
Abstract
Background:
Inflammation contributes to the pathogenesis of colorectal cancer (CRC), and cytokine levels are altered during colorectal carcinogenesis.
Methods:
The serum levels of 13 cytokines and their relation to clinical and pathological parameters, and systemic inflammatory response (mGPS, CRP and neutrophil–lymphocyte ratio), were analysed from a prospective series of 148 CRC patients and 86 healthy age- and sex-matched controls.
Results:
CRC patients had higher serum platelet-derived growth factor, interleukin (IL)-6, IL-7, and IL-8 levels and lower monocyte chemotactic protein-1 (MCP-1) levels than the controls. A logistic regression model for discriminating the patients from the controls – including the five most predictive cytokines (high IL-8, high IL-6, low MCP-1, low IL-1ra, and low IP-10) – yielded an area under curve value of 0.890 in receiver operating characteristics analysis. Serum cytokines showed distinct correlation with other markers of systemic inflammatory response, and advanced CRCs were associated with higher levels of IL-8, IL-1ra, and IL-6. A metastasised disease was accompanied by an orientation towards Th2 cytokine milieu.
Conclusion:
CRC is associated with extensive alterations in serum cytokine environment, highlighting the importance of studying relative cytokine level alterations. Serum cytokine profile shows promise in separating CRC patients from healthy controls but its clinical value is yet to be confirmed.
Similar content being viewed by others

Main
Inflammation has a significant influence in the development of colorectal cancer (CRC) (Pages et al, 2010; Terzic et al, 2010). Patients with chronic inflammatory bowel disease, such as ulcerative colitis and Crohn’s disease, have an increased risk of developing CRC (Eaden et al, 2001; von Roon et al, 2007). Preventive effect of NSAIDs on the development of CRC has been shown in epidemiological studies (Rothwell et al, 2010) and also in a randomised placebo-controlled trial in HNPCC (Burn et al, 2011). Immune cells also contribute to the immunosurveillance, and high-grade peri- and intratumoral inflammatory cell infiltration is an independent indicator of an improved survival in CRC (Klintrup et al, 2005; Galon et al, 2006; Roxburgh et al, 2009). Moreover, systemic inflammatory markers like modified Glasgow prognostic score (mGPS) and blood neutrophil/lymphocyte ratio have established prognostic value in CRC (Roxburgh and McMillan, 2010).
Cytokines are key regulators of immune responses in cancer. They can modulate tumour growth and microenvironment by mediating interactions between cancer cells and infiltrating inflammatory cells. On the basis of their function, cytokines can be grouped into anti- or proinflammatory cytokines, chemokines, and growth factors. Moreover, the classification into Th1 and Th2 cytokines is of importance. In general, Th1-type cytokines, e.g., interleukin (IL)-12, IL-15, and interferon gamma (IFN-γ), contribute to cellular immune reactions considered essential for an effective response against tumour cells, whereas Th2-type cytokines, e.g., IL-4, IL-5, IL-10, and IL-13, may suppress the tumour-specific immune response (Ellyard et al, 2007; Cui and Florholmen, 2008).
The development of CRC is accompanied by alterations in cytokine production, which is thought to polarise from Th1 into Th2 along the colorectal adenoma–carcinoma sequence (Cui and Florholmen, 2008). Increased serum cytokine concentrations, e.g., elevated levels of IL-8 (Ueda et al, 1994), IL-6 (Knupfer and Preiss, 2010), and platelet-derived growth factor (PDGF) (Belizon et al, 2009) have been reported in CRC patients compared with healthy individuals, and certain cytokines and chemokines, such as IL-6 and VEGF, are considered to have prognostic value (Chung and Chang, 2003; De Vita et al, 2004; Knupfer and Preiss, 2010). One of the limitations of the previous studies examining serum inflammatory markers has been that they have focused on the levels of one or few cytokines at a time. However, relative alterations in cytokine levels can have substantial effects in the immune functions (Commins et al, 2010). Therefore, it is likely that an analysis of extensive set of cytokines would provide more accurate information on the tumour-related immunological responses, thus also bringing out the importance of individual cytokines on the immune response against CRC.
Tumour stage (TNM classification) is the most important prognostic factor in CRC (Puppa et al, 2010), and 5-year survival rate varies from 90% in stage I tumours to <10% in advanced stage IV tumours (O’Connell et al, 2004). To reduce mortality, it is essential to develop diagnostic tools for the early detection of cancer, which could be easily adapted to clinical use. At the moment, stool tests are neither very sensitive nor specific, and colonoscopy is a time-consuming and costly screening method (Sturgeon et al, 2008). Several serum markers have been assessed in the diagnostics of the disease, but none have been adapted to routine use so far (Sturgeon et al, 2008).
The aim of this study was to evaluate the pattern of alterations in the serum cytokine levels in CRC patients compared with controls. Accordingly, we analysed serum levels of 27 cytokines and chemokines from a series of 148 newly diagnosed CRC patients, and healthy controls matched for age and gender. An additional goal was to see whether the patterns of the serum cytokines in CRC could provide information of tumour stage.
