
Abstract
Aim:
Co-administration of diltiazem can reduce the dosage of cyclosporine (CsA) in patients with renal transplantation. In this study, we investigated how diltiazem altered the relationship between MDR1 genetic polymorphisms and CsA concentration in Chinese patients with renal transplantation.
Methods:
A total of 126 renal transplant patients were enrolled. All the patients received CsA (2–4 mg·kg−1·d−1), and diltiazem (90 mg/d) was co-administered to 76 patients. MDR1-C1236T, G2677T/A, and C3435T polymorphisms were genotyped. The whole blood concentration was measured using the FPIA method, and the adjusted trough concentrations were compared among the groups with different genotypes.
Results:
In all patients, MDR1-C1236T did not influence the adjusted CsA trough concentration. With regard to MDR1-3435, the adjusted CsA trough concentration was significantly higher in TT carriers than in CC and CT carriers when diltiazam was co-administered (58.83±13.95 versus 46.14±7.55 and 45.18±12.35 ng/mL per mg/kg, P=0.011), and the differences were not observed in patients without diltiazam co-administered. With regard to MDR1-2677, the adjusted CsA trough concentration was significantly higher in TT carriers than in GG and GT carriers when diltiazam was co-administered (61.31±12.93 versus 52.25±7.83 and 39.70±7.26 ng/mL per mg/kg, P=0.0001). The differences were also observed in patients without diltiazam co-administered (43.27±5.95 versus 35.22±7.55 and 29.54±5.35 ng/mL per mg/kg, P=0.001). The adjusted CsA trough blood concentration was significantly higher in haplotype T-T-T and haplotype T-T-C carriers than in non-carriers, regardless of diltiazem co-administered.
Conclusion:
MDR1 variants influence the adjusted CsA trough concentration in Chinese patients with renal transplant, and the influence more prominent when diltiazem is co-administered.
Similar content being viewed by others


Introduction
Cyclosporine (CsA), a calcineurin inhibitor, is widely used to prevent acute rejection after solid organ transplantation1. However, cyclosporine has low oral bioavailability, a narrow therapeutic index and shows marked interindividual differences in pharmacokinetics2 . The ATP-driven efflux pump, P-glycoprotein (P-gp), has been identified as an absorptive barrier to orally administered CsA. Therefore, P-gp might play a role in the disposition of CsA3.
The multidrug resistance gene (MDR1), encoding P-gp, is expressed at high levels in the adrenal glands and kidneys, at intermediate levels in the lung, liver, lower jejunum, colon and rectum, and at low levels in many other tissues4. As a transporter, P-gp plays a significant role in drug disposition, ie, absorption, distribution, and excretion, and might also be involved in the secretion of steroids5. A total of 50 single nucleotide polymorphisms (SNPs) have been identified in MDR1, including C1236T, G2677T/A and C3435T in exons 12, 21 and 26, respectively, and these functionally important mutations can form different haplotypes. Both SNPs and haplotypes have been demonstrated as highly polymorphic among individuals and different ethnic groups6,7,8. The genetic polymorphisms of MDR1 have been implicated as one of the factors resulting in CsA pharmacokinetic variation.
Co-administration with diltiazem has been frequently used, and this treatment might have beneficial effects beyond the economic impact associated with the dose reduction of CsA. Indeed, diltiazem is relatively safe, showing a useful antihypertensive action, potentially exhibiting blood pressure control and renal protection9. It has been reported that the CsA dosage was 12% lower in the diltiazem group than that in the non-diltiazem group at one year after transplantation. Furthermore, the diltiazem group might be associated with significantly lower probability to develop chronic allograft nephropathy than the non-diltiazem group10.
However, the correlation between MDR1 genetic polymorphisms and cyclosporine concentration when diltiazem is co-administered remains unclear. Therefore, in the present study, we retrospectively compared the impact of the MDR1 SNP/haplotype on cyclosporine concentration with and without diltiazem co-administration to assess the influence of diltiazem on the association of MDR1 genetic polymorphisms with cyclosporine concentration.
