
Abstract
Aim:
To examine the electrophysiological effects of sophocarpine on action potentials (AP) and ionic currents of cardiac myocytes and to compare some of these effects with those of amiodarone.
Methods:
Langendorff perfusion set-up was used in isolated guinea pig heart, and responses to sophocarpine were monitored using electrocardiograph. Conventional microelectrode, voltage clamp technique and perforated patch were employed to record fast response AP (fAP), slow response AP (sAP) and ionic currents in guinea pig papillary muscle or rabbit sinus node cells.
Results:
Tachyarrhythmia produced by isoprenaline (15 μmol/L) could be reversed by sophocarpine (300 μmol/L). Sophocarpine (10 μmol/L) decreased the amplitude by 4.0%, maximal depolarization velocity (Vmax) of the fAP by 24.4%, and Na+ current (INa) by 18.0%, while it prolonged the effective refractory period (ERP) by 21.1%. The same concentration of sophocarpine could also decrease the amplitude and Vmax of the sAP, by 26.8% and 25.7%, respectively, and attenuated the Ca2+ current (ICaL) and the K+ tail current substantially. Comparison of sophocarpine with amiodarone demonstrated that both prolonged the duration and the ERP of fAP and sAP, both decreased the amplitude and Vmax of the fAP and sAP, and both slowed the automatic heart rate.
Conclusion:
Sophocarpine could reverse isoprenaline-induced arrhythmia and inhibit INa, ICaL, and IKr currents. The electrophysiological effects of sophocarpine are similar to those of amiodarone, which might be regarded as a prospective antiarrhythmic agent.
Similar content being viewed by others


Introduction
Sophora flavescens is a traditional Chinese medicine that has been used for nearly 2000 years in China. It contains several types of alkaloids such as aloperin, matrine and sophocarpine. Some reports have found that Sophora flavescens has antiarrhythmic effects. Matrine, one extract from Sophora flavescens, was able to decrease abnormal spontaneous activities of the rat right atrium at 220 μmol/L1. It was also reported that matrine protects against aconitine-induced arrhythmia2. In 2008, Chen et al reported that sophocarpine could inhibit ouabain-induced arrhythmias in guinea pigs3.
Zhang et al4 found that sophocarpine, the extract from Sophora flavescens, was an effective drug in the treatment of viral myocarditis, not only for its antiviral effects, but also for its antiarrhythmic properties. According to Chen's data5, 220 patients were enrolled in the sophocarpine therapeutic group, most of whom had shown different types of extra systoles. After treatment with sophocarpine (5–6 mg/kg in 500 mL of 5% glucose, iv for 4 h/d, 2–4 weeks as a course), the case analyses indicated that the antiarrhythmic efficiency of sophocarpine had reached 89.7%. Among these patients, complete data from 24 h Holter records were available for 49; the average number of extra systole cycles was decreased from 6120±3966 to 112±179 by sophocarpine in these patients. This report was very impressive, but the mechanism for its antiarrhythmic action needed to be further resolved. Chen et al6 reported that sophocarpine could prolong the effective refractory period and raise the ventricular fibrillation threshold. However, those results were not enough to explain the drug's efficacy in clinical use.
In spite of those experimental studies and case reports, very little work has been done regarding the electrophysiological effects of sophocarpine on the heart, cardiac myocytes and ion channels. The aim of this paper was to fully study the electrophysiological properties of sophocarpine and explore the mechanism of its antiarrhythmic function. We took 3 steps to fulfill this purpose: first, we tried to confirm whether sophocarpine had antiarrhythmic effects in an arrhythmic model; second, we studied the effects of sophocarpine on action potentials (AP), whole cell and single channel currents to understand its electrophysiological properties; and third, we intended to compare the effects of sophocarpine with those of some known antiarrhythmic drugs.
Materials and methods
In the experiments, all of the procedures were approved by the Animal Care and Use Committee at Shanghai Jiaotong University. The investigation conforms to the Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No 85–23, revised 1996).
Solution preparation and materials
Tyrode's solution for perfusion preparations consisted of the following (in mmol/L): NaCl, 138; KCl, 5.4; CaCl2, 1.8; MgCl2, 1; glucose, 10; and HEPES, 10; pH 7.4±0.05 saturated by 100% O2.
For whole cell Na+ current recordings, the pipette solution contained (in mmol/L): KCl, 120; CaCl2, 0.1; MgCl2, 2; EGTA, 1.1; and HEPES, 10; pH 7.2. The bath solution was Tyrode's solution.
For inside-out Na+ channel current recording, the bath solution was (in mmol/L): KCl, 120; MgCl2, 2; CaCl2, 0.1; HEPES, 10; and EGTA, 1.1; pH 7.4, while the pipette solution contained (in mmol/L): NaCl, 180; KCl, 1.3; MgCl2, 0.5; CaCl2, 1.5; glucose, 5; HEPES, 5; CoCl2, 3; TEA, 10; 4-AP, 10; and CsCl, 10; pH 7.2.
The pipette solution for the perforated patch clamp contained (in mmol/L): K-aspartate, 130; MgCl2, 2; CaCl2, 5; EGTA, 11; Na-HEPES, 10; and Na2-ATP, 2; pH 7.2. The concentration of amphotericin B was 240 μmol/L.