Materials and methods
Patients and controls
This prospective study was introduced to all newly diagnosed CRC patients operated in Oulu University Hospital between April 2006 and January 2010 (n=344), of which a total of 148 patients were both eligible for the study and had signed informed consent to participate. Control serum samples were obtained from age- and sex-matched healthy voluntary blood donors (Finnish Red Cross, Oulu, Finland; n=36, age <65 years) and cataract surgery patients (Oulu University Hospital; n=50, age ⩾65 years). Patients and controls with earlier or simultaneously diagnosed other malignant diseases were excluded. Owing to the strict regulations in blood donation, other exclusion criteria for blood donor controls included, e.g., the absence of acute infections, trauma or operation during the preceding 4 months, chronic diseases like coronary artery disease, stroke or cancer, and organ transplantation. Study design was accepted by the Ethical Committee of Oulu University Hospital (58/2005, 184/2009).
Clinical details of patients and controls were acquired from the clinical records and by a questionnaire. Data on recurrences by the 24-month follow-up visit was collected in August 2012. Preoperative staging of CRC was done by whole-body CT-scan and the local staging of rectal cancer was done by MRI. Patients with T3 or T4 rectal tumours received preoperative radiotherapy or chemoradiotherapy (RT/CRT, n=32). To avoid confounding and to model the situation before the diagnosis of the disease, only those CRC patients who did not receive preoperative RT/CRT (n=116) were included in this study.
For the histopathological analysis, samples from the surgical specimens were fixed in 10% buffered formalin solution, embedded in paraffin, and 5-μm sections were stained with haematoxylin and eosin. TNM 6 (Sobin and Wittekind, 2002) was used in staging and WHO classification in grading (Hamilton et al, 2010). On an average, 15 lymph nodes were examined (median 12, interquartile range 8–19, range 0–62). Peritumoral inflammatory reaction was evaluated according to a two-tiered Klintrup–Mäkinen classification, where peritumoral inflammatory cell reaction was estimated to be low-grade when the peritumoral inflammatory cells formed no or patchy infiltrate that did not cause destruction of invading cancer cells at the invasive margin, and high-grade when inflammatory cells formed band-like or cuff-like peritumoral tumour-destructive infiltrate at the invasive margin (Klintrup et al, 2005).
Collection and analysis of serum samples
Blood samples from patients and controls were obtained in the morning after fasting for 12 h. The samples were centrifuged, and serum was stored at −70 °C until further analysis. Serum cytokine concentrations were analysed with Bio-Plex Pro Human pre-manufactured 27-Plex Cytokine Panel (Bio-Rad, Hercules, CA, USA). The pre-manufactured cytokine panel included 27 cytokines: IL-1β, IL-1ra, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8 (CXCL8), IL-9, IL-10, IL-12 (p70), IL-13, IL-15, IL-17, IFN-γ, tumour necrosis factor alpha, IFN-γ-induced protein 10 kDa (IP-10, CXCL10), monocyte chemotactic protein-1 (MCP-1, CCL2), macrophage inflammatory protein-1α (MIP-1α, CCL3), MIP-1β (CCL4), regulated upon activation, normal T-cell expressed, and secreted (CCL5), eotaxin (CCL11), granulocyte colony-stimulating factor, granulocyte-macrophage colony-stimulating factor, fibroblast growth factor basic, PDGF, subtype BB (PDGF-BB), and vascular endothelial growth factor A. The assay conditions were controlled, standardized and pre-optimized to ensure optimal repeatability and reproducibility of the assays according to the manufacturer’s instructions. The assay kits were all from the same lot, which allows better control of inter-assay variability. For the analyses, the samples were diluted in the appropriate sample matrix 1 : 2. The beads were incubated overnight with the samples. A minimum of 50 events (beads) were collected for each analyte, and the concentrations calculated from the standard curves on the basis of median fluorescence intensities. BioPlex Manager Software 4.1 (Bio-Rad) was utilised in calculating the concentrations.
Out of the 27 analytes, 13 cytokines (IL-1ra, IL-4, IL-6, IL-7, IL-8, IL-9, IL-12, IFN-γ, IP-10, MCP-1, MIP-1β, eotaxin, and PDGF-BB) with three (1.5%) or fewer values outside the assay working range were included in this study. The other 14 cytokines (IL-1β, IL-2, IL-5, IL-10, IL-13, IL-15, IL-17, fibroblast growth factor basic, granulocyte colony-stimulating factor, granulocyte-macrophage colony-stimulating factor, MIP-1α, regulated upon activation, normal T-cell expressed, and secreted, tumour necrosis factor, and VEGF) were excluded from this study because of having 20 (10%) or more of the values below or above the assay working range, which would not enable an examination as a continuous variable (Supplementary Table 1).
Statistical analyses
Normally distributed continuous variables are presented as mean (s.d.), whereas other continuous variables are presented as median (interquartile range). Statistical significances of the differences in serum cytokine levels between the different study groups and age, sex, stage, grade, inflammatory reaction, and BMI categories were analysed by Mann–Whitney U-test or Kruskal–Wallis test. Univariate correlations are presented as Pearson’s correlation coefficients after a logarithmic transformation of the variables with positive skewness. A logistic regression model was generated to evaluate the potential of serum cytokine profile in discriminating the CRC patients from the controls. For the model, the cytokine levels were logarithmically transformed to improve the goodness of fit. Backward stepwise approach was used to restrict the model to the five most predictive cytokines. The predictive power of the final model was evaluated by receiver operating characteristics analysis, and the goodness of fit of the model was tested with the Hosmer–Lemeshow statistic, where a nonsignificant probability value indicates good fit. The logistic regression model for the presence of nodal metastases was also constructed using the backward stepwise method. Multiple linear regression was used in stage-adjusted assessment of the associations between serum cytokines and patient age. The statistical analyses were carried out using statistical analysis software PASW Statistics 18 (IBM, Chicago, IL, USA). In all the tests, a two-tailed, exact P value <0.05 was considered statistically significant.