Materials and methods
Patients
This study was conducted between June 2008 and December 2011, involving a total of 126 renal transplant recipients (82 males, 44 females) who underwent transplantation at the Department of Organ Transplant, The First Affiliated Hospital, Sun Yat-sen University and were enrolled during outpatient visits at the Renal Transplant Clinic, The First Affiliated Hospital, Sun Yat-sen University. The average age of the patients was 29.15±15.36 years (range, 18–74 years), and the average body weight was 56.65±9.82 kg. All patients were maintained on a triple immunosuppressive regimen comprising CsA, mycophenolate mofetil and steroids, and the average time of post-transplantation was 25 months. During the experimental period, oral prednisolone was administered at 10 mg/d and mycophenolate mofetil was administered at 1 g bid. Diltiazem, as a CsA-sparing agent, was administered at 90 mg/d as a single daily dose to 76 patients. The patients did not receive any other drugs, such as calcium channel blockers (nicardipine and verapamil), antiepileptics (phenytoin and carbamazepine), antimycotics (fluconazole and ketoconazole), or macrolide antibiotics (erythromycin and clarithromycin), which interact with CsA. Patients fulfilling the above criteria were included. This study was performed in accordance with the Declaration of Helsinki, and ethical approval was obtained from the Ethical Committee of Sun Yat-sen University, Guangzhou, China. Written informed consent was obtained from all subjects.
CsA dosage and quantitation
The dosage of CsA was 2–4 mg·kg−1·d−1 and the daily dosage was adjusted, according to the blood trough CsA concentration (C0), to a target concentration of 100–120 ng/mL. The body weight, CsA dosage, and whole blood concentration were recorded at 5 d after the patient was administered the same dosage of CsA.
CsA was administered daily, in equal amounts, at 8:00 AM and 8:00 PM. To determine the trough concentration (C0), blood samples (using ethylenediaminetetraacetic acid as an anticoagulant) were collected at 8:00 AM, prior to administering the morning dose. The samples were assayed using the commercially available CsA whole blood monoclonal antibody fluorescence polarization assay (FPIA; TDx; Abbott Laboratories, Chicago, IL, USA)11. The weight-adjusted CsA dosage (mg·kg−1·d−1) and the adjusted concentration (ng/mL per mg·kg−1·d−1) were calculated.
Genotyping the MDR1 polymorphism
Total DNA was extracted from the peripheral leukocytes obtained from the subjects using the phenol-chloroform extraction method as previously described12. Polymerase chain reaction, followed by restriction fragment length polymorphism analysis (PCR-RFLP) was used to genotype the MDR1 polymorphisms, with only slight modifications13,14. Details regarding the primer sequences and restriction enzymes used in the present study are shown in Table 1.
Statistical analysis
The data were analyzed using the computer software SPSS (Statistical Package for the Social Sciences) for Windows (Version 12.0, Chicago, IL, USA). The MDR1 1236-2677-3435 haplotype analysis was performed using PHASE 2.1 software (downloaded from http://www.stat.washington.edu/stephens/phase/download.html. The adjusted trough blood concentration (ng/mL per mg/kg) and daily dose (mg/kg) required to achieve target blood concentrations were compared among individuals according to the allelic status of MDR1. The quantitative variables are expressed as the mean±standard deviation (SD). The distribution of quantitative parameters was compared between groups using parametric or nonparametric tests depending on the normality of the variables tested (Wilks-Shapiro test). For each analysis, P values less than 0.05 were considered statistically significant.
Results
Influence of diltiazem on CsA trough and adjusted trough concentrations
One hundred twenty-six Chinese renal transplant patients were enrolled in this study and divided into Dil(+) (n=76) and Dil(−) (n=50) groups (Table 2). As shown in Table 3, significantly different daily dosages were observed between Dil(+) and Dil(−) groups (2.76±0.78 versus 3.61±0.97 mg/kg, P<0.001). The adjusted CsA trough concentrations were significantly higher in the Dil(+) group than in the Dil(−) group during the stable stage in Chinese renal transplant patients (47.32±11.71 versus 32.87±7.62 ng/mL per mg/kg, P<0.001).
Influence of MDR1 genotypes on CsA trough and adjusted trough concentrations
The distribution of the MDR1 C1236T, G2677T/A, and C3435T alleles was consistent with Hardy-Weinberg equilibrium (each P>0.05). As shown in Table 4, there were no significant differences in the CsA trough concentrations, adjusted trough concentrations and daily dosage among different MDR1 C1236T genotype groups in both patients who used diltiazem and those who did not use diltiazem during the stable stage.
