeared to be significantly lower than in patients originally randomised to placebo (0.69 lesions vs 2.4 lesions per month), a finding that could warrant further investigation of the use of intermittent treatment in these patients. The role of hedgehog pathway inhibitors is still evolving; for example, their use in the neoadjuvant setting is under evaluation.
Conclusion
Complex cases of locally advanced, metastatic or recurrent BCC pose a significant management challenge and current treatment options are limited. With new therapies emerging, it is timely to raise awareness of the complexities of advanced BCC as an indication for these treatments. We propose here a definition of advanced BCC from the UK perspective: tumours of AJCC stage II or above in which current treatment modalities are considered potentially contraindicated by clinical or patient-driven factors.
Diagnosis of advanced BCC is very much dependent on the individual circumstances of each patient and treatment centre, as well as other clinical and patient factors that may preclude treatment or render available treatment options ineffective, including the size, location and histological subtype of the tumour, any underlying genetic or comorbid conditions, tumour multiplicity or recurrence, metastatic spread and patients’ fears or concerns about treatment.
Having established the diagnosis, management of advanced BCC should take place in the context of a specialist multidisciplinary team, involving dermatologists, plastic surgeons, oncologists, pathologists, radiologists and nurse specialists in order to determine appropriate treatment options. It is anticipated that the introduction of recently developed novel targeted treatments will help to fulfil the high unmet medical need of patients with advanced BCC.
References
Artis AHMM, Mosterd K, Essers BAB, Spoorenberg E, Sommer A, De Rooij MJM, van Pelt HPA, Quaedvlieg PJF, Krekels GAM, van Neer PAFA, Rijzewijk JJ, van Geest AJ, Steijlen PM, Nelemans PJ, Kelleners-Smeets NWJ (2013) Photodynamic therapy versus topical imiquimod versus topical fluorouracil for treatment of superficial basal-cell carcinoma: a single blind, non-inferiority, randomised controlled trial. Lancet Oncol 14: 647–654.
Avril MF, Auperin A, Margulis A, Gerbaulet A, Duvillard P, Benhamou E, Guillaume JC, Chalon R, Petit JY, Sancho-Garnier H, Prade M, Bouzy J, Chassagne D (1997) Basal cell carcinoma of the face: surgery or radiotherapy? Results of a randomized study. Br J Cancer 76: 100–106.
Baxter JM, Patel AN, Varma S (2012) Facial basal cell carcinoma. Br Med J 345: e5342.
Castori M, Morrone A, Kanitakis J, Grammatico P (2012) Genetic skin diseases predisposing to basal cell carcinoma. Eur J Dermatol 22: 299–309.
Chakravarty EF, Michaud K, Wolfe F (2005) Skin cancer, rheumatoid arthritis, and tumor necrosis factor inhibitors. J Rheumatol 32: 2130–2135.
Dummer R (2013) Treating basal-cell carcinoma in a real life setting. Lancet Oncol 14: 572–573.
Dreno B (2003) Skin cancers after transplantation. Nephrol Dial Transplant 18: 1502–1508.
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A (2010) AJCC Cancer Staging Manual ed 7. Springer: New York, pp 301–314.
Eibenschutz L, Marenda S, Buccini P, De Simone P, Ferrari A, Mariani G, Silipo V, Catricalà C (2008) Giant and large basal cell carcinoma treated with topical photodynamic therapy. Eur J Dermatol 18: 663–666.
Fernandes H, Fernandes N, Bhattacharya S, Chen W, Seth A, Hameed M, Mirani N, Lambert WC (2010) Molecular signatures linked with aggressive behavior in basal cell carcinoma: a report of 6 cases. Am J Dermatopathol 32: 550–556.
Grob JJ, Kunstfeld R, Dreno B, Jouary T, Mortier L, Basset-Sequin N, Ascierto PA, Hansson J, Mitchell L, Starnawski M, Hauschild A (2013) Vismodegib, a hedgehog pathway inhibitor (HPI), in advanced basal cell carcinoma (aBCC): STEVIE study interim analysis in 300 patients. J Clin Oncol 31 (Suppl): abstr 9036.
