
Abstract
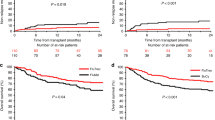
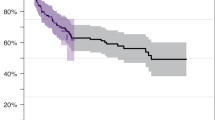
To compare the antileukemic efficacy of idarubicin and mitoxantrone in elderly patients with acute myeloid leukemia (AML) and to evaluate the feasibility of autologous transplantation using PBSC after consolidation in those with a good performance status, 160 patients (median age 69 years), with AML at diagnosis, 118 of them with de novo AML and 42 with AML secondary to myelodysplastic syndrome or toxic exposure (sAML), received induction treatment with idarubicin, 8 mg/m2/day or mitoxantrone, 7 mg/m2/day, on days 1, 3, and 5, both combined with VP-16, 100 mg/m2/day on days 1 to 3 and cytarabine (araC), 100 mg/m2/day, on days 1 to 7. G-CSF, 5 μg/kg/day, was administered after chemotherapy in patients aged more than 70 years. Patients in complete remission (CR) received one course of consolidation using the same schedule as for induction except the araC administration was shortened to 5 days. Some patients younger than 70 years were then scheduled for autologous stem cell harvest on days 5 to 7 of G-CSF, 5 μg/kg/day, initiated after hematopoietic recovery from consolidation. Autologous transplantation was performed following an additional chemotherapy conditioning. Ninety-five patients (59%) achieved CR, without significant difference between the idarubicin (56% CR) and mitoxantrone (63% CR) group. There was also no significant difference in CR rate between de novo AML (63%) and secondary AML (55%) (P = 0.12). Patients aged < 70 years had 67% cr, while patients aged ≥ 70 years had 49% (P = 0.02). There was no significant difference in the duration of aplasia between the two arms. Median time to neutrophil recovery was 22 days in patients who received G-CSF following induction and 27 days in patients who did not (P = 0.006). Severe extra-hematologic toxicities of induction did not differ between the two arms and included sepsis (39%), diarrhea (13%), hyperbilirubinemia (8%), hemorrhage (6%) and vomiting (6%). Overall, 14 patients (9%), died from toxicity of induction. First consolidation was administered in 74 patients of whom seven (9%) died from toxicity. Nineteen patients have received transplantation. Median time to recovery of neutrophils >0.5 × 109/1 was 13 days and of platelets >50 × 109/l 43 days following consolidation. There were two toxic deaths. Median disease-free survival and survival from time of achieving CR of non transplanted patients are 6 and 7 months respectively without difference between the two arms. Fourteen transplanted patients relapsed at a median of 5 months post-transplant. We conclude that this regimen is well tolerated and has a good efficacy to induce CR, without a significant difference in efficacy and toxicity between idarubicin and mitoxantrone. Intensive postinduction, including transplantation, is feasible; however, this procedure did not seem to prevent early relapse in the majority of patients. Neither the high rate of CR nor consolidation nor transplant procedure in a selected group of patients did translate into improved DFS and/or survival.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Archimbaud, E., Jehn, U., Thomas, X. et al. Multicenter randomized phase II trial of idarubicin vs mitoxantrone, combined with VP-16 and cytarabine for induction/consolidation therapy, followed by a feasibility study of autologous peripheral blood stem cell transplantation in elderly patients with acute myeloid leukemia. Leukemia 13, 843–849 (1999). https://doi.org/10.1038/sj.leu.2401445
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.leu.2401445
Keywords
This article is cited by
-
Escalation of daunorubicin and addition of etoposide in the ADE regimen in acute myeloid leukemia patients aged 60 years and older: Cancer and Leukemia Group B Study 9720
Leukemia (2011)
-
Blood and marrow transplantation in elderly acute myeloid leukaemia patients – older certainly is not better
Bone Marrow Transplantation (2007)
-
Non-infusional vs intravenous consolidation chemotherapy in elderly patients with acute myeloid leukemia: final results of the EORTC-GIMEMA AML-13 randomized phase III trial
Leukemia (2006)
-
Standard induction chemotherapy followed by attenuated consolidation in elderly patients with acute myeloid leukemia
Annals of Hematology (2006)
-
Low transplant-related mortality with allogeneic stem cell transplantation in elderly patients
Bone Marrow Transplantation (2004)