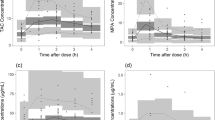
As shown in Figure 1, 2, and Table 5, the adjusted CsA trough concentration was significantly higher in MDR1-2677TT carriers than in GG and GT carriers in the Dil(+) group, showing 61.31±12.93 versus 52.25±7.83 and 39.70±7.26 ng/mL per mg/kg, respectively (P=0.004). Moreover, these differences were also observed in the Dil(−) group, showing 43.27±5.95 versus 35.22±7.55 plus 29.54±5.35 ng/mL per mg/kg, respectively (P=0.001). The adjusted CsA trough concentrations were increased with the increasing number of 2677-T alleles in all patients during the stable stage after renal transplantation.

Correlation of MDR1-2677 genotype with the dose-adjusted trough concentration of cyclosporine in patients who co-administered with diltiazem. Dose-adjusted trough concentration of cyclosporine was significantly higher in MDR1-2677TT carriers than that in GG plus GT carriers. *A=GA+AA+AT.

Correlation of MDR1-2677 genotype with the dose-adjusted trough concentration of cyclosporine in patients who didn't use diltiazem. Dose-adjusted trough concentration of cyclosporine was significantly higher in MDR1-2677TT carriers than that in GG plus GT carriers. *A= GA+AA+AT.
As shown in Figure 3 and Table 6, the adjusted CsA trough concentrations were significantly higher in MDR1-3435TT carriers than in CC and CT carriers in the Dil(+) group, showing 58.83±13.95 versus 46.14±7.55 and 45.18±12.35 ng/mL per mg/kg, respectively (P=0.011). However, no significant difference was observed in the CsA trough concentrations, adjusted trough concentrations and daily dosage among MDR1 C3435T genotype groups in patients who did not use diltiazem.

Correlation of MDR1-3435 genotype with the dose-adjusted trough concentration of cyclosporine in patients who co-administered with diltiazem. Dose-adjusted trough concentration of cyclosporine was significantly higher in MDR1-3435TT carriers than that in CC plus CT carriers.
Influence of MDR1 haplotype on CsA adjusted trough concentrations
The most common MDR1 1236-3677-3435 haplotype was T-G-C, with a frequency of 31.2%. Other haplotypes were also detected, including C-G-C, T-T-T, T-G-T, and T-T-C, with frequencies of 26.2%, 18.7%, 10.3%, and 5.2%, respectively.
As shown in Table 7, in the Dil(+) group, significantly higher adjusted CsA trough concentrations were observed in carriers of haplotypes T-T-T and T-T-C compared with non-carriers (P=0.007 and 0.001, respectively), while haplotype T-G-C carriers had significantly lower adjusted CsA trough concentrations than non-carriers (P=0.0001). However, in the Dil(−) group, the adjusted CsA trough concentrations in carriers of haplotypes T-T-T and T-T-C were significantly higher than in non-carriers (P=0.009 and 0.004, respectively), but haplotype T-G-T carriers had significantly lower adjusted CsA trough concentrations than non-carriers (P=0.002).
Discussion
This study extensively investigated the effect of diltiazem on the relationship between genetic polymorphisms of MDR1 and CsA concentration during the stable stage after renal transplantation. In recent years, high inter-individual heterogeneity in the MDR1 gene, influencing the metabolism of digoxin15,16,17, cyclosporin18,19,20, tacrolimus21,22,23 and amlodipine24, has been described. In the present study, we explored the association of MDR1 SNPs with CsA dose requirements and adjusted concentration in renal recipients co-treated or not with diltiazem. The ultimate objective of the present study was to optimize the clinical CsA therapeutic regimen, which might lead to individualized drug dosing and improved therapeutics.
In the present study, MDR1 C1236T did not influence the adjusted CsA trough concentration during the stable stage in all patients; however, MDR1 C3435T influenced the adjusted CsA trough concentration in patients using diltiazem. These results suggest that individuals carrying the MDR1-2677TT genotype or the T-T-T or T-T-C MDR1 haplotypes have a higher adjusted CsA trough concentration, regardless of co-treatment or not with diltiazem. Moreover, this result also suggests that the CsA dosage for patients with these genotypes and haplotypes might be reduced during the stable stage after renal transplantation.
The MDR1 variant alleles, 1236-T and 2677-T, significantly lower P-gp mRNA expression compared with 1236-C and 2677-G, respectively7. Dennis et al18 reported that MDR1 C3435T did not influence the dose-adjusted trough blood concentration of CsA in stable renal transplant patients. Consistent results were obtained in another study involving American renal transplant patients19. Crettol et al20 also reported that MDR1 genotypes did not influence the dose-adjusted trough blood concentration of CsA in transplant recipients. In contrast, Chinese renal transplant patients showed that MDR1 G2677T/A and MDR1 haplotypes C-G-C, T-G-T and T-T-C are associated with the CsA concentration during the early post-transplant period25. Consistently, Chen et al26 also reported that MDR1 SNPs and haplotypes were associated with C(2) and C(0) of CsA in 115 Chinese patients at 1 week and 1 month after renal transplantation. The MDR1 2677G allele has also been associated with a high CsA dose requirement to prevent renal allograft rejection in North India patients27.