Results
Univariate analyses
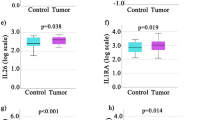
The characteristics of 116 CRC patients and 86 healthy controls are shown in Table 1, and their preoperative serum cytokine levels are summarised in Table 2. The levels of IL-6, IL-7, IL-8, and PDGF-BB were increased, and the levels of MCP-1 were decreased in patients compared with controls. Also Th1 cytokines IL-12 and IFN-γ showed a tendency towards increased values in CRC.
Age and gender
For seven of the thirteen cytokines (PDGF-BB, IL-1ra, IL-7, IL-8, IL-9, IFN-γ, and MIP-1β), the serum levels were higher in patients younger than 65 years compared with older patients (Supplementary Table 2). Only IP-10 levels were higher in patients aged 65 or older. The associations were mainly similar when age was studied as a continuous variable and correlation coefficients were calculated (Supplementary Table 3). Serum levels were similar in females and males (Supplementary TABLE 4), except for eotaxin, the levels of which were higher in male compared with female patients (P=0.017). There were no significant differences in cytokine levels between patients in different body mass index groups (data not shown).
Clinicopathological parameters
The patients with proximal tumour had higher serum IP-10 compared with patients having distal colon or rectal cancer (P=0.032; Supplementary Table 5). WHO grade 3 tumours yielded higher IL-1ra, IL-6, and IL-8 levels compared with grade 1 or 2 tumours (Table 3). Significant alterations of cytokine levels were also seen when assessing the effect of TNM stage (Table 4), as the levels of IL-1ra and especially IL-8 had an association with high-stage disease. Deeper local invasion (T) was associated with increased serum levels of IL-6 (P=0.015), IL-8 (P=9.28E−5), and MCP-1 (P=0.023; Supplementary Table 6), and the levels of IL-8 were also higher in the presence of lymph-node metastases (P=0.017; Supplementary Table 7). The patients with distant metastases (M1) had higher serum levels of IL-1ra (P=0.008), IL-4 (P=0.033), IL-6 (P=0.011), IL-7 (P=0.008), IL-8 (P=3.14E−5), MCP-1 (P=0.016), and PDGF-BB (P=0.010) compared with patients without metastases (M0; Supplementary Table 8). Serum cytokine levels were associated with other systemic inflammation markers. Patients with higher modified Glasgow prognostic score had higher serum levels of IL-1ra, IL-6, IL-7, IL-8, IL-9, IL-12, IFN-γ, IP-10, MCP-1, MIP-1β, and PDGF-BB (Supplementary Table 9). High blood neutrophil/lymphocyte ratio was associated with higher serum levels of IL-1ra, IL-6, IL-7, IL-8, and IL-12, MCP-1, and PDGF-BB, and high CRP was associated with higher levels of IL-1ra, IL-6, IL-7, IL-8, IL-12, and eotaxin (Supplementary Table 10). Klintrup–Mäkinen classification showed a statistical trend with the serum IL-8 levels (P=0.08, Mann–Whitney U-test). More detailed analyses of local inflammatory cell reaction were considered to be out of the scope of the current study.
Multivariate analyses
We generated a logistic regression model to evaluate the potential of serum cytokine profile in discriminating the CRC patients from the controls and to assess the mutual relationships of the differences observed in the univariate analyses. Certain cytokine values from three subjects were unreadable, and the model was based on 115 of 116 CRC patients and 84 of 86 controls.
The final model is presented in Table 5. It consists of the five most predictive cytokines chosen using the backward stepwise method. As in the univariate analyses, high IL-8 and IL-6, as well as low MCP-1, were associated with CRC. Interestingly, also low IL-1ra and IP-10 were associated with CRC, although these cytokines showed no difference between CRC patients and healthy controls in the univariate analyses. Hosmer-Lemeshow test for goodness-of-fit of the model indicated a good calibration (χ2=11.1, probability value=0.195). A receiver operating characteristics analysis for the model (Figure 1) yielded an area under curve of 0.890 (95% confidence interval, CI 0.845–0.934), which denotes an excellent discriminatory capability. Receiver operating characteristics curves were also obtained separately to all the cytokines included in the regression model, and the area under curves were the following: IL-1ra, 0.541 (95% CI 0.461–0.622); IL-6, 0.724 (95% CI 0.654–0.793); IL-8, 0.769 (95% CI 0.703–0.834); IP-10, 0.510 (95% CI 0.429–0.592); and MCP-1, 0.634 (95% CI 0.557–0.711).

A receiver operating characteristics curve for serum cytokine/chemokine profile in discriminating CRC patients from healthy controls. The profile achieved an excellent discriminatory capability. Several probability cutoff values were tested, and the sensitivities and specificities were calculated: cutoff 0.349 (sensitivity 0.930, specificity 0.607), cut-off 0.500 (sensitivity 0.826, specificity 0.738), cut-off 0.545 (sensitivity 0.809, specificity 0.821), and cut-off 0.690 (sensitivity 0.687, specificity 0.952). Abbreviations: AUC=area under curve; CI=confidence interval.
