
Abstract
Study design
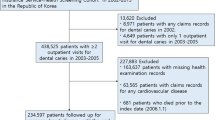
This was a nested case control study within the Oslo study, which began in 1972/73 with the principle aim of studying prevention and epidemiology of cardiovascular diseases.
Intervention
Within the Oslo study, men who attended for examination in both 1972/73 and 2000 with a self-reported history of MI (n=548) were compared to controls (n=625) selected at random from the same cohort, and matched by five-year strata for age.
Outcome measure
Information on history of tooth extractions and the reasons for these extractions were obtained from a self-reported questionnaire. Reasons for tooth extractions were subgrouped into infection (marginal periodontitis and apical infection) or trauma/other causes.
Results
Investigation of the association between the reason for extraction and MI, using prospective logistic analysis, found that extractions attributed to dental infections were significant predictors for risk factors in both 1972/73 and 2000.
Conclusions
There was an increased association between MI and tooth extraction due to dental infection compared with tooth extraction for trauma and other reasons.
Similar content being viewed by others
Commentary
The authors explore the relationship between reasons for dental extractions and the occurrence of non-fatal myocardial infarction (MI) in a large cohort of male patients followed for over 30 years. They hypothesised that the level of bacteraemiap- during dental extractions, in the presence of infection, may have a relation to the occurrence of MI.
Previous studies revealed that bacteraemia levels during dental extractions might not be different from bacteraemia from brushing, especially in patients with periodontal disease.1,2
The case control design used was adequate for a harmful outcome such as MI. Cases (n=548) consisted of patients with a self-reported history of MI. Controls (625) were adequately matched by age. Other characteristics that could play a role as confounders like BMI, cholesterol levels and systolic blood pressure were not matched as well.
The history of tooth extractions and oral infections was elicited by a questionnaire, introducing the potential for recall bias and open issues with interpretation.
Interestingly data collected in 2000 showed no statistical differences in the levels of C-reactive protein between groups, while the evaluation of the current oral condition reported the presence of periodontal infection being double in the control group (50%) that of the study group (24%). Levels of C-reactive protein have been widely used in research to monitor effectiveness of periodontal therapy,3,4and they are also used in the medical field as a risk indicator for MI.5
The time of the MI occurrence was not reported. Neither the timeline between the extractions and the MI nor antibiotic usage were reported. A temporal relationship could not be established. More cases had teeth extracted than controls did (92.7% versus 88.6%) during the study.
The results were presented as odds ratio (OR) with a calculated value of 1.73, with 95% CI: 1.34-2.23 between having extractions attributed to infections and developing an MI.
The authors do not discard the possibility of what they call a ‘common underlying trait’ for oral infections and MI as part as the effect observed.
With the methodological limitations of this observational study, the researchers concluded that the results indicate a strong association between the two entities and clearly point to the presence of the underlying infection as the factor of importance. The authors' conclusions may be limited because we can only guess that the extractions preceded the MI and that the nature of the bacteraemia is significantly different during this study from when brushing or flossing.
Practice points
-
No possible conclusion about the relationship between extractions and MI can be established.
References
Tomás I, Diz P, Tobías A, Scully C . Periodontal health status and bacteraemia from daily oral activities: systematic review/meta-analysis. J Clin Periodontol 2012; 39: 213–228.
Lockhart PB, Brennan MT, Sasser HC, Fox PC, Paster BJ, Bahrani-Mougeot FK . Bacteremia associated with tooth brushing and dental extraction. Circulation, 2008; 117: 3118–3125.
Paraskevas S, Huizinga JD, Loos BG . A systematic review and meta-analyses on C-reactive protein in relation to periodontitis. J Clin Periodontol. 2008; 35: 277–290.
Freitas CO, Gomes-Filho IS, Naves RC, Nogueira Filho Gda R, Cruz SS, Santos CA, et al. Influence of periodontal therapy on C-reactive protein level: a systematic review and meta-analysis. J Appl Oral Sci 2012; 20: 1–8.
Vavuranakis M, Kariori MG, Kalogeras KI, et al. Biomarkers as a guide of medical treatment in cardiovascular diseases. Curr Med Chem 2012; 19: 2485–2489.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Lise Lund Haheim, Institute of Oral Biology, Faculty of Dentistry, University of Oslo, Oslo, Norway. E-mail: a.l.haheim@odont.uio.no
Haheim LL, Olsen I, Ronningen KS. Association between tooth extraction due to infection and myocardial infarction. Community Dent Oral Epidemiol 2011; 39: 393–397.
Rights and permissions
About this article
Cite this article
Spivakovsky, S. Myocardial infarction and tooth extraction associated. Evid Based Dent 13, 110 (2012). https://doi.org/10.1038/sj.ebd.6400894
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400894
This article is cited by
-
Evaluation of cardiac risk in dental patients
British Dental Journal (2018)
