
Abstract
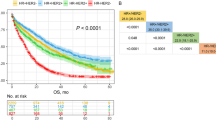
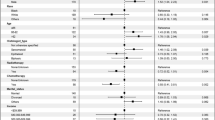
Surgical treatment of lung metastases from melanoma is highly controversial as the expected outcome is much poorer than for other primary tumours and a reliable system for selecting patients is lacking. This study evaluated the long-term results of lung metastasectomy for melanoma, with the aim of defining a subset of patients with better prognosis. By reviewing the data of the International Registry of Lung Metastases (IRLM), we identified 328 patients who underwent lung metastasectomy for melanoma in the period 1945–1995. Survival was calculated by Kaplan–Meier estimate, using log-rank test and Cox regression model for statistical analysis. After complete pulmonary metastasectomy (282 patients) the 5- and 10-year survival was 22% and 16%, respectively. In this group of patients, a time to pulmonary metastases (TPM) shorter than 36 months or the presence of multiple metastases were independent unfavourable prognostic factors. There were no long-term survivors after incomplete resection (46 patients, P< 0.01). Using the IRLM grouping system, patients without risk factors (TPM > 36 months and single lesion) experienced the best survival (29% at 5 years), followed by those with one risk factor only (20% at 5 years). On the other hand, those with two risk factors or incomplete resection showed a significantly poorer survival (7% and 0% at 5 years). Surgery plays an important role in carefully selected cases of pulmonary metastatic melanoma. The prognostic grouping system proposed by the International Registry of Lung Metastases provides a simple and effective method for improving the selection of surgical candidates. © 2000 Cancer Research Campaign
Similar content being viewed by others

Article PDF
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Balch CM & Milton GW (1985) Diagnosis of metastatic melanoma at distant sites. In Cutaneous melanoma: clinical management and treatment results worldwide, Balch CM, Milton GW (eds) pp 221. Philadelphia: Lippincott
Cahan WG (1973) Excision of melanoma metastases to lung: problems in diagnosis and management. Ann Surg 178: 703–709
Falkson CI, Ibrahim J, Kirkwood JM, Coates AS, Atkins MB & Blum RH (1998) Phase III trial of dacarbazine with interferon alpha-2b versus dacarbazine with tamoxifen versus dacarbazine with interferon alpha-2b and tamoxifen in patients with metastatic malignant melanoma: an Eastern Cooperative Oncology Group study. J Clin Oncol 16: 1743–1751
Fletcher WS, Pommier RF, Lum S & Wilmarth TJ (1998) Surgical treatment of metastatic melanoma. Am J Surg 175: 413–417
Gorenstein LA, Putnam JB, Natarajan,, Balch CA & Roth JA (1991) Improved survival after resection of pulmonary metastases from malignant melanoma. Ann Thorac Surg 52: 204–210
Harpole DH, Johnson CM, Wolfe WG, George SL & Seigler HF (1992) Analysis of 945 cases of pulmonary metastatic melanoma. J Thorac Cardiovasc Surg 103: 743–750
Holder WD, White RL, Zuger JH, Easton EJ & Greene FL (1998) Effectiveness of positron emission tomography for the detection of melanoma metastases. Ann Surg 227: 764–771
Karakousis CP, Velez A, Driscoll DL & Takita H (1994) Metastasectomy in malignant melanoma. Surgery 115: 295–302
Ketcham AS & Balch CM (1985) Classification and staging system. In Cutaneous melanoma: clinical management and treatment results worldwide, Balch CM, Milton GW (eds) pp 55–62, Philadelphia: Lippincott
Mathisen DJ, Flye MW & Peabody J (1979) The role of thoracotomy in the management of pulmonary metastases from malignant melanoma. Ann Thorac Surg 27: 295–299
Mountain CF, McMuntrey MJ & Hermes KE (1984) Surgery for pulmonary metastasis: a 20 years experience. Ann Thorac Surg 38: 323–330
Olilla DW, Stern SL & Morton DL (1998) Tumour doubling time: a selection factor for pulmonary resection of metastatic melanoma. J Surg Oncol 69: 206–211
Pastorino U, Buyse M, Friedel G, Ginsberg RJ, Girard P, Goldstraw P, Johnston M, McCormack P, Pass H & Putnam JB (1997) Long-term results of lung metastasectomy: prognostic analysis based on 5206 cases. J Thorac Cardiovasc Surg 113: 37–49
Pogrebniak HW, Stovroff M, Roth JA & Pass HI (1988) Resection of pulmonary metastases from malignant melanoma: results of 16-years experience. Ann Thorac Surg 46: 20–23
Slingluff CL, Dodge RK, Stanley WE & Seigler HF (1992) The annual risk of melanoma progression. Cancer 70: 1917–1927
Tafra L, Dale PS, Wanek LA, Ramming KP & Morton DL (1995) Resection and adjuvant immunotherapy for melanoma metastatic to the lung and thorax. J Thorac Cardiovasc Surg 110: 119–128
Thayer JO & Overholt RH (1985) Metastatic melanoma to the lung: long term results of surgical excision. Am J Surg 149: 558–562
Wong JH, Skinner KA, Kim KA, Foshag LJ & Morton DL (1993) The role of surgery in the treatment of nonregionally recurrent melanoma. Surgery 113: 389–394
Author information
Authors and Affiliations
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Leo, F., Cagini, L., Rocmans, P. et al. Lung metastases from melanoma: when is surgical treatment warranted?. Br J Cancer 83, 569–572 (2000). https://doi.org/10.1054/bjoc.2000.1335
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1054/bjoc.2000.1335
Keywords
This article is cited by
-
Apelin promotes blood and lymph vessel formation and the growth of melanoma lung metastasis
Scientific Reports (2021)
-
Chirurgische Therapie pulmonaler Metastasen des malignen Melanoms
Der Hautarzt (2015)
-
Maligne Melanome im Kopf-Hals-Bereich
HNO (2015)
