
Abstract
OBJECTIVE:
The most common admission to intensive care nurseries is the infant with suspected neonatal sepsis. To determine the clinical practice of neonatologists with respect to this diagnosis, we examined a large neonatal database during a 2-year period of time. The goal of this study was to define whether there were optimal practice strategies that could identify a “benchmark” clinical approach for this diagnosis.
DESIGN:
The PROACT© database of ParadigmHealth was examined for all term infants with an admitting ICD – 9 code for suspected neonatal sepsis between January 1, 2001 and December 31, 2002. Infants had to be asymptomatic by 24 hours of life with no significant respiratory signs and receiving oral feedings. All infants had negative blood cultures. Maternal risk factors were examined to determine if they influenced the duration of therapy. The impact of treatment upon subsequent length of stay was also evaluated. Several areas of the country were individually examined to see if possible regional variations existed with respect to treatment of suspected sepsis.
RESULTS:
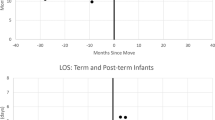
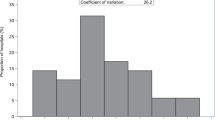
There were no significant differences noted in the management when maternal risk factors for suspected sepsis were assessed. In general, neonates were treated for 3.3±1.8 to 3.5±2.1 days, regardless of the number of maternal risk factors present at birth (p=NS). Length of stay ranged from 4.2±2.1 to 4.4±1.9 days in these groups (p=NS). The duration of treatment ranged from 1 to 10 days, even though all infants were clinically well and feeding by 24 hours of life. A total of 170 infants (17.0%) were treated for 4 to 6 days and 116 (11.6%) neonates received antibiotics for 7 to 10 days, even with negative blood cultures. One region of the country appeared to treat infants for a longer period of time than the other four regions examined, increasing the mean length of stay by 1.8 days (p<0.05).
CONCLUSIONS:
Treatment of neonates with suspected sepsis appears to be influenced by considerations other than maternal risk factors or the infant's clinical condition beyond the first day of life. There appears to be a great deal of practice variation among neonatologists confronted by patients with suspected sepsis. Awareness of this unnecessary variation may be of great value in reducing the duration of antibiotic therapy in the NICU and shortening the length of stay.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
ParadigmHealth Management Services database, 2003.
Prevention of Perinatal Group B Streptococcal Disease. Revised Guidelines from CDC. MMWR 2002;51(RR11):1–22.
Touch SM, Greenspan JS, Kornhauser MS, Spitzer AR . Intensive care management of the term neonate: are there regional differences in outcome? Clini Pediatr 2002;41:587–592.
Touch SM, Greenspan JS, Kornhauser MS, O'Connor JP, Nash DB, Spitzer AR . The timing of neonatal discharge: an unwanted variation? Pediatrics 2001;107:73–77.
Garcia-Prats JA, Cooper TR, Schneider VF, et al. Rapid detection of microorganisms in blood cultures of newborn infants utilizing an automated blood culture system. Pediatrics 2000;105:523–527.
Kumar Y, Qunibi M, Neal TJ, Yoxall CW . Time to positivity of neonatal blood cultures. Arch Dis Child Fetal Neonatal Ed 2001;85:F182–F186.
Sarkar S, Bhagat I, Mele P, et al. A prospective trial of the role of multiple site blood cultures in the initial evaluation of neonatal sepsis. Pediatric Res 2003;53:442A.
Schelonka RL, Yoder BA, desJardins SE, Capt., et al. Peripheral leukocyte count and leukocyte indexes in healthy newborn term infants. J Pediatr 1994;125:603–606.
Kocherlakota P, La Gamma EF . Preliminary report: rhG-CSF may reduce the incidence of neonatal sepsis in prolonged preeclampsia-associated neutropenia. Pediatrics 1998;102:1107–1111.
Fagoaga OR, Nehlsen-Cannarella SL . Maternal modulation of neonatal immune system development. Dev Immunol 2002;9:9–17.
Goetzl L, Evans T, Rivers J, et al. Elevated maternal and fetal serum interleukin-6 levels are associated with epidural fever. Am J Obstet Gynecol 2002;187:834–838.
Bauer J, Hentschel R, Linderkamp O . Effect of sepsis syndrome on neonatal oxygen consumption and energy expenditure. Pediatrics 2002;110:e69.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Spitzer, A., Kirkby, S. & Kornhauser, M. Practice Variation in Suspected Neonatal Sepsis: A Costly Problem in Neonatal Intensive Care. J Perinatol 25, 265–269 (2005). https://doi.org/10.1038/sj.jp.7211252
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7211252