Sophocarpine (13,14-didehydromatridin-15-one, Mw 246.2, purity 99.7%, Figure 1A) was provided by Shanghai Institute of Pharmaceutical Industry (Shanghai, China). The injection solution of sophocarpine (10 g/L), produced by Shanghai Hejia Pharmaceutical Company (No 030827), was diluted to the final concentrations for the experiments. Amiodarone was purchased from the Mingzhu Pharmaceutical Factory of Sanofi-aventis China.

Sophocarpine (Soph) reversed the tachyarrhythmia of guinea pig. A: Molecular structure of soph. B: Soph reversed the isoprenaline-induced tachyarrhythmia of guinea pig. (a) Control ECG. (b) The tachyarrhythmia was initiated after 6 min perfusion of the heart with isoprenaline 15 μmol/L. (c) The tachyarrhythmia began to be reversed after the heart had been exposed to Soph (300 μmol/L) plus isoprenaline solution for 13 min. (d) Two minutes later, the regular beating appeared on the ECG in the Soph-isoprenaline-contained solution. (e) The tachyarrhythmia recurred after Soph had been washed out for 7 min with the same solution as the one used in trace b.
Chromanol 293B was provided by Aventis Pharma (Frankfurt, Germany), dofetilide by EGIS Pharmaceuticals Ltd (Pfizer Global Research & Development, UK, Batch 3644–399). Chromanol 293 B and dofetilide were initially dissolved in 100% DMSO to make a stock solution (10 mmol/L).
Electrocardiogram (ECG) recording in isolated guinea pig hearts
Guinea pigs (weighing approximately 250–300 g) of either sex were anesthetized with an intraperitoneal injection of urethane (20%, 5 mL/kg). The hearts were quickly taken out of the chest and perfused using a Langendorff perfusion setup at the recorded pressure of 80 cm H2O. The temperature of Tyrode's solution was maintained at 37±0.5 °C. Three platinum electrodes, which had been placed on the cardiac apex, right atrium, and aortic root, were used to record the ECG. The signals were documented on a computer with the PowerLab system (PowerLab ML135, ML 785, ADInstruments, Australia)7.
Primary culture of neonatal rat ventricular myocytes
Neonatal Sprague-Dawley (SD) rats of either sex (postnatal 1 d) were anesthetized by intraperitoneal injection of urethane (20%, 5 mL/kg). After the heart had been taken out, the ventricles were cut into small pieces and processed by collagenase-containing solution for digestion. The myocytes were separated from the cell suspension by centrifuging twice. The isolated ventricular myocytes were planted and grown on glass coverslips in DMEM (Invitrogen, Burlington, OH, USA) with 10% fetal bovine serum for 5-6 d8, 9.
Preparation of guinea pig papillary muscles and rabbit sinus node
Guinea pigs (250–300 g) or rabbits (1.5–2.5 kg) of either sex were sacrificed by venesection under deep anesthesia with an intravenous injection of sodium pentobarbital (30 mg/kg). The hearts were rapidly removed into the dissection chamber filled with Tyrode's solution. The right ventricular papillary muscles (from guinea pig) or the sinus nodes with partial right atrium (from rabbit) were excised and pinned to the bottom of a recording chamber. The chamber was perfused with Tyrode's solution at a constant rate of 3 mL/min and maintained at a temperature of 37±0.5 °C7, 10.
Recording of the fast-response and slow-response AP
Bipolar platinum electrodes were used to drive the preparations with rectangular current pulses at a stimulation frequency of 1 Hz for papillary muscle and 2.2 Hz for the sinus node. Each pulse lasted 0.1 ms with a strength of about 1.5 times the threshold value. After 30 min of stimulation, transmembrane AP was recorded by a conventional glass microelectrode that was filled with 3 mol/L KCl and had a tip resistance of 15–20 MΩ. The records were sampled and stored in the computer through the amplifier (MEZ8201, Nihon Kohden, Japan) and PowerLab interface (PowerLab ML785, ADInstruments, Australia)7, 10. The calculated parameters for the fast response AP included the resting potential (RP), the action potential amplitude (APA), the maximal depolarization velocity (Vmax), the action potential duration (APD50 and APD90), and the effective refractory period (ERP). To measure the ERP, the preparations of guinea pig were driven by a series of 8 stimuli pulses at a frequency of 1 Hz. Following the last pulse, an additional test pulse was added. By adjusting the time interval between the eighth pulse and the test stimulus, which was able to elicit an extra AP, the minimum interval was calculated as the ERP.
In our study of the sinus node, the parameters of the slow response AP were measured as APA, Vmax, APD90, the maximum repolarization potential (MRP) and the spontaneous depolarization rate (SDR) in phase 4.
Voltage clamp experiment
The patch clamp technique was used to record the whole-cell and single channel currents. The cells were perfused with the bath solution mentioned above at a rate of 3 mL/min. The protocol for whole cell current recording is shown in the Results section.
Single Na+ channel current was recorded in an inside-out configuration. Since K+ and Ca2+ channels were blocked by TEA, 4-AP, CoCl2, and CsCl in the pipette solution11, the only channel that allowed an inward current to pass through would be the Na+ channel.