Next, we generated a logistic regression model for discriminating patients with nodal metastases from patients without nodal metastases. Using the backward stepwise method, the model was restricted to the four most predictive cytokines because of a smaller number of positive cases than in the model used to separate patients from controls. In this model, low IFN-γ (OR 0.09, 95% CI 0.005–1.65, P=0.105) and IP-10 (OR 0.11, 95% CI 0.015–0.85, P=0.034) and high IL-8 (OR 9.4, 95% CI 1.5–58.3, P=0.016) and IL-1ra (OR 8.3, 95% CI 0.8–84.5, P=0.074) were associated with lymph-node metastases. A small amount of M1 cases (n=18) did not enable a construction of a sensible logistic regression model for the presence of distant metastases.
Regression models were also used to adjust the differences observed in univariate analyses for potential confounding factors. Several potential confounding factors were tested, and in our material, adjusting for BMI, sex, and the age of the patients did not influence the results of the univariate analyses (data not shown). Tumour grade correlated with stage, but small numbers of grade 3 (n=14) tumours did not allow us to construct a regression model to confirm confounding by that. Most of the negative correlations between serum cytokine levels and patient age were found to be a result of younger patients being more likely to have a metastasised disease, as age correlated only positively with IP-10 and negatively with PDGF-BB when the correlations were adjusted for stage using multiple linear regression (Supplementary Table 11).
Recurrence analysis
Owing to the short follow-up at the moment, we were not able to perform a complete 60-month survival analysis. Instead, we carried out a 24-month recurrence analysis, which included 79 (68.1%) of 116 patients. Of the 116 patients, 22 (19.0%) were excluded because they underwent a palliative operation, and 15 (12.9%) were excluded because they did not have the 24-month follow-up data available. Recurrences were observed in 17 patients (21.5%). None of the studied cytokine markers had a statistically significant association with recurrences (Supplementary Table 12). However, a longer follow-up is needed, and also neutrophil/lymphocyte ratio, modified Glasgow prognostic score, and Klintrup–Mäkinen classification for local general inflammatory infiltrate (Supplementary Table 13) lacked a significant association with recurrences in this limited follow-up despite having an established prognostic value.
Discussion
Cytokines and chemokines form a complex network of regulatory proteins, and often several cytokines are required to synergize to bring about an optimal effect (Commins et al, 2010). To our knowledge, this is so far the most extensive study on serum cytokine and chemokine alterations in CRC. The method used in this study offers an opportunity to study relative changes of cytokine levels, allowing analysing the shifts in the immune balance occurring in patients with CRC. In this study, we generated a logistic regression model that showed an excellent ability to discriminate patients from the controls, and yielded information that may prove useful for the development of clinical applications for screening, diagnosis, staging, and even for the follow-up of CRC.
In univariate analyses, CRC patients had increased serum levels of PDGF-BB, IL-6, IL-7, and IL-8, and decreased levels of MCP-1. The increases in serum PDGF-BB, IL-6, and IL-8 levels in CRC have been reported earlier (Ueda et al, 1994; Belizon et al, 2009; Knupfer and Preiss, 2010). Increase of IL-7 levels and decrease of MCP-1 levels in CRC represent novel findings of this study. Previously, IL-7 levels have been reported to be increased in early-stage prostate cancer as compared with benign prostate hyperplasia (Mengus et al, 2011), and decreased MCP-1 levels have been described in gastric cancer (Tonouchi et al, 2002). Of these five cytokines, PDGF-BB has a prominent role in cell proliferation, cell migration, and angiogenesis (Hellberg et al, 2010). IL-6 is a pleiotropic cytokine with a variety of functions, including interaction between acute and chronic inflammation, inducing B-lymphocyte responses, and acute-phase functions like pyrogenic effect (Naugler and Karin, 2008), whereas IL-7 is considered to be an important haematopoietic cytokine having a role in the generation of both T and B lymphocytes (Mackall et al, 2011). The primary function of IL-8 is to recruit neutrophils during acute inflammation, while MCP-1 is chemoattractant for monocytes (Wang et al, 2009).
The knowledge of the cancer-specific functions of cytokines and chemokines is still limited. In CRC, IL-6 has been reported to increase the proliferation and invasiveness of cancer cells and promote tumour angiogenesis (Knupfer and Preiss, 2010). Also IL-8 has been suggested to have a multifunctional role in CRC progression, which possibly involves enhancing the survival of cancer cells and regulating adhesion and invasion, in addition to recruiting neutrophils (Rubie et al, 2007; Waugh and Wilson, 2008). These suggested functions correspond to our observation of both IL-6 and IL-8 having an association with a metastasised disease. Higher levels of IL-7 in CRC seen in this study is an interesting finding, as IL-7 enhances the responses to immunisation, especially to weak or low-affinity antigens common for cancer (Melchionda et al, 2005; Capitini et al, 2009). Monocyte chemoattractant MCP-1 has been shown to be overexpressed in several solid tumours, and it is thought to be responsible for acquiring tumour-associated macrophages, which in most tumours present with an anti-inflammatory phenotype (Mantovani et al, 2008).
