
Abstract
Oral cancer incidence was investigated among 10 857 individuals using Scottish Cancer Registry data. Since 1980 the incidence of oral cancer among males in Scotland has significantly increased, the rise occurring almost entirely in the most deprived areas of residence.
Similar content being viewed by others
Main
Incidence of oral and oro-pharyngeal cancer continues to rise across the UK in all age groups and in both sexes (Conway et al, 2006). Oral cancer risk appears highly correlated with socio-economic factors, both in Scotland (Macfarlane et al, 1996) and in the UK (Edwards and Jones, 1999), although this was not reflected in a review of incidence studies across the world (Faggiano et al, 1997). Studies of the socio-economic association with oral cancer tend to be cross-sectional and cannot account for temporal changes (Greenwood et al, 2003; Møller and Brewster, 2005). One recent case–control study in Italy, which examined time –trends, found that oral cancer risk associated with poor socio-economic circumstances had disappeared through the 1990s (Bosetti et al, 2001). The aims of this study were to assess the pattern, magnitude, and time trends of socio-economic inequalities in the distribution of oral cancer in Scotland.
Materials and methods
Incident cases of oral cancers (ICD-10 C00-C06) and cancers of the oro-pharynx (C09, C10, and C14) for the period 1976–2002 were obtained from the Scottish Cancer Registry, which has a high level of case ascertainment (Brewster et al, 1997) and accuracy of postcodes, from which the Carstairs scores were derived (see below) (Brewster et al, 2002). Mid-year population estimates were derived from the Annual Reports of the Registrar General for Scotland for corresponding years (General Register Office for Scotland, 1977–2003). Annual and triennial age-standardised incidence rates by sex were calculated for the period 1977–2002 by direct standardisation to the European Standard Population (Waterhouse et al, 1976).
This study utilises the area-based (postcode sector) Carstairs index of deprivation, which comprises four variables from the UK decennial census: social class, unemployment, overcrowding, and car ownership (Carstairs and Morris, 1991). First, 1981, 1991, and 2001 Carstairs deprivation categories were linked with cancer registration data relating to the periods of diagnosis 1976–1985, 1986–1995, and 1996–2002, respectively. Second, to validate this approach, the 1991 census-derived Carstairs deprivation categories were applied to the whole period of diagnosis 1976–2002. There were no substantial differences observed between the two methods; therefore, only data from our first method are reported here.
Poisson regression models were used to assess the magnitude of change and significance of trends in incidence. The independent effects were analysed in a fully adjusted model, and interactions were also examined. Statistical analyses were performed on SAS version 9.1 (SAS Institute Inc.).
Results
Overall incidence of oral cancer for males was 11.1 per 100 000 (95% confidence interval 10.8, 11.3) and for females was 4.1 per 100 000 (3.9, 4.2). Incidence increased significantly in both males (+87%, P<0.001) and females (+65%, P<0.001) over the period of the study. Comparing the 3-year periods at the start and end of the period, incidence in males increased from 10.1 (10.8, 11.3) to 13.3 (12.5, 14.1) per 100,000 and in females from 2.8 (2.5, 3.2) to 5.5 (5.0, 6.0) per 100 000. The median age of diagnosis was 65.1 years.
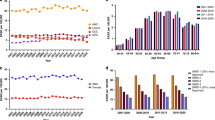
Between 1976 and 2002, the widening gaps in oral cancer incidence between affluent and deprived socio-economic groups by sex are clearly demonstrated in Figure 1 and Table 1. For males there was a general increase in incidence of oral cancer with increasing severity of deprivation. From an inverse relationship in 1976–1978, the gap between the most and least deprived males appeared in the late 1970s and increased rapidly through to the 1990s. The gap is almost entirely explained by an increase in incidence (+196%, P<0.001) in the most deprived, with a (nonsignificant) reduction in the least deprived group over the period (−74%, P=0.54). A different pattern is seen for females in both magnitude and timing. The incidence increased in those from all levels of deprivation, with those women from the most deprived areas having the greatest increase (+163%, P<0.001), but a significant increase also apparent in the least deprived (+91%, P<0.001). The widening gap between the most and least deprived appeared in the 1980s and continued to increase until the late 1990s. Data from 2000 to 2002 suggest that the gap had closed for women over 65 years.

Males and females European age-standardised incidence rate (EASR) of oral and oro-pharyngeal cancer by Carstairs deprivation least and most deprived quintiles 1976–2002 in Scotland.
Discussion
Our study shows that oral cancer incidence has increased from the 1970s to present, with corresponding widening socio-economic inequalities, particularly in males. During this period, societal changes have included post-industrial decline bringing unemployment and polarisation of poverty to the parts of Scotland (Devine and Finlay, 1996), where oral cancer is commonest.
The interaction between socio-economic life circumstances and behaviour is complex. These circumstances can affect knowledge of and ability to make healthy choices (Evans and Stoddart, 1994). Smoking (Stead et al, 2001) and alcohol consumption (Marmot, 1997) have been regarded as coping mechanisms for the stress associated with deprivation. It is also well documented that diet is related to access and affordability of healthy foods and not simply a lifestyle choice (Wrigley, 2002).