Regarding the whole cell calcium current recording, the perforated patch clamp technique described in detail by our previous papers12, 13 was used to prevent the run-down of calcium current. The perfusion solution contained 4-aminopyridine (4-AP, Sigma, USA), which was used to block the transient outward current (Ito) to reveal the Ca2+ current. An oscilloscope (DSS6521, Kikusui, Japan) and Axopatch-1D amplifier (Axon Instruments, Foster City, CA, USA) were used to monitor and record the clamped voltage and channel currents. The data were sampled with the Clampex 9.0 software suite (Axon Instruments) and stored in the computer through the interface (Digidata 1320, Axon Instruments). The sample rate was 100 kHz with a filtering frequency of 10 kHz.
Statistical analysis
Chart 5 (ADInstruments, Australia) software, Clampex 9.0, and Origin 6 (Microcal Software, Inc, USA) were used for measurement and statistical analysis. All of the results were expressed as means±SEM. Statistical significance was determined using Student's t-test for paired data. P<0.05 was considered statistically significant.
Results
Sophocarpine did exert an anti-arrhythmic effect
During tachyarrhythmia modeling, the heart was first perfused with isoprenaline (15 μmol/L)-containing Tyrode's solution. About 6–8 min later, the tachyarrhythmia or ventricular fibrillation was initiated and recorded. After that, sophocarpine was added to the isoprenaline-containing perfusion solution. About 11–17 min later, the tachyarrhythmia or the ventricular fibrillation was stopped, and the regular heartbeats appeared again on the ECG. Six guinea pig hearts were subjected to this protocol. All of them developed the tachyarrhythmia produced by isoprenaline, and all of the tachyarrhythmia was inhibited by sophocarpine (300 μmol/L). Isoprenaline increased the heart rate from 218±26 to 284±37 beats/min, leading to tachyarrhythmia; in contrast, sophocarpine returned the heart rate to 179±24 beats/min and finally stopped the tachyarrhythmia. The washing out of sophocarpine and isoprenaline returned the heart rate to 207±28 beats/min. Figure 1B-e shows that after the sophocarpine had been washed out with the same isoprenaline-containing solution, the tachyarrhythmia recurred.
The cardiac electrophysiological properties of sophocarpine
Four types of experiments were carried out to study the electrophysiological properties of sophocarpine: 1) recording of the fast response AP, 2) recording of the slow response AP, 3) measuring of Na+ current in whole cell and single channel configurations, and 4) observing the changes in Ca2+ and K+-tail currents.
The effects of sophocarpine on the fast response AP of ventricular cells
After the APs of the guinea pig papillary muscles had stabilized, the preparations were then perfused consecutively with different concentrations of sophocarpine-containing Tyrode's solution. Each perfusion lasted for about 8–10 min; meanwhile the RP, APA, Vmax, and APD were measured7.
The effective refractory period was obtained by an extra super-threshold stimulus, which was applied during different repolarizing phases of the AP. Figure 2A shows that the APA was decreased while the APD and the effective refractory periods of the AP were dose-dependently prolonged by sophocarpine. The data from 6 experiments are presented in Table 1.

The effects of sophocarpine (Soph) and amiodarone (Amio) on the fast response AP of guinea pig papillary muscle and the slow response AP of rabbit sinus node cells. A: The superimposed traces of the AP with the extra responses in different concentrations of Soph. The short upward straight lines before the AP and the each extra-response (a′, b′, and c′) were stimulus artifacts. The figure showed that Soph not only decreased the APA (from trace a to c) but also prolonged the action potential durations and the effective refractory period (ERP) in a dose-dependent manner, and at the same time it did not change the resting membrane potential very much. (a) Control; (b) Soph 1 μmol/L. (c) Soph 10 μmol/L. B: The effect of Amio on the AP. (a) Control; (b) Amio 1 μmol/L; (c) Amio 10 μmol/L. C: The superimposed action potential traces of sinus node with different concentrations of Soph. The short vertical bars before APs were the stimulus artifacts. Soph dose-dependently decreased the APA and prolonged the APD (from trace a to c). (a) Control; (b) Soph 0.5 μmol/L; (c) Soph 1 μmol/L.
For measurement of the dose relationship between APD and sophocarpine, the concentrations of sophocarpine used ranged from 1 to 100 μmol/L. EC50(median effective concentration) of the prolonged APD90 was 5.93 μmol/L; the dose response curve is presented in Figure 3.

Dose-response of the APD90 of the papillary muscle to sophocarpine (Soph). Abscissa, concentration of Soph. Ordinate, normalized percentage changes of APD90 by Soph (n=5). Data was fitted with Exponential Decay Function. EC50 was 5.93 μmol/L.
The effect of sophocarpine on the slow response AP of rabbit sinus node
In order to observe the effect of sophocarpine on the slow response AP of sinus node, the preparation of rabbit sinus node had to be driven by electric stimulus at the rate of 130 times/min (faster than its own spontaneous beating). In this way, we could eliminate the influence of the varying rhythm of spontaneous activity of the sinus node on the APD; otherwise, it might interfere with the calculation of the AP parameters, for it is known that the faster the heart beats, the shorter the APD will be. In those experiments, the stimulated APs were recorded by glass microelectrode10. The changes in AP parameters induced by sophocarpine are listed in Table 2. Figure 2C presents results from 5 experiments on the sinus node. In Figure 2C, the decreases in both the APA and the Vmax were observed after the application of different concentrations of sophocarpine. Furthermore, the APD90 was also prolonged by sophocarpine, which was in accordance with the results from the fast response AP recordings (Figure 2A).