The role of tumour-associated macrophages in CRC is controversial. Most studies have indicated that peritumoral macrophages have a favourable effect on CRC prognosis, suggesting their polarisation towards M1 phenotype (Klintrup et al, 2005; Erreni et al, 2011). On the contrary, intratumoral macrophages in CRC have been shown to be correlated with invasion and lymph-node metastases, and in general with more aggressive behaviour, which allows a suggestion that intratumoral macrophages in CRC are polarised towards M2 phenotype (Pancione et al, 2009; Kang et al, 2010). In colon, increased MCP-1 expression has been observed in colorectal adenomas in relation to normal epithelium, and it has also been related to an increased tumour-associated macrophage accumulation within tumour tissue and to an advancing stage (Tanaka et al, 2006; Bailey et al, 2007). It should be noted, however, that the increase of MCP-1 in colorectal adenoma and CRC tissue has been observed in relation to the non-neoplastic mucosa of CRC or adenoma patients, not to the normal mucosa obtained from healthy controls. In our study, serum MCP-1 concentrations are increased by advancing stage, yet in all CRC patients, we detected lower mean serum concentrations of MCP-1 than in controls. In an earlier report examining serum MCP-1 levels, 14% of CRC patients had lower MCP-1 value than the minimum value of any of the healthy volunteers, although no statistically significant difference between these two study groups was observed (Tonouchi et al, 2004).
According to our results, the absolute levels of cytokines generally increase in CRC, but there are also alterations in the relative cytokine levels indicating a shift in the balance of the immune system. Our logistic regression model revealed a relative decrease in the levels of serum IL-1ra and IP-10 in CRC, besides the increases in serum IL-6 and IL-8 and the decrease in serum MCP-1, which were also seen in univariate analyses. In this model, decreased IL-1ra/IL-6 ratio in CRC might indicate a decreased systemic anti-inflammatory response against the tumour. Similarly, increased levels of neutrophil chemoattractant IL-8 relative to monocyte chemoattractants IP-10 and MCP-1 might depict an orientation towards a granulocyte response, although mononuclear cells are considered to be the main contributors to restricting cancer growth (Klintrup et al, 2005). However, the actions of most cytokines and chemokines are pleiotropic (Commins et al, 2010), and, e.g., IP-10, a chemokine secreted by several cell types in response to IFN-γ, is antiangiogenic besides possessing a leucocyte chemoattractant function (Luster and Leder, 1993; Strieter et al, 1995).
Our findings corroborate earlier observations that serum cytokine levels in CRC have only minor association with age and gender (Kaminska et al, 2005; Sharma et al, 2010). In our study, the levels of PDGF-BB, IL-1ra, IL-7, IL-8, IL-9, IFN-γ, and MIP-1β were slightly higher and IP-10 levels were lower in younger patients in univariate analysis, but younger patients more often presented with a metastatic disease. After adjusting for disease stage, the only significant correlations between serum cytokines and patient age were lower IP-10 and higher PDGF levels in the younger patients. The only difference we observed between males and females was higher eotaxin levels in the male patients. Biology of this difference is unknown at present, but it could offer a new aspect for studying gender-related differences of CRC.
Proximal and distal CRCs are different regarding their pathogenesis and many clinical and pathological characteristics, as well as in their behaviour. Proximal CRC is more frequent in female patients, presents more often with MSI and increased numbers of tumour-infiltrating lymphocytes, and also a greater proportion of Lynch syndrome-associated CRCs occur in the proximal colon (Jenkins et al, 2007). On this basis, we expected that the differences of the proximal and distal CRCs would be reflected in the cytokine profile, but the only difference we found was slightly elevated levels of IP-10 in proximal colon cancer compared with distal colon and rectal cancer.
The levels of IL-1ra, IL-6, and IL-8 were found to be significantly higher in patients with poorly differentiated tumours than in those with well- or moderately-differentiated tumours. However, the levels of these three cytokines were also among those most dependent on the tumour stage, which could confound the result. Nevertheless, similar association of serum IL-6 and IL-8 and poor differentiation has been reported earlier in CRC (Kaminska et al, 2005), and poorly differentiated and undifferentiated CRCs have been demonstrated to have up to 20-fold activity in IL-6 gene (Brozek et al, 2005), suggesting that the increased serum levels observed could be related to an increased IL-6 production by the poorly differentiated cancer cells.
The alterations in the levels of major Th1 (IL-12, IFN-γ) and Th2 (IL-4) cytokines was one of our interests, as a shift towards Th2 cytokine response has been proposed to occur in the development of CRC (Pellegrini et al, 1996; Cui and Florholmen, 2008). We could not demonstrate a clear polarisation of the systemic cytokine levels towards Th2 in CRC, as our CRC patients showed a trend for increased levels of both Th2 (IL-4) and Th1 (IL-12 and IFN-γ) cytokines. Instead, a Th2-oriented cytokine milieu – evidenced by an increase in IL-4 in the absence of significant alterations in IL-12 and IFN-γ – was associated with a metastatic disease. Thus, rather than being characteristic to CRC, shift of Th1/Th2 balance towards Th2 seems to be related to the progression of cancer. In tissue level, local Th1-type immune response typically shows high densities of tumour-infiltrating lymphocytes and is associated with better survival (Ropponen et al, 1997; Naito et al, 1998). An association of Th1 response with prognostically significant antitumour activity is further supported by our regression model, where high IFN-γ associated with the absence of nodal metastases. Therefore, we believe that assessment of Th1/Th2 balance may help to identify CRC patients with a shift of cytokine levels towards Th2, resulting in an ineffective immune response and unfavourable prognosis. Such patients could be reasonable subjects for more intensive or tailored treatment, including immunomodulatory therapy (Pages et al, 2010). However, at this point, the follow-up time in our prospective material is not long enough, and it remains to be seen, whether serum cytokine profile could add prognostic information to other systemic inflammation-based markers like neutrophil/lymphocyte ratio or modified Glasgow prognostic score (Roxburgh and McMillan, 2010).