The important known ‘lifestyle’ factors for oral cancer are smoking (Blot et al, 1988) and alcohol consumption (Bagnardi et al, 2001), which, importantly for oral cancer, together also have a synergistic effect (Macfarlane et al, 1995). A diet low in fresh fruit and vegetables (Pavia et al, 2006) has also been found to be associated with increased oral cancer risk. The question is to what extent can the trends in oral cancer inequality be explained by socio-economic variation in these risk factors.
Data on smoking prevalence from 1972 show a consistent downward trend in all social classes in both sexes across Britain. Although smoking remained substantially lower in the higher social classes, widening inequalities were not obvious (Goddard and Green, 2005). More recent Scottish data (1995–2003) indicate that the downward trend in smoking prevalence continues with increasing inequalities in its distribution–with those from deprived areas increasingly less likely to give up (Bromley et al, 2005). Oral cancer risk markedly declines after quitting smoking (La Vecchia et al, 1999). Overall, the patterns in smoking behaviour cannot easily explain the widening socio-economic inequalities in oral cancer incidence.
The association between alcohol drinking in Scotland and socio-economic factors is somewhat mixed. The Scottish Health Survey 1995–2003 (Bromley et al, 2005) consistently shows that more people were drinking alcohol excessively, irrespective of their socio-economic circumstances. Similar findings in Britain from the 1980s were reported (Goddard and Green, 2005). However, between 1998 and 2003 there was a 19% rise in alcohol-related hospital episodes in Scotland with a strong relationship to area deprivation (Bromley et al, 2005). Thus, alcohol may have a role in socio-economic inequalities in oral cancer, although the evidence is incomplete. In our study, we were unable to investigate the well-documented synergistic effects of smoking and heavy drinking.
Daily fruit and vegetable consumption has significantly increased in Scotland (1995–2003), although those from deprived areas were eating less than their affluent counterparts (Bromley et al, 2005). Earlier UK data have highlighted similar trends among unemployed individuals (Braddon et al, 1988). However, owing to the absence of long-term dietary behaviour data, strong conclusions cannot be drawn.
The effects of socio-economic circumstances per se are worth considering. Although area measures of socioeconomic status have previously been criticised as ‘ecological fallacy’ – individuals are allocated a status based on their residence – this may in fact help with an explanation. People in the same area sharing many socio-economic circumstances may also experience some additional collective ‘stresses’ (Macintyre et al, 1993). Hypotheses of ‘biological ageing’ effects of poor socio-economic circumstances may be relevant (Adams and White, 2004), perhaps being mediated by telomere shortening (Cawthon et al, 2003).
Explanations for the widening inequality trends are complex. More work is required to explain the continuing rise in oral cancer incidence and the increasing socioeconomic inequalities, and public health programmes for early detection and prevention of oral cancer need to be developed by working with deprived communities.
Explanations for the widening inequality trends are complex. More work is required to explain the continuing rise in oral cancer incidence and the increasing socio-economic inequalities. Public health programmes for the early detection and prevention of oral cancer are needed in deprived communities. Although the association with socio-economic factors is well known, little has been done to explicitly address this. To date, ‘high-risk groups’ have primarily been defined by their sex, age, smoking and alcohol behaviours (Speight et al, 2006). Those living in deprived areas should be considered as the key ‘priority risk group’. Policy needs to be directed towards tackling root causes of disadvantage, as efforts to reduce exposure to risk factors are unlikely to succeed unless they are supported by measures designed to improve socio-economic circumstances.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Adams JM, White M (2004) Biological ageing. Eur J Pub Health 14: 331–334, doi:10.1093/eurpub/14.3.331
Bagnardi V, Blangiardo M, La Vecchia C, Corrao G (2001) A meta-analysis of alcohol drinking and cancer risk. Br J Cancer 85: 1700–1705, doi:10.1054/bjoc.2001.2140
Blot WJ, McLaughlin JK, Winn DM, Austin DF, Greenberg RS, Preston-Martin S, Bernstein L, Schoenberg JB, Stemhagen A, Fraumeni Jr JF (1988) Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res 48: 3282–3287
Bosetti C, Fanceschi S, Negri E, Talamini R, Tomei F, La Vecchia C (2001) Changing socioeconomic correlates for cancers of the upper digestive tract. Ann Oncol 12: 327–330
Braddon FEM., Wadsworth MEJ, Davies JMC, Cripps HA (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort. J Epidemiol Commun Health 42: 341–349