The possible mechanism for the sophocarpine-mediated prolongation of the APD
Chromanol 293 B14 specifically blocks IKs, while dofetilide15 blocks IKr. In this experiment, chromanol 293 B was first applied to block IKs, and then sophocarpine with different concentrations was consecutively added to the perfusing solution. Figure 4-IA shows that the prolongation of APD induced by chromanol 293 B (trace b) was further increased by sophocarpine (trace c and d), which suggests that sophocarpine might inhibit IKr, resulting in the increased APD. To confirm this, the following protocol was used (Figure 4-IB): Dofetilide was first used to inhibit the IKr, leading to the increase in APD (trace b); then sophocarpine at different concentrations was added to the perfusing solution. Figure 4-IB demonstrates that the APD was no longer affected by sophocarpine (traces c and d). The above results indicate that sophocarpine could block IKr rather than IKs, leading to prolongation of the APD. Figure 4-II presents the 5 experimental results with the washing-out data.

Sophocarpine (Soph) inhibits IKr. Soph1, sophocarpine 5 μmol/L. Soph2, sophocarpine 10 μmol/L. Dofe: dofetilide 1 μmol/L. 293B, chromanol 293B of 15 μmol/L. Amio: amiodarone 10 μmol/L. Part I A: the effect of Soph on APD after the IKs had been blocked by chromanol 293B. B: the effect of Soph on APD after IKr had been blocked by Dofe. Section C: Amio did not prolong APD after the action of Soph. Part II The statistical data (n=5) showing the percentage changes of APD90 by different drugs as indicated in part I A and B. Ordinate: normalized percentage changes of APD90. Abscissa: the symbols corresponded to those of the Part I plus the washing out. bP<0.05, cP<0.01 vs control. eP<0.05 vs 293B+Soph1.
The effect of sophocarpine on the cardiac Na+ current
The action of sophocarpine on the cardiac Na+ current was carried out in 2 experimental levels: the whole cell INa recording and single Na+ channel current recording.
Sophocarpine decreased the whole cell INa
Whole cell current recording was carried out in enzyme-isolated ventricular cells of neonatal rat heart. The cell was depolarized from the holding potential (−110 mV) to the testing potential (−50 mV) for 300 ms before it was returned to the holding potential. The initial large inward current was invoked by depolarization clamping, as shown in Figure 5A. As this inward current had been blocked by the special Na+ channel blocker TTX 10 μmol/L (not shown), this current could be regarded as INa7. After the cell was perfused with sophocarpine (10 μmol/L), the inward current was decreased substantially. From 3 experiments that involved whole cell recordings, the average decrease of the INa induced by sophocarpine (10 μmol/L) was about 18.0%.

Sophocarpine (Soph) decreased the early Na+ current. A: Soph decreased INa in the whole cell recording configuration. The upper half showed the whole cell sodium current recordings; the lower one was the voltage clamp protocol. (a) control inward current. (b) The decreased current by Soph 10 μmol/L. B: Soph decreased the Na+ current in the single channel recording configuration. The upper parts (a, b, c, d) referred to the channel current recording; the lower was the voltage clamp protocol. (a) a group of control traces. (b) the traces after Soph 30 μmol/L. (c and d) the averaged inward currents which were calculated before and after the Soph from 43 and 35 trails respectively.
Sophocarpine inhibited single Na+ channel activity
Single Na+ channel current recordings were carried out in an inside-out configuration on isolated ventricular myocytes from neonatal rats. The patch membrane was first held at −110 mV and then depolarized to and clamped at −50 mV for 500 ms before it was returned to the holding potential. As the pipette solution contained Ca2+ and K+ channel blockers (see Material and methods section), the recorded channel current may have represented the Na+ current.
Single channel openings were observed on the recording traces. Both the open occurrences and the averaged inward current were decreased after the cells had been perfused with a sophocarpine (30 μmol/L)-containing solution in 3 experiments. Figure 5B shows one of the results.
Sophocarpine inhibited the ICaL of cardiac myocytes
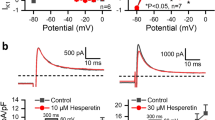
The whole cell recording configuration and perforated patch technique were used in this experiment. The ventricular cells of neonatal rat were first held at −40 mV to inactivate the Na+ channels and then depolarized to the command potential of 20 mV for 500 ms before they were returned to the holding potential (Figure 6). As 4-AP had been used to block the Ito, the inward current was clearly discernible at the command potential (Figure 6a). Sophocarpine (10 μmol/L) was then added to the perfusion solution. About 3 min later, not only had the inward current decreased, but also the tail current (outward K+ current, a') was diminished. Compared with the controls in 3 experiments, average ICaL decreased by 33.2%±11.7% at the command potential of 20 mV.

Sophocarpine (Soph) inhibited ICaL and Ik tail current. The a, b, c, and a′, b′, c′ represented ICaL and IK tail currents respectively. (a) Control. (b) Soph 10 μmol/L. (c) Washing out.