Gropper AB, Girouard SD, Hojman LP, Huang SJ, Qian X, Murphy GF, Vleugels RA (2012) Metastatic basal cell carcinoma of the posterior neck: case report and review of the literature. J Cutan Pathol 39: 526–534.
Jimeno A, Weiss GJ, Miller WH Jr, Gettinger S, Eigl BJC, Lynne A, Chang S, Dunbar J, Devens S, Faia K, Skliris G, Kutok J, Lewis KD, Tibes R, Sharfman WH, Ross RW, Rudin CM (2013) Phase I study of the hedgehog pathway inhibitor IPI-926 in adult patients with solid tumors. Clin Cancer Res 19: 2766–2774.
Lear JT (2012) Oral hedgehog-pathway inhibitors for basal-cell carcinoma. N Engl J Med 366: 2225–2226.
Leger M, Quintana A, Tzu J, Yee H, Kamino H, Sanchez M (2011) Nevoid basal cell carcinoma syndrome. Dermatol Online J 17: 23.
Lin TL, Matsui W (2012) Hedgehog pathway as a drug target: smoothened inhibitors in development. Onco Targets Ther 5: 47–58.
Lomas A, Leonardi-Bee J, Bath-Hextall F (2012) A systematic review of worldwide incidence of nonmelanoma skin cancer. Br J Dermatol 166: 1069–1080.
Long MD, Herfarth HH, Pipkin CA, Porter CQ, Sandler RS, Kappelman MD (2010) Increased risk for non-melanoma skin cancer in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol 8: 268–274.
McCusker ME, Hou J, Wang L, Yue H, Hauschild A (2012) Metastatic basal cell carcinoma: differences in survival by site of spread. J Clin Oncol 30 (suppl): abstr 8585.
Miller SJ (2000) The National Comprehensive Cancer Network (NCCN) guidelines of care for nonmelanoma skin cancers. Dermatol Surg 26: 289–292.
Mosterd K, Krekels GA, Nieman FH (2008) Surgical excision versus Mohs’ micrographic surgery for primary and recurrent basal-cell carcinoma of the face: a prospective randomised controlled trial with 5-years’ follow-up. Lancet Oncol 9: 1149–1156.
Rangwala S, Tsai KY (2011) Roles of the immune system in skin cancer. Br J Dermatol 165: 953–965.
Rowe DE, Carroll RJ, Day CL Jr (1989) Mohs surgery is the treatment of choice for recurrent (previously treated) basal cell carcinoma. J Dermatol Surg Oncol 15: 424–431.
Samarasinghe V, Madan V (2012) Nonmelanoma skin cancer. J Cutan Aesthet Surg 5: 3–10.
Scrivener Y, Grosshans E, Cribier B (2002) Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br J Dermatol 147: 41–47.
Sekulic A, Migden MR, Basset-Seguin N, Grabe C, Gesierich A, Lao CD, Miller C, Mortier L, Murrell DF, Hamid O, Quevedo F, Schadendorf D, Hou J, Yue H (2013) Long-term safety and efficacy of vismodegib in patients with advanced basal cell carcinoma (aBCC): 18-month update of the pivotal ERIVANCE BCC study. J Clin Oncol 31 (Suppl): abstr 9037.
Sekulic A, Migden MR, Oro AE, Dirix L, Lewis KD, Hainsworth JD, Solomon JA, Yoo S, Arron ST, Friedlander PA, Marmur E, Rudin CM, Chang AL, Low JA, Mackey HM, Yauch RL, Graham RA, Reddy JC, Hauschild A (2012) Efficacy and safety of vismodegib in advanced basal-cell carcinoma. N Engl J Med 366: 2171–2179.
Silverman MK, Kopf AW, Bart RS, Grin CM, Levenstein MS (1992) Recurrence rates of treated basal cell carcinomas. Part 3: surgical excision. J Dermatol Surg Oncol 18: 471–476.
Skvara H, Kalthoff F, Meingassner JG, Wolff-Winiski B, Aschauer H, Kelleher JF, Wu X, Pan S, Mickel L, Schuster C, Stary G, Jalili A, David OJ, Emotte C, Antunes AM, Rose K, Decker J, Carlson I, Gardner H, Stuetz A, Bertolino AP, Stingl G, De Rie MA (2011) Topical treatment of basal cell carcinomas in nevoid basal cell carcinoma syndrome with a smoothened inhibitor. J Invest Dermatol 131: 1735–1744.