Majority of CRC deaths could be prevented by sensitive screening methods. At the moment, stool tests are neither very sensitive nor specific, and colonoscopy is a time-consuming and costly method (Sturgeon et al, 2008). Carcinoembryonic antigen is a widely used serum biomarker for CRC follow-up, but its sensitivity and specificity in the detection of CRC is low (Duffy, 2001; Sturgeon et al, 2008). As cytokines and chemokines are involved in most systemic and local inflammatory diseases, it is unlikely that determination of any single cytokine could be used as a diagnostic or a follow-up marker for CRC. Instead, by examining changes in multiple cytokines, it may be possible to detect more specific ‘cytokine footprints’ for different inflammatory and neoplastic diseases. For example, a promising result based on a multiplexed cytokine immunoassay in identifying lung cancer has been reported recently (Lee et al, 2010). In our study, measurements covering several essential cytokines enabled us to generate a logistic regression model – a serum cytokine profile – which achieved an excellent accuracy in discriminating CRC patients from healthy controls with an area under curve of 0.890 in the receiver operating characteristics analysis. This observation supports the potential of cytokine determinations as a screening or diagnostic tool. Still, our study has also limitations, as we did not have comparison groups of patients with inflammatory or infectious diseases and the logistic regression model was specifically fitted to our material. Therefore, our results and approach need to be confirmed by subsequent studies with independent study populations, and in studies including subjects with inflammatory conditions and gastrointestinal symptoms.
In conclusion, CRC is characterised by broad and complex alterations in serum cytokine and chemokine levels, including increased PDGF-BB, IL-6, IL-7, and IL-8 and decreased MCP-1. Our study highlights the benefits of analysing the serum cytokine levels as a group to observe relative expression level changes. Future studies are needed to compare the alterations between serum cytokine levels and individual inflammatory cell response to reveal immune reaction patterns in CRC, as well as to evaluate the specificity of the alterations of the cytokine profile in CRC in relation to other inflammatory disorders and neoplasms.
Change history
26 October 2012
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Bailey C, Negus R, Morris A, Ziprin P, Goldin R, Allavena P, Peck D, Darzi A (2007) Chemokine expression is associated with the accumulation of tumour associated macrophages (TAMs) and progression in human colorectal cancer. Clin Exp Metastasis 24: 121–130
Belizon A, Balik E, Horst PK, Shantha Kumara HM, Nasar A, Whelan RL (2009) Platelet-derived growth factor (subtype BB) is elevated in patients with colorectal carcinoma. Dis Colon Rectum 52: 1166–1171
Brozek W, Bises G, Girsch T, Cross HS, Kaiser HE, Peterlik M (2005) Differentiation-dependent expression and mitogenic action of interleukin-6 in human colon carcinoma cells: relevance for tumour progression. Eur J Cancer 41: 2347–2354
Burn J, Gerdes AM, Macrae F, Mecklin JP, Moeslein G, Olschwang S, Eccles D, Evans DG, Maher ER, Bertario L, Bisgaard ML, Dunlop MG, Ho JW, Hodgson SV, Lindblom A, Lubinski J, Morrison PJ, Murday V, Ramesar R, Side L, Scott RJ, Thomas HJ, Vasen HF, Barker G, Crawford G, Elliott F, Movahedi M, Pylvanainen K, Wijnen JT, Fodde R, Lynch HT, Mathers JC, Bishop DT on behalf of the CAPP2 Investigators (2011) Long-term effect of aspirin on cancer risk in carriers of hereditary colorectal cancer: an analysis from the CAPP2 randomised controlled trial. Lancet 378: 2081–2087
Capitini CM, Chisti AA, Mackall CL (2009) Modulating T-cell homeostasis with IL-7: preclinical and clinical studies. J Intern Med 266: 141–153
Chung YC, Chang YF (2003) Serum interleukin-6 levels reflect the disease status of colorectal cancer. J Surg Oncol 83: 222–226
Commins SP, Borish L, Steinke JW (2010) Immunologic messenger molecules: cytokines, interferons, and chemokines. J Allergy Clin Immunol 125: S53–S72
Cui G, Florholmen J (2008) Polarization of cytokine profile from Th1 into Th2 along colorectal adenoma-carcinoma sequence: implications for the biotherapeutic target? Inflamm Allergy Drug Targets 7: 94–97
De Vita F, Orditura M, Lieto E, Infusino S, Morgillo F, Martinelli E, Castellano P, Romano C, Ciardiello F, Catalano G, Pignatelli C, Galizia G (2004) Elevated perioperative serum vascular endothelial growth factor levels in patients with colon carcinoma. Cancer 100: 270–278
Duffy MJ (2001) Carcinoembryonic antigen as a marker for colorectal cancer: is it clinically useful? Clin Chem 47: 624–630
Eaden JA, Abrams KR, Mayberry JF (2001) The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut 48: 526–535