Comparison of electrophysiological effects between sophocarpine and amiodarone
From the above results, we can see that sophocarpine induced effects similar to those of class III anti-arrhythmic drug amiodarone, ie, it was also able to prolong the APD. The following experiments were designed to compare these two drugs in their effects on both the fast and the slow response AP morphologies.
Effect of amiodarone on the fast response AP
The preparation and the experimental protocol were the same as sophocarpine section. Amiodarone at a concentration of 10 μmol/L not only prolonged the APD and ERP by 11.1% and 14.7%, respectively, but also decreased the APA and Vmax. The results from 6 experiments are presented in Table 1, and one example is shown in Figure 2B.
Because our results confirmed that sophocarpine could inhibit IKr to prolong the APD and that amiodarone could block the IKr, the following experiment was designed to determine what would happen to amiodarone if sophocarpine were first used to inhibit IKr.
Figure 4-IC shows that after chromanol 293B had blocked the IKs (from trace a to trace b) leaving IKr, sophocarpine increased the APD (from b to c), and then amiodarone (at the same concentration as sophocarpine) was added to the perfusing solution. The latter had no obvious effect on the APD (traces c and d were superimposed); neither were substantial changes to the APD observed when sophocarpine was administered before amiodarone (data not shown).
The effects of amiodarone and sophocarpine on the spontaneous AP of rabbit sinus node
The preparation of rabbit sinus node did not involve electric stimulus; spontaneous APs were recorded with a glass microelectrode. After the control AP was recorded in Tyrode's solution, amiodarone (10 μmol/L) or sophocarpine (10 μmol/L) was added to the perfusion solution. About 10 min later, the changes in AP produced by the drugs were measured, and then the drugs were washed out with control Tyrode's solution. Sophocarpine-mediated inhibition of Vmax and APA started at about 2 min and reached the maximum in another 1 min. The inhibitory effect on APA or Vmax lasted stably for a considerable time. In our records, we only pre-treated the preparations for about 30–50 min and then washed them out to observe the recovery process. Full recovery could be obtained after 8 to 10 min of washing out. Figure 7 illustrates the comparison. The results from 5 experiments are shown in Table 3. In short, the data show that both drugs could decrease the APA, the Vmax and the spontaneous heart rate and that both could prolong the APD to some extent.

Sophocarpine (Soph) and amiodarone (Amio) had the similar effects on the spontaneous AP of rabbit sinus node. The traces of A, B, C, D, E, and F were spontaneous APs. A, B, C belonged to Soph experiment, and D, E, F to those of Amio's. A and D: Controls. B: Ten minutes after Soph 10 μmol/L. E: Ten minutes after Amio 10 μmol/L. C and F: Washout with the control Tyrode's solution.
Discussion
The electrophysiological effects of sophocarpine on the heart
Phase 0 of the fast response AP is initiated by the fast inward Na+ current. The APA and Vmax are related to the dynamics of this current. Our whole current experiments demonstrated that sophocarpine could substantially inhibit the INa, which would explain why sophocarpine decreased APA and Vmax in the experiment on the fast response AP. In the inside-out recording experiments, K+ and Ca2+ channels had been blocked by CoCl2, TEA, 4-AP, and CsCl in the pipette solution; hence, the inward current in Figure 5 must have been the Na+ current. The decreased opening and reduced magnitude of the Na+ channel current following sophocarpine treatment confirmed the inhibitory effect of sophocarpine on Na+ channels.
During the whole cell recording of the slow inward current (ICaL), sophocarpine substantially decreased the current. The slow response AP, such as the AP in sinus node, is initiated by the slow ICaL. The APA and Vmax of the slow AP are dependent on the dynamics or conditions of the Ca2+ channel. The decreases in APA and Vmax induced by sophocarpine could result from the inhibitory effect of sophocarpine on the Ca2+ channel.
APD is mainly related to the balance between the inward ICaL and the outward K+ current. The observed prolongations of the APD in both the fast response AP (papillary muscle myocytes) and the slow response AP (sinus node cells) mediated by sophocarpine suggest that sophocarpine could also inhibit the outward K+ current, which would result in retardation of the repolarization and prolongation of the APD. The direct evidence for sophocarpine-mediated inhibition of the K+ current is presented in Figure 6, which presents the sophocarpine-mediated reduction of the K+ tail current (Figure 6b). Notably, after IKs had been blocked by chromanol 293B, sophocarpine was capable to dose-dependently prolong the APD; however, if IKr was first inhibited by the IKr-blocker dofetilide, sophocarpine did not demonstrate this effect. Although this design was unable to rule out whether IKr was involved in the process, our results coincided with those described by Yang et al in their study of the effect of sophocarpine on HERG channel stably expressed in human embryonic kidney-293 cells13. The authors demonstrated that sophocarpine inhibited the transfected HERG channels by influencing the inactivation state16.