Brewster DH, Crichton J, Harvey JC, Dawson G (1997) Completeness of case ascertainment in a Scottish regional cancer registry for the year 1992. Public Health 111: 339–343
Brewster DH, Stockton D, Harvey J, Mackay M (2002) Reliability of cancer registration data in Scotland, 1997. Eur J Cancer 38: 414–417, doi:10.1016/S0959-8049(01)00385-9
Bromley C, Sproston K, Shelton N (2005) Scottish Health Survey 2003. Edinburgh: The Stationery Office http://www.scotland.gov.uk/Publications/2005/11/25145024/50251 (accessed November 2006)
Carstairs V, Morris R (1991) Deprivation and Health in Scotland. Aberdeen: Aberdeen University Press
Cawthon RM, Smith KR, O’Brien E, Sivatchenko A, Kerber RA (2003) Association between telomere length in blood and mortality in people aged 60 years or older. Lancet 361: 393–395, doi:10.1016/S0140-6736(03)12384-7
Conway DI, Stockton DL, Warnakulasuriya KAAS, Ogden G, Macpherson LMD (2006) Incidence of oral and oro-pharyngeal cancer in United Kingdom (1990–1999) – recent trends and regional variation. Oral Oncol 42: 586–592, doi:10.1016/j.oraloncology.2005.10.018
Devine TM, Finlay RJ (1996) Scotland in the 20th Century. Edinburgh: Edinburgh University Press
Edwards DM, Jones J (1999) Incidence of and survival from upper aerodigestive tract cancers in the UK: the influence of deprivation. Eur J Cancer 35: 968–972, doi:10.1016/S0959-8049(99)00095-7
Evans RG, Stoddart GL (1994) Producing health, consuming health care. In Why are Some People Healthy and Others are not? Evans RG, Barer ML, Marmot TR (eds) pp 27–64. New York: Walter de Gruyter
Faggiano F, Partanen T, Kogevinas M, Boffetta P (1997) Socio-economic differences in cancer incidence and mortality. In Social Inequalities and Cancer Kogevinas M, Pearce N, Susser M, Boffetta P (eds) pp 65 IARC Scientific Publication No. 138. Lyon: International Agency for Research on Cancer
General Register Office for Scotland (1977–2003) Annual Reports 1977–2003. Edinburgh: General Register Office for Scotland
Goddard E, Green H (2005) Smoking and drinking among adults, 2004. General Household Survey, 2004. London: Office for National Statistics
Greenwood M, Thomson PJ, Lowry RJ, Steen IN (2003) Oral cancer: material deprivation, unemployment and risk factor behaviour – an initial study. Int J Oral Maxillofac Surg 32: 74–77, doi:10.1054/ijom.2002.0274
La Vecchia C, Franceschi S, Bosetti C, Levi F, Talamini R, Negri E (1999) Time since stopping smoking and the risk of oral and pharyngeal cancers. J Natl Cancer Inst 91: 726–728
Macfarlane GF, Zheng T, Marshall JR, Boffeta P, Niu S, Brasure J, Merletti F, Boyle P (1995) Alcohol, tobacco, diet and the risk of oral cancer: a pooled analysis of three case–control studies. Eur J Cancer B Oral Oncol 50: 6502–6507
Macfarlane GJ, Sharp L, Porter S, Franceschi S (1996) Trends in survival from cancers of the oral cavity and pharynx in Scotland: a clue as to why the disease is becoming more common? Br J Cancer 73: 805–808
Macintyre S, MacIver S, Sooman A (1993) Area, class and health: should we be focusing on places or people? J Soc Pol 22: 213–234
Marmot M (1997) Inequality, deprivation and alcohol use. Addiction 92: S13–S20, doi: 10.1111/j.1360-0443.1997.tb03391.x
Møller H, Brewster DH (2005) Lip, mouth and pharynx. In Cancer Atlas of the United Kingdom and Ireland 1991–2000 Quinn M, Wood H, Cooper N, Rowan S (eds) pp 129–138, Studies on Medical and Population Subjects No. 68. Basingstoke: Palgrave Macmillan
Pavia M, Pileggi C, Nobile CGA, Angelillo IF (2006) Association between fruit and vegetable consumption and oral cancer: a meta-analysis of observational studies. Am J Clin Nutr 83: 1126–1134
Speight PM, Palmer S, Moles DR, Downer MC, Smith DH, Henriksson M, Augustovki F (2006) The cost-effectiveness of screening for oral cancer in primary care. Health Technology Assessment 10 (14) www.ncchta.org/projectdata/1_project_record_published.asp?PjtId=1214&SearchText=oral+cancer (accessed February 2007)
Stead M, MacAskill S, MacKintosh AM, Reece J, Eadie D (2001) It's as if you’re locked in’: qualitative explanations for area effects on smoking in disadvantaged communities. Health Place 7: 333–343, doi:10.1016/S1353-8292(01)00025-9
Waterhouse J, Muir C, Cornea P, Powell J (1976) Cancer Incidence in Five Continents Vol III, pp 454–459. Lyon: International Agency for Research on Cancer
Wrigley N (2002) Food deserts in British cities: policy context and research priorities. Urban Stud 39: 2029–2040, doi:10.1080/0042098022000011344
Acknowledgements
We thank Andrew Duffy, ISD, for extracting the data and all those who contributed to the Scottish Cancer Registry.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Conway, D., Brewster, D., McKinney, P. et al. Widening socio-economic inequalities in oral cancer incidence in Scotland, 1976–2002. Br J Cancer 96, 818–820 (2007). https://doi.org/10.1038/sj.bjc.6603621
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6603621