Ellyard JI, Simson L, Parish CR (2007) Th2-mediated anti-tumour immunity: friend or foe? Tissue Antigens 70: 1–11
Erreni M, Mantovani A, Allavena P (2011) Tumor-associated macrophages (TAM) and inflammation in colorectal cancer. Cancer Microenviron 4: 141–154
Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-Pages C, Tosolini M, Camus M, Berger A, Wind P, Zinzindohoue F, Bruneval P, Cugnenc PH, Trajanoski Z, Fridman WH, Pages F (2006) Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science 313: 1960–1964
Hamilton SR, Bosman FT, Boffetta P, Ilyas M, Morreau H, Nakamura S-I, Quirke P, Riboli E, Sobin LH (2010) Carcinoma of the colon and rectum. In World Health Organization classification of tumours of the digestive system. Pathology and genetics of tumours of the digestive system, Bosman FT, Carneiro F, Hruban RH, Theise NDSR, (eds) pp 134–146. IARC Press: Lyon
Hellberg C, Ostman A, Heldin CH (2010) PDGF and vessel maturation. Recent Results Cancer Res 180: 103–114
Jenkins MA, Hayashi S, O'Shea AM, Burgart LJ, Smyrk TC, Shimizu D, Waring PM, Ruszkiewicz AR, Pollett AF, Redston M, Barker MA, Baron JA, Casey GR, Dowty JG, Giles GG, Limburg P, Newcomb P, Young JP, Walsh MD, Thibodeau SN, Lindor NM, Lemarchand L, Gallinger S, Haile RW, Potter JD, Hopper JL, Jass JR Colon Cancer Family Registry (2007) Pathology features in Bethesda guidelines predict colorectal cancer microsatellite instability: a population-based study. Gastroenterology 133: 48–56
Kaminska J, Nowacki MP, Kowalska M, Rysinska A, Chwalinski M, Fuksiewicz M, Michalski W, Chechlinska M (2005) Clinical significance of serum cytokine measurements in untreated colorectal cancer patients: soluble tumor necrosis factor receptor type I--an independent prognostic factor. Tumour Biol 26: 186–194
Kang JC, Chen JS, Lee CH, Chang JJ, Shieh YS (2010) Intratumoral macrophage counts correlate with tumor progression in colorectal cancer. J Surg Oncol 102: 242–248
Klintrup K, Mäkinen JM, Kauppila S, Väre PO, Melkko J, Tuominen H, Tuppurainen K, Mäkelä J, Karttunen TJ, Mäkinen MJ (2005) Inflammation and prognosis in colorectal cancer. Eur J Cancer 41: 2645–2654
Knupfer H, Preiss R (2010) Serum interleukin-6 levels in colorectal cancer patients--a summary of published results. Int J Colorectal Dis 25: 135–140
Lee G, Lee JM, Gardner BK, Walser TC, Krysan K, Pak PS, Mao J, Hazra S, Dubinett SM (2010) Blood-based biomarker profiles for detecting lung cancer. J Thorac Oncol 5 (Suppl 3): S220–S221
Luster AD, Leder P (1993) IP-10, a -C-X-C- chemokine, elicits a potent thymus-dependent antitumor response in vivo. J Exp Med 178: 1057–1065
Mackall CL, Fry TJ, Gress RE (2011) Harnessing the biology of IL-7 for therapeutic application. Nat Rev Immunol 11: 330–342
Mantovani A, Allavena P, Sica A, Balkwill F (2008) Cancer-related inflammation. Nature 454: 436–444
Melchionda F, Fry TJ, Milliron MJ, McKirdy MA, Tagaya Y, Mackall CL (2005) Adjuvant IL-7 or IL-15 overcomes immunodominance and improves survival of the CD8+ memory cell pool. J Clin Invest 115: 1177–1187
Mengus C, Le Magnen C, Trella E, Yousef K, Bubendorf L, Provenzano M, Bachmann A, Heberer M, Spagnoli GC, Wyler S (2011) Elevated levels of circulating IL-7 and IL-15 in patients with early stage prostate cancer. J Transl Med 9: 162
Naito Y, Saito K, Shiiba K, Ohuchi A, Saigenji K, Nagura H, Ohtani H (1998) CD8+ T cells infiltrated within cancer cell nests as a prognostic factor in human colorectal cancer. Cancer Res 58: 3491–3494
Naugler WE, Karin M (2008) The wolf in sheep's clothing: the role of interleukin-6 in immunity, inflammation and cancer. Trends Mol Med 14: 109–119
O’Connell JB, Maggard MA, Ko CY (2004) Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J Natl Cancer Inst 96: 1420–1425
Pages F, Galon J, Dieu-Nosjean MC, Tartour E, Sautes-Fridman C, Fridman WH (2010) Immune infiltration in human tumors: a prognostic factor that should not be ignored. Oncogene 29: 1093–1102
Pancione M, Forte N, Sabatino L, Tomaselli E, Parente D, Febbraro A, Colantuoni V (2009) Reduced beta-catenin and peroxisome proliferator-activated receptor-gamma expression levels are associated with colorectal cancer metastatic progression: correlation with tumor-associated macrophages, cyclooxygenase 2, and patient outcome. Hum Pathol 40: 714–725
Pellegrini P, Berghella AM, Del Beato T, Cicia S, Adorno D, Casciani CU (1996) Disregulation in TH1 and TH2 subsets of CD4+ T cells in peripheral blood of colorectal cancer patients and involvement in cancer establishment and progression. Cancer Immunol Immunother 42: 1–8
Puppa G, Sonzogni A, Colombari R, Pelosi G (2010) TNM staging system of colorectal carcinoma: a critical appraisal of challenging issues. Arch Pathol Lab Med 134: 837–852
Ropponen KM, Eskelinen MJ, Lipponen PK, Alhava E, Kosma VM (1997) Prognostic value of tumour-infiltrating lymphocytes (TILs) in colorectal cancer. J Pathol 182: 318–324