Sophocarpine could decrease the L-type calcium current, which might shorten the APD90 and interfere with its prolongation effect on APD17 that there are two different repolarizing currents that are activated by a rise in cytosolic calcium concentration17. One current, IK.Ca, appears to be a member of the Kv family of potassium channels; the other, Ito2, is probably a calcium-activated chloride channel. Both respond to a rise in cytosolic calcium by shortening the action potential duration, limiting further calcium entry into the heart. According to this opinion, we suppose that the reduction of the calcium current by sophocarpine would therefore have less effect on IK.Ca and be conducive to the prolongation of APD. Valenzuela et al18, in their experiments on guinea pig ventricular myocytes, found that amiodarone (16 μmol/L) induced dramatic tonic and phasic reductions of the Ca2+ current. Nonetheless, amiodarone still prolonged the APD.
The possible mechanism of the anti-arrhythmic function of sophocarpine
β-adrenergic agonists lead to the elevation of cytosolic cyclic AMP levels and the activation of protein kinase A. This kinase phosphorylates L-type Ca2+ channels and thereby increases the channel's open probability, resulting in large Ca2+ current into the cell. Normally, the inward Ca2+ current is balanced by the Ca2+ pumps located in the sarcoplasmic reticulum and cell membrane and in the Na+/Ca2+ exchangers in the cell membrane. The tachyarrhythmia produced in our experiment may be due to the use of high concentrations of isoprenaline (15 μmol/L) in the perfused solution. Isoprenaline could induce the delayed after-depolarization (DAD) by increasing sarcoplasmic reticulum (SR) Ca2+ load, leading to spontaneous SR Ca2+ release and activation of transient inward current (Iti), which underlies DADs19. Ultimately, ECG revealed tachyarrhythmia or fibrillation of the ventricle.
Tosaki et al20 reported that in the isolated rat heart, reperfusion-induced arrhythmias were exacerbated by isoproterenol (0.01–1.0 μmol/L). The proarrhythmic action of isoproterenol was primarily the result of a β1-receptor-mediated tachycardia rather than a free radical mediated process21, since it was prevented competitively by the β1-receptor antagonist metoprolol, but not by the free radical scavengers. The authors also found22 that drugs such as lidocaine, which prevent ion movements induced by some pathologic changes, protected against reperfusion-induced arrhythmias.
It has been said that 'Virtually all anti-arrhythmic drugs inhibit the opening or reactivation of voltage-gated ion channels'23. Because sophocarpine inhibited Ca2+ channel current, it was expected to relieve the Ca2+-overload produced by isoprenaline. Furthermore, sophocarpine, with its inhibitory effects on potassium and sodium currents, was not only able to prolong the effective refractory period but also able to decrease the conduction velocity via its inhibition of APA and Vmax of the AP. Those two effects might be conducive to its antiarrhythmic effect because propagation of the AP can be interrupted by those two effects if reentry occurs during tachyarrhythmia. However, one reporter showed that the increase or decrease in heart rate was closely correlated with the development of arrhythmias24. The investigation showed that increasing the heart rate in increments from 200 to 400 beats/min caused an increased incidence of ventricular fibrillation and ventricular tachycardia during reperfusion. Some researchers25 explained that a higher heart rate would cause the accumulation of extracellular potassium. Loss of cellular potassium was a critical factor in determining the vulnerability of the heart to arrhythmias. Furthermore, a lower heart rate also directly decreases the possibility of triggered activity26. In our experiment with isoprenaline, the perfused heart rate increased from 218±26 to 284±37 beats/min and tachyarrhythmia developed. After sophocarpine, the heart rate decreased to 179±24 beats/min and the tachyarrhythmia disappeared (Figure 1). In terms of Tosaki's point of view, the heart-rate-slowing effect of sophocarpine may explain one of its antiarrhythmic mechanisms. Although we have no direct evidence to support the above hypotheses or experiments to rule out whether sophocarpine could act as a β-receptor antagonist, the fact is that sophocarpine does reverse the tachyarrhythmia and fibrillation produced by isoprenaline. This antiarrhythmic function of sophocarpine has been proven by other experimental reports1, 2, 3, 4 and clinical practice5, 27.
According to Chen's clinical observations5, 27, sophocarpine has no obvious harmful effects on the functions of the liver or kidney or on the blood system. A few patients have exhibited nausea or urticaria. After a decrease in the dosage, the symptoms disappeared in a few days. A clinical trial on sophocarpine conducted by researchers at Renji Hospital has progressed from stage II to stage III. The information gathered should be illuminating.
Comparison of sophocarpine with amiodarone with regard to electrophysiological characteristics
In our preliminary experiments, we found that sophocarpine had some inhibitory effect on potassium, sodium and calcium currents, similar to amiodarone28. It has been reported that sotalol has no effects on sodium or calcium currents. That was the main reason we chose amiodarone instead of sotalol for comparison with sophocarpine. Furthermore, the clinical review maintains: Despite limited indication, amiodarone is one of the most frequently prescribed specific anti-arrhythmic drugs in the United States29, 30, 31. Amiodarone is a class III antiarrhythmic drug. It inhibits repolarizing K+ currents and so prolongs the cardiac AP; it weakly inhibits depolarizing currents, such as those mediated by the Na+ and Ca2+ channels32, 33, 34. Therefore, it was worth comparing the electrophysiological effects of these two drugs. Our results indicated that their effects were very similar: both can inhibit the APA and Vmax of the fast and the slow response APs; both can prolong the APD and the ERP of ventricular myocytes; both can decrease the automatic heartbeat and spontaneous depolarization rate in phase 4 of the sinus node AP. However, in some respects, for example in the reduction of spontaneous heart beating, amiodarone seemed more powerful than sophocarpine: 10 μmol/L amiodarone decreased the heartbeat by 36.6%, while 10 μmol/L sophocarpine decreased the heartbeat by only 26.9%. In other respects, sophocarpine could increase the APD and prolong the ERP for a little longer than amiodarone. Actually, we do not know which is more effective in clinical use, for this kind of comparison must include many other factors, such as the side effects or the kinetics of the drugs, etc. However, Li et al, in their study on the antiarrhythmic properties of long-term treatment with matrine in rats with arrhythmia induced by coronary ligation, found that long term oral administration of Martine reduced arrhythmia and mortality more effectively than did amiodarone35.