Tang JY, Mackay-Wiggan JM, Aszterbaum M, Yauch RL, Lindgren J, Chang K, Coppola C, Chanana AM, Marji J, Bickers DR, Epstein EH Jr (2012) Inhibiting the hedgehog pathway in patients with the basal-cell nevus syndrome. N Engl J Med 366: 2180–2188.
Tawbi HA, Ahnert JR, Dummer R, Thomas AL, Granvil C, Shou Y, Dey J, Mita MM, Amakye DD, Mita AC (2011) Phase I study of LDE225 in advanced solid tumors: updated analysis of safety, preliminary efficacy, and pharmacokinetic-pharmacodynamic correlation. J Clin Oncol 29 (Suppl): abstr 3062.
Telfer NR, Colver GB, Morton CA (2008) Guidelines for the management of basal cell carcinoma. Br J Dermatol 159: 35–48.
Ting PT, Kasper R, Arlette JP (2005) Metastatic basal cell carcinoma: report of two cases and literature review. J Cutan Med Surg 9: 10–15.
Von Hoff DD, LoRusso PM, Rudin CM, Reddy JC, Yauch RL, Tibes R, Weiss GJ, Borad MJ, Hann CL, Brahmer JR, Mackey HM, Lum BL, Darbonne WC, Marsters JC Jr, de Sauvage FJ, Low JA (2009) Inhibition of the hedgehog pathway in advanced basal-cell carcinoma. N Engl J Med 361: 1164–1172.
Weinstock MA, Still JM (2011) Assessing current treatment options for patients with severe/advanced basal cell carcinoma. Semin Cutan Med Surg 30 (suppl 4): S10–S13.
Wong CS, Strange RC, Lear JT (2003) Basal cell carcinoma. Br Med J 327: 794–798.
Zagrodnik B, Kempf W, Seifert B, Müller B, Burg G, Urosevic M, Dummer R (2003) Superficial radiotherapy for patients with basal cell carcinoma: recurrence rates, histologic subtypes, and expression of p53 and Bcl-2. Cancer 98: 2708–2714.
Zoccali G, Pajand R, Papa P, Orsini G, Lomartire N, Giuliani M (2012) Giant basal cell carcinoma of the skin: literature review and personal experience. J Eur Acad Dermatol Venereol 26: 942–952.
Acknowledgements
We acknowledge Dr Qamar Ghafoor (New Queen Elizabeth Hospital, Birmingham, UK), Dr Irshad Zaki (Spire Parkway Hospital, Solihull, UK) and Dr Robert Herd (Western Infirmary, Glasgow, UK) for their review of this article. Succinct Medical Communications provided logistical support for the focus group meeting and editorial support for development of the manuscript, both of which were facilitated by a Grant from Roche Products Ltd. Complete editorial control was retained by the authors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
JTL, CC, KF, SV and CAH have sat on advisory boards and received honoraria from Roche Products Ltd. PD and GLR have no conflict of interest to declare.
PowerPoint slides
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article

Cite this article
Lear, J., Corner, C., Dziewulski, P. et al. Challenges and new horizons in the management of advanced basal cell carcinoma: a UK perspective. Br J Cancer 111, 1476–1481 (2014). https://doi.org/10.1038/bjc.2014.270
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2014.270
Keywords
This article is cited by
-
Assessment of various efficacy outcomes using ERIVANCE-like criteria in patients with locally advanced basal cell carcinoma receiving sonidegib: results from a preplanned sensitivity analysis
BMC Cancer (2021)
-
Effects of Sonidegib Following Dose Reduction and Treatment Interruption in Patients with Advanced Basal Cell Carcinoma During 42-Month BOLT Trial
Dermatology and Therapy (2021)
-
Sonidegib: Safety and Efficacy in Treatment of Advanced Basal Cell Carcinoma
Dermatology and Therapy (2020)
-
Advanced Squamous Cell Carcinoma: What’s New?
Current Dermatology Reports (2019)
-
Hedgehog Pathway Inhibition for the Treatment of Basal Cell Carcinoma
Targeted Oncology (2019)