In the present study, we observed a relationship between the MDR1C1236T or the MDR1G2677T polymorphism and the adjusted CsA concentration in Chinese renal recipients, regardless of diltiazem use during the stable stage. This result indicated a positive correlation between the number of MDR12677T alleles and adjusted CsA trough blood concentrations, showing that every T allele was associated with an approximate 20% increment in adjusted trough blood concentrations of CsA.
However, considering the relationship between MDR1 C3435T and the CsA concentration, we only observed a significant association in patients using diltiazem. Among the 50 SNPs of the MDR1 gene, the mutation at position 3435 in exon 26 is the only silent polymorphism identified to date that might influence P-gp expression in different human tissues and different ethnic groups28. Previous studies have reported similar results, showing that MDR1 C3435T did not influence the adjusted CsA trough blood concentration in patients who did not use diltiazem during the early and stable post-transplant periods18,20,25. We cannot explain this change in relationship; however, we speculate that this change might partially reflect the nature of diltiazem, which is a substrate and inhibitor of P-gp.
In the present study, the whole blood CsA concentration was measured using the FPIA method. It has previously been reported that most of the analytical methods were specific for the parent drug, although some discrepancies in the results were obtained between high-performance liquid chromatography and fluorescence polarization immunoassays (FPIA). This overestimation might reflect cross-reactivity with CsA metabolites, even when monoclonal antibodies are used in the immunoassays8,11,28. In the present study, the co-administration of diltiazem affected the correlation between MDR1 genetic polymorphisms and CsA blood concentrations, likely reflecting the reaction of FPIA with CsA and its metabolites. Thus, further mechanistic studies are needed to explain these findings.
In the present study, we investigated the impact of MDR1 haplotypes derived from SNPs C1236T, G2677T and C3435T on the adjusted CsA trough concentration in renal transplant patients and observed that the adjusted CsA concentration in carriers of haplotypes T-T-T and T-T-C was significantly higher than in non-carriers. Chowbaya et al29 reported that CsA exposure (AUC0–4 h, AUC0–12 h and Cmax) was higher in patients with the T-T-T haplotype than in heart transplant patients with the C-G-C haplotype. However, Ingrid et al30 showed that MDR1 haplotypes derived from the SNPs G2677T (exon 21) and C3435CT (exon 26) are not associated with cyclosporine pharmacokinetics in renal transplant patients. Therefore, prospective studies using a large sample size might be needed to explore the impact of MDR1 haplotypes on the CsA adjusted concentration.
In conclusion, the results of the present study demonstrated that the adjusted CsA trough concentration was significantly higher in MDR1-3435TT carriers than that in CC and CT carriers among patients using diltiazam; however, these differences were not observed in patients who did not use diltiazam. We also observed that G2677T/A SNPs and T-T-T and T-T-C haplotypes in MDR1 are associated with higher CsA trough concentrations in Chinese renal transplant patients, regardless of the co-administration or not of diltiazem during the stable post-transplant period. The identification of MDR1 SNPs and haplotypes and the use of diltiazem might have a clinically significant impact on allograft outcome and might provide pre-transplant pharmacogenetics information to individualize the CsA dosage.
Author contribution
Yi-xi WANG, Jia-li LI, Min HUANG, and Chang-xi WANG designed the study; Yi-xi WANG, Jia-li LI, and Yu ZHANG performed the experiments; Yi-xi WANG, Jia-li LI, and Xue-ding WANG contributed new reagents or analytic tools; Yi-xi WANG and Jia-li LI analyzed the data; and Yi-xi WANG and Jia-li LI drafted the manuscript.
References
Lindholm A, Henricsson S, Dahlqvist R . The effect of food and bile acid administration on the relative bioavailability of cyclosporin. Br J Clin Pharmacol 1990; 29: 541–8.
Kahan BD, Keown P, Levy GA, Johnston A . Therapeutic drug monitoring of immunosuppressant drugs in clinical practice. Clin Ther 2002; 24: 330–50.