Study limitations
One limitation of the present study is the lack of a comparison between sophocarpine and amiodarone and the short-lived duration of the effects of amiodarone on INa, ICaL, and IKr currents. Thus, further studies are needed.
Another limitation is that sophocarpine has obvious inhibitory effects on the isoprenaline-induced tachyarrhythmia, yet it is still unclear which of its electrophysiological properties plays the crucial role in this action. The mechanism by which isoprenaline induces tachyarrhythmia is complicated. Either the delayed after-depolarization or the re-entry mechanisms or the changes in heart rate may take part in the process. Further study will be necessary.
Conclusion
Sophocarpine could reverse isoprenaline-induced arrhythmia and inhibit INa, ICaL, and IKr currents. The electrophysiological effects of sophocarpine are similar to those induced by amiodarone, which might be regarded as a prospective antiarrhythmic drug in clinical practice.
Author contribution
Ci-zhen LI and Yuan-mou LIU designed the research plan; Zhi-fang YANG, Ci-zhen LI, Hong-wei WANG, Wei WANG, and Ying ZHANG performed the research: Zhi-fang YANG, Hong-wei WANG, Ci-zhen LI, and Ying-min CHEN analyzed the data; Hong-wei Wang and Yuan-mou LIU wrote the paper.
References
Zhang BH, Wang NS, Li XJ, Kong XJ, Cai YL . Anti-arrhythmic effects of matrine. Acta Pharmacol Sin 1990; 11: 253–7.
Huang CY, Xie SR, Huang SY, Gao GY . Experimental studies of anti-arrhythmic effects of matrine. J Dalian Med Univ 2002; 24: 177–9.
Chen YM, Xu J, Li HB, Chen MF, Qian FR, Chen SX, et al. Effect of sophocarpine on ouabain-induced arrhythmia in guinea pigs. Chin J New Drugs Clin Rem 2008; 27: 576–8.
Zhang XY, Chen SX, Liu JX, Qian FR . Protection of cardiomyocytes from coxsackievirus B3 by sophocarpine. Chin J New Drugs Clin Rem 2006; 25: 709–12.
Chen SX, Chen MF, Qian FR, Xie LS . A clinical research of sophocarpine in treatment of viral myocarditis. Chin J Clin Cardiol 2005; 211: 608–11.
Chen YM, Xu J, Ye Q, Chen MF, Shen HF, Chen SX . Effect of sophocarpine in raising ventricular fibrillation threshold and prolonging ventricular effective refractory period of early acute myocardial ischemia in canine. Chin J New Drugs Clin Rem 2006; 25: 252–5.
Wang HW, Yang ZF, Zhang Y, Yang JM, Liu YM, Li CZ . Beta-receptor activation increases sodium current in guinea pig heart. Acta Pharmacol Sin 2009; 30: 1115–22.
Baetz D, Regula KM, Ens K, Shaw J, Kothari S, Yurkova N, et al. Nuclear factor kappaB-mediated cell survival involves transcriptional silencing of the mitochondrial death gene BNIP3 in ventricular myocytes. Circulation 2005; 112: 3777–85.
Zhang Y, Zheng YQ, Wang HW . Yang Zf, Liu YM, Li CZ. Method for culturing neonatal rat cardiac myocytes and observation of its electrophysiological properties. J Shanghai Jiaotong Univ (Med Sci) 2007; 27: 398–400.
Yang ZF, Wang HW, Zheng YQ, Zhang Y, Liu YM, Li CZ . Possible arrhythmiogenic mechanism produced by ibuprofen1. Acta Pharmacol Sin 2008; 29: 421–9.
Liu YM, DeFelice LJ, Mazzanti M . Na channels that remain open throughout the cardiac action potential plateau. Biophys J 1992; 63: 654–62.
Liu YM, Yu H, Li CZ, Cohen IS, Vassalle M . Cesium effects on If and Ik in rabbit sinoatrial node myocytes: implications for SA node automaticity. J Cardiovasc Pharmacol 1998; 32: 783–90.
Li CZ, Liu YM, Yang ZF, Wang HW, Yang JM . An improved method of isolation of rabbit sinus node cells and the perforated patch recording with amphotericin B. Chin J Appl Physiol 1999; 15: 89–92.
Ding WG, Toyoda F, Mastsuura H . Blocking action of chromanol 293B on the slow component of delayed rectifier K+ current in guinea-pig sino-atrial node cells. Br J Pharmacol 2002; 137: 253–62.
