
Abstract
Data sources
Medline, Cochrane Library, Web of Science, Scopus, Latin American and Caribbean Health Sciences (LILACS), Brazilian Library of Dentistry (BBO), clinicaltrials.gov and SIGLE databases.
Study selection
Only randomised clinical trials were considered that compared direct vs indirect composite restorations, with or without cusp involvement, having a follow-up period of two years or greater.
Data extraction and synthesis
Two reviewers selected studies for inclusion, abstracted data and assessed risk of bias. A fixed effects meta-analysis was conducted.
Results
Nine studies met the inclusion criteria with six contributing to the meta-analysis. There was no statistically significant difference in clinical longevity for direct and indirect resin composite restorations; relative risk (RR) = 1.494 (95% CI; 0.893–2.500, p = 0.126). Comparing molars and premolars restored with DRC and IRC at three years there was no significant difference; RR = 0.716 (95% CI; 0.177–2.888, p = 0.638).
Conclusions
The results of the review indicate that there is no statistically significant difference in failure rate of direct resin composites vs indirect resin composites. Longitudinal studies on today's improved materials should, however, be considered for further review.
Similar content being viewed by others

Commentary
In everyday practice, dentists must make treatment choice recommendations with the patients' best interests in mind. With the improvements seen over the past decade or more, restorative materials and treatment option advancements have been made. Bonded restorations offer excellent functional capability and endurance and have the added advantage of being aesthetically pleasing as well as metal free. Advising patients on restorative choices may at times seem daunting. In medium to large cavities, we tend to expect that an indirect resin composite may be a superior choice, offering patients long-term success and viability. However, is this truly the case?
The objective of this systematic review and meta-analysis is to answer this question. Is there a difference in clinical longevity between direct vs indirect composite restorations? The primary outcome was to evaluate the failure rate of direct and indirect composite restorations in posterior teeth. The secondary outcome explored failure rates in subgroups which consisted of direct vs indirect resin composites, direct vs direct inlay/onlay composite restorations, and clinical effects of bruxism and caries on failure rate of direct vs indirect composite restorations.
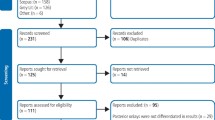
The review authors selected only RCT papers that considered longevity of direct vs indirect restorations with or without involvement of cusps. There were no restrictions on language, setting or year of publication. Eligibility criteria were verified by a pilot test, conducted on a sample study. Low risk studies were used and included in meta-analysis by use of the Comprehensive Meta-Analysis software and the Collaboration's tool for assessing bias in RCTs. Four key domains were considered; sequence generation, allocation of concealment, incomplete outcome data and selective outcome reporting.
A meta-analysis was conducted for five-year follow-up studies comparing DRC to IRC. Low heterogeneity was reported (I2 = 4.09%) and RR (1.494) for indirect restorations. No statistically significant difference in longevity was found in the pooled meta-analysis (p = 0.126).
In a subgroup analysis, of DRC vs IRC at five-year follow-up, the RR was (1.278) in relation to IRC. No statistically significant difference was shown, (p = 0.464), and low heterogeneity was reported. A second subgroup meta-analysis of DRC vs DIO at five-year follow-up showed no statistically significant difference. RR (1.915), and (P = 0.124) in relation to DIO. There was no heterogeneity between groups, (I2 = 0.00%)
A pooled meta-analysis of DRC vs IRC at three years showed low heterogeneity (I2 = 25.03%) for molars and (I2 = 0.00%) for premolars.
Relative risk of 0.716 and no statistically significant difference, with (p = 0.638).
Potential problems with the studies reviewed are that lack of clarity was reported by the review authors with sequence generation and allocation concealment. In order to help resolve these problems, the study authors were emailed. These issues were not addressed in the methodology of the RCTs. Another point to consider is that the materials used in the studies no longer exist and many new and improved materials have since been developed. Consideration of further longitudinal studies is needed and should be implemented.
Although further research can be beneficial, the results from this review are well established in their delivery of scientific evidence. Since they show no statistically significant difference in longevity and failure rates, why not offer patients this less expensive, comparably acceptable treatment option?
Author information
Authors and Affiliations
Additional information
Address for correspondence: Lucianne Cople Maia, Disciplina de Odontopediatria da FO-UFRJ, caixa postal 68066, CEP: 21941-971, Cidade Universitária, Rio de Janeiro, RJ, Brazil. E-mail: rorefa@terra.com.br
da Veiga AM, Cunha AC, Ferreira DM, da Silva Fidalgo TK, Chianca TK, Reis KR, Maia LC. Longevity of direct and indirect resin composite restorations in permanent posterior teeth: A systematic review and meta-analysis. J Dent 2016; 54: 1–12. pii: S0300-5712(16)30160-9. doi: 10.1016/j.jdent.2016.08.003. [Epub ahead of print] Review. PubMed PMID: 27523636.
Rights and permissions
About this article

Cite this article
Congiusta, M. No differences in longevity of direct and indirect composite restorations. Evid Based Dent 18, 46 (2017). https://doi.org/10.1038/sj.ebd.6401237
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401237