Lown KS, Mayo RR, Leichtman AB, Hsiao HL, Turgeon DK, Schmiedlin-Ren P, et al. Role of intestinal P-glycoprotein (mdr1) in interpatient variation in the oral bioavailability of cyclosporine. Clin Pharmacol Ther 1997; 62: 248–60.
Schinkel AH, Wagenaar E, Mol CA, van Deemter L . P-glycoprotein in the blood-brain barrier of mice influences the brain penetration and pharmacological activity of many drugs. J Clin Invest 1996; 97: 2517–24.
Cordon-Cardo C, O'Brien JP, Casals D, Rittman-Grauer L, Biedler JL, Melamed MR, et al. Multidrug-resistance gene (P-glycoprotein) is expressed by endothelial cells at blood-brain barrier sites. Proc Natl Acad Sci U S A 1989; 86: 695–8.
Kim RB, Leake BF, Choo EF, Dresser GK, Kubba SV, Schwarz UI, et al. Identification of functionally variant MDR1 alleles among European Americans and African Americans. Clin Pharmacol Ther 2001; 70: 189–99.
Moriya Y, Nakamura T, Horinouchi M, Sakaeda T, Tamura T, Aoyama N, et al. Effects of polymorphisms of MDR1, MRP1, and MRP2 genes on their mRNA expression levels in duodenal enterocytes of healthy Japanese subjects. Biol Pharm Bull 2002; 25: 1356–9.
Kim YO, Kim MK, Woo YJ, Lee MC, Kim JH, Park KW, et al. Single nucleotide polymorphisms in the multidrug resistance 1 gene in Korean epileptics. Seizure 2006; 15: 67–72.
Bleck JS, Thiesemann C, Kliem V, Christians U, Hecker H, Repp H, et al. Diltiazem increases blood concentrations of cyclized cyclosporine metabolites resulting in different cyclosporine metabolite patterns in stable male and female renal allograft recipients. Br J Clin Pharmacol 1996; 41: 551–6.
Mezzano S, Flores C, Ardiles L, Foradori A, Elberg A . Study of neoral kinetics in adult renal transplantation treated with diltiazem. Transplant Proc 1998; 30: 1660–2.
Sabate I, Ginard M, Gonzalez JM, Baro E, Acebes G, Cuadros J, et al. Evaluation of the AxSYM monoclonal cyclosporin assay and comparison with radioimmunoassay. Ther Drug Monit 2000; 22: 474–80.
Blin N, Stafford DW . A general method for isolation of high molecular weight DNA from eukaryotes. Nucleic Acids Res 1976; 3: 2303–8.
Ameyaw MM, Regateiro F, Li T, Liu X, Tariq M, Mobarek A, et al. MDR1 pharmacogenetics: frequency of the C3435T mutation in exon 26 is significantly influenced by ethnicity. Pharmacogenetics 2001; 11: 217–21.
Li D, Zhang GL, Lou YQ, Li Q, Wang X, Bu XY . Genetic polymorphisms in MDR1 and CYP3A5 and MDR1 haplotype in mainland Chinese Han, Uygur and Kazakh ethnic groups. J Clin Pharm Ther 2007; 32: 89–95.
Schinkel AH, Wagenaar E, van Deemter L, Mol CA, Borst P . Absence of the mdr1a P-Glycoprotein in mice affects tissue distribution and pharmacokinetics of dexamethasone, digoxin, and cyclosporin A. J Clin Invest 1995; 96: 1698–705.
Johne A, Kopke K, Gerloff T, Mai I, Rietbrock S, Meisel C, et al. Modulation of steady-state kinetics of digoxin by haplotypes of the P-glycoprotein MDR1 gene. Clin Pharmacol Ther 2002; 72: 584–94.
Kurzawski M, Bartnicka L, Florczak M, Gornik W, Drozdzik M . Impact of ABCB1 (MDR1) gene polymorphism and P-glycoprotein inhibitors on digoxin serum concentration in congestive heart failure patients. Pharmacol Rep 2007; 59: 107–11.
Hesselink DA, van Schaik RH, van der Heiden IP, van der Werf M, Gregoor PJ, Lindemans J, et al. Genetic polymorphisms of the CYP3A4, CYP3A5, and MDR-1 genes and pharmacokinetics of the calcineurin inhibitors cyclosporine and tacrolimus. Clin Pharmacol Ther 2003; 74: 245–54.