Roukoz H, Saliba W . Dofetilide: a new class III anti-arrhythmic agent. Expert Rev Cardiovasc Ther 2007; 5: 9–19.
Qi ZP, Shi SS, Zhao XL, Zhao WX, Bai YL, Lu YJ, et al. Effect of Sophocarpine on HERG K+ Channels. Yao Xue Xue Bao 2008; 43: 44–9.
Katz AM . The Cardiac Action Potential. In: Kartz AM, editors. Physiology of the heart 3rd ed. Philadelphia: Lippincott Williams & Wilkins 2001: P 478–516.
Valenzuela C, Bennett PB . Voltage-and use-dependent modulation of calcium channel current in guinea pig ventricular cells by amiodarone and des-oxo-amiodarone. J Cardiovasc Pharmacol 1991; 17: 894–902.
Desantiago J, Ai X, Islam M, Acuna G, Ziolo MT, Bers DM, et al. Arrhythmogenic effects of β2-adrenergic stimulation in the failing heart are due to enhanced SR Ca load. Circ Res 2008; 102: 1389–97.
Tosaki A, Woodward B, Yamamoto F, Hearse DJ . Isoproterenol and the genesis of reperfusion-induced arrhythmias in isolated rat heart: adrenoceptor or free radical-mediated mechanisms? J Cardiovasc Pharmacol 1990; 15: 398–407.
Tosaki A, Braquet P . DMPO and reperfusion injury: Arrhythmia, heart function, electron spin resonance, and nuclear magnetic resonance studies in isolated working guinea pig hearts. Am Heart J 1990; 120: 819–30.
Tosaki A, Balint S, Szekeres L . Protective effect of lidocaine against ischemia and reperfusion-induced arrhythmias and shifts of myocardial sodium, potassium, and calcium content. J Cardiovasc Pharmacol 1988; 12: 621–8.
Katz AM . Arrhythmias II: Clinical Manifestations and Principles of Therapy. In: Katz AM, editors. Physiology of the heart 3rd ed. Philadelphia: Lippincott Williams & Wilkins 2001: P 580–629.
Tosaki A, Balint S, Szekeres L . Pacing and reperfusion induced arrhythmias: protection by slow heart rate in the rat heart. Cardiovasc Res 1988; 22: 818–25.
Weiss J, Shine KI . Effect of heart rate on extracellular K+ accumulation during myocardial ischemia. AM J Physiol 1986; 250: H982–91.
Zuanetti G, DeFerrari GM, Priori SG, Schwartz PJ . Protective effect of vagal stimulation on reperfusion arrhythmias in cats. Circ Res 1987; 61: 429–35.
Chen SX, Xu XH, Zhang DQ, Mei SW, Xie LS, Chen MF, et al. The study on the expression of IFN-γ and IL-10 in patients with viral myocarditis and their interference with Chinese drugs. Chin J Endocrinol Metab 2001; 21: 14–7.
Zhao XJ, Guo DL, Wu Y, Liu TX, Yan GX . Effects of chronic amiodarone therapy on L-type calcium current recovery and action potential duration of rabbit ventricular myocytes. Chin J Cardiol 2009; 37: 528–31.
Singh BN . Expanding indications for the use of class III agents in patients at high risk for sudden death. J Cardiovasc Electr 1995; 6: 887–900.
Anderson JL . Contemporary clinical trials in ventricular tachycardia and fibrillation: implications of ESVEM, CASCADE, and CASH for clinical management. J Cardiovasc Electr 1995; 6: 880–6.
Vassallo P, Trohman RG . Prescribing amiodarone an evidence-based review of clinical indications. J Am Med Assoc 2007; 298: 1312–22.
Sicouri S, Belardinelli L, Carlsson L, Antzelevitch C . Potent antiarrhythmic effects of chronic amiodarone in canine pulmonary vein sleeve preparations. J Cardiovasc Electr 2009; 20: 803–10.
Kodama I, Kamiya K, Toyama J . Amiodarone: Ionic and cellular mechanisms of action of the most promising class III agent. Am J Cardiol 1999; 9: 20–8.
Singh BN . Amiodarone: A multifaceted antiarrhythmic drug. Curr Cardiol Rep 2006; 5: 349–55.
Li XL, Chu WM, Liu JL, Xue XR, Lu YJ, Shan HL, et al. Antiarrhythmic properties of long-term treatment with Matrine in arrhythmic rat induced by coronary ligation. Biol Pharm Bull 2009; 32: 1521–6.
Acknowledgements
This work was supported by the Science Foundation of the Shanghai Science Committee Foundation (No 06JC14045) and the Science Foundation of Shanghai Health Bureau (No 2009045).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yang, Zf., Li, Cz., Wang, W. et al. Electrophysiological mechanisms of sophocarpine as a potential antiarrhythmic agent. Acta Pharmacol Sin 32, 311–320 (2011). https://doi.org/10.1038/aps.2010.207
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/aps.2010.207
Keywords
This article is cited by
-
New antiarrhythmic targets to control intracellular calcium handling
Netherlands Heart Journal (2014)
-
New 12-N-β-Hydroxyethylcytisine Derivatives with Potential Antiarrhythmic Activity
Chemistry of Natural Compounds (2014)