Rothwell PM, Wilson M, Elwin CE, Norrving B, Algra A, Warlow CP, Meade TW (2010) Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet 376: 1741–1750
Roxburgh CS, McMillan DC (2010) Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol 6: 149–163
Roxburgh CS, Salmond JM, Horgan PG, Oien KA, McMillan DC (2009) Tumour inflammatory infiltrate predicts survival following curative resection for node-negative colorectal cancer. Eur J Cancer 45: 2138–2145
Rubie C, Frick VO, Pfeil S, Wagner M, Kollmar O, Kopp B, Graber S, Rau BM, Schilling MK (2007) Correlation of IL-8 with induction, progression and metastatic potential of colorectal cancer. World J Gastroenterol 13: 4996–5002
Sharma A, Greenman J, Walker LG, Monson JR (2010) Differences in cytokine levels due to gender in colorectal cancer patients. Cytokine 50: 91–93
Sobin LH, Wittekind C (eds) (2002) TNM Classification Of Malignant Tumours. Wiley-Liss: New York
Strieter RM, Kunkel SL, Arenberg DA, Burdick MD, Polverini PJ (1995) Interferon gamma-inducible protein 10 (IP-10), a member of the C-X-C chemokine family, is an inhibitor of angiogenesis. Biochem Biophys Res Commun 210: 51–57
Sturgeon CM, Duffy MJ, Stenman UH, Lilja H, Brunner N, Chan DW, Babaian R, Bast RC, Dowell B, Esteva FJ, Haglund C, Harbeck N, Hayes DF, Holten-Andersen M, Klee GG, Lamerz R, Looijenga LH, Molina R, Nielsen HJ, Rittenhouse H, Semjonow A, Shih I, Sibley P, Soletormos G, Stephan C, Sokoll L, Hoffman BR, Diamandis EP National Academy of Clinical Biochemistry (2008) National Academy of Clinical Biochemistry laboratory medicine practice guidelines for use of tumor markers in testicular, prostate, colorectal, breast, and ovarian cancers. Clin Chem 54: e11–e79
Tanaka S, Tatsuguchi A, Futagami S, Gudis K, Wada K, Seo T, Mitsui K, Yonezawa M, Nagata K, Fujimori S, Tsukui T, Kishida T, Sakamoto C (2006) Monocyte chemoattractant protein 1 and macrophage cyclooxygenase 2 expression in colonic adenoma. Gut 55: 54–61
Terzic J, Grivennikov S, Karin E, Karin M (2010) Inflammation and colon cancer. Gastroenterology 138: 2101.e5–2114.e5
Tonouchi H, Miki C, Ohmori Y, Kobayashi M, Mohri Y, Tanaka K, Konishi N, Kusunoki M (2004) Serum monocyte chemoattractant protein-1 in patients with postoperative infectious complications from gastrointestinal surgery for cancer. World J Surg 28: 130–136
Tonouchi H, Miki C, Tanaka K, Kusunoki M (2002) Profile of monocyte chemoattractant protein-1 circulating levels in gastric cancer patients. Scand J Gastroenterol 37: 830–833
Ueda T, Shimada E, Urakawa T (1994) Serum levels of cytokines in patients with colorectal cancer: possible involvement of interleukin-6 and interleukin-8 in hematogenous metastasis. J Gastroenterol 29: 423–429
von Roon AC, Reese G, Teare J, Constantinides V, Darzi AW, Tekkis PP (2007) The risk of cancer in patients with Crohn's disease. Dis Colon Rectum 50: 839–855
Wang D, Dubois RN, Richmond A (2009) The role of chemokines in intestinal inflammation and cancer. Curr Opin Pharmacol 9: 688–696
Waugh DJ, Wilson C (2008) The interleukin-8 pathway in cancer. Clin Cancer Res 14: 6735–6741
Acknowledgements
We thank Ms Riitta Vuento, Ms Marja Tolppanen, Ms Meeri Kröger, Ms Helena Moilanen, and Ms Aila Vehkaperä for their help in this study, and Dr Heikki Tokola, MD, for his help in the collection of the material. This work has been supported by grants from the Academy of Finland, Emil Aaltonen Foundation, Finnish Cancer Society, Finnish Medical Foundation, and Northern Finland Cancer Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Supplementary Information accompanies the paper on British Journal of Cancer website
Supplementary information
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Kantola, T., Klintrup, K., Väyrynen, J. et al. Stage-dependent alterations of the serum cytokine pattern in colorectal carcinoma. Br J Cancer 107, 1729–1736 (2012). https://doi.org/10.1038/bjc.2012.456
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2012.456
Keywords
This article is cited by
-
Prognostic Significance of Sarcopenia and Systemic Inflammatory Markers in Biliary Tract Cancer: A Retrospective Cohort Study
Journal of Gastrointestinal Cancer (2024)
-
Integrated circulating tumour DNA and cytokine analysis for therapy monitoring of ALK-rearranged lung adenocarcinoma
British Journal of Cancer (2023)
-
Association of ABCA1 R219K polymorphism and telomere length in a Chinese rural population: possible linking to systemic inflammation
Journal of Genetics (2023)
-
Neutrophil–lymphocyte ratio (NLR), platelet–lymphocyte ratio (PLR) and lymphocyte–monocyte ratio (LMR) in predicting systemic inflammatory response syndrome (SIRS) and sepsis after percutaneous nephrolithotomy (PNL)
Urolithiasis (2022)
-
Association of blood biomarkers and autoimmunity with immune related adverse events in patients with cancer treated with immune checkpoint inhibitors
Scientific Reports (2021)