Haufroid V, Mourad M, Van Kerckhove V, Wawrzyniak J, De Meyer M, Eddour DC, et al. The effect of CYP3A5 and MDR1 (ABCB1) polymorphisms on cyclosporine and tacrolimus dose requirements and trough blood levels in stable renal transplant patients. Pharmacogenetics 2004; 14: 147–54.
Crettol S, Venetz JP, Fontana M, Aubert JD, Pascual M, Eap CB . CYP3A7, CYP3A5, CYP3A4, and ABCB1 genetic polymorphisms, cyclosporine concentration, and dose requirement in transplant recipients. Ther Drug Monit 2008; 30: 689–99.
Mai I, Perloff ES, Bauer S, Goldammer M, Johne A, Filler G, et al. MDR1 haplotypes derived from exons 21 and 26 do not affect the steady-state pharmacokinetics of tacrolimus in renal transplant patients. Br J Clin Pharmacol 2004; 58: 548–53.
Roy JN, Barama A, Poirier C, Vinet B, Roger M . Cyp3A4, Cyp3A5, and MDR-1 genetic influences on tacrolimus pharmacokinetics in renal transplant recipients. Pharmacogenet Genomics 2006; 16: 659–65.
Akbas SH, Bilgen T, Keser I, Tuncer M, Yucetin L, Tosun O, et al. The effect of MDR1 (ABCB1) polymorphism on the pharmacokinetic of tacrolimus in Turkish renal transplant recipients. Transplant Proc 2006; 38: 1290–2.
Kim KA, Park PW, Park JY . Effect of ABCB1 (MDR1) haplotypes derived from G2677T/C3435T on the pharmacokinetics of amlodipine in healthy subjects. Br J Clin Pharmacol 2007; 63: 53–8.
Wang Y, Wang C, Li J, Wang X, Zhu G, Chen X, et al. Effect of genetic polymorphisms of CYP3A5 and MDR1 on cyclosporine concentration during the early stage after renal transplantation in Chinese patients co-treated with diltiazem. Eur J Clin Pharmacol 2009; 65: 239–47.
Chen B, Zhang W, Fang J, Jin Z, Li J, Yu Z, et al. Influence of the MDR1 haplotype and CYP3A5 genotypes on cyclosporine blood level in Chinese renal transplant recipients. Xenobiotica 2009; 39: 931–8.
Singh R, Kesarwani P, Srivastava A, Mittal RD . ABCB1 G2677 allele is associated with high dose requirement of cyclosporin A to prevent renal allograft rejection in North India. Arch Med Res 2008; 39: 695–701.
Wacke R, Drewelow B, Hehl EM, Riethling AK . Measurement of cyclosporin A in whole blood by RIA, EMIT and FPIA: a comparative study. Int J Clin Pharmacol Ther Toxicol 1992; 30: 502–3.
Chowbay B, Cumaraswamy S, Cheung YB, Zhou Q, Lee EJ . Genetic polymorphisms in MDR1 and CYP3A4 genes in Asians and the influence of MDR1 haplotypes on cyclosporin disposition in heart transplant recipients. Pharmacogenetics 2003; 13: 89–95.
Mai I, Stormer E, Goldammer M, Johne A, Kruger H, Budde K, et al. MDR1 haplotypes do not affect the steady-state pharmacokinetics of cyclosporine in renal transplant patients. J Clin Pharmacol 2003; 43: 1101–7.
Acknowledgements
This work was supported by the National Major Projects for Science and Technology Development from the Science and Technology Ministry of China (No 2009ZX09304-003), the National Natural Science Foundation of China (No 30572231, 30873124 and 30873125) and the Science and Technology Planning Project of Guangdong Province (No 2007B031511001). We also received financial support from the National Major Projects for Science and Technology Development from Science and Technology Ministry of China (Grant No 2012ZX09506001-004) and the National Natural Science Foundation of China (No 81202600, 81102515, 81072708 and 81173131). The authors would like to thank all doctors, nurses and patients who participated in this study.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Wang, Yx., Li, Jl., Wang, Xd. et al. Diltiazem augments the influence of MDR1 genotype status on cyclosporine concentration in Chinese patients with renal transplantation. Acta Pharmacol Sin 36, 855–862 (2015). https://doi.org/10.1038/aps.2015.6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/aps.2015.6
Keywords
This article is cited by
-
Drug–drug–gene interactions and adverse drug reactions
The Pharmacogenomics Journal (2020)
-
Population Pharmacokinetic Modeling of Diltiazem in Chinese Renal Transplant Recipients
European Journal of Drug Metabolism and Pharmacokinetics (2018)
