
Abstract
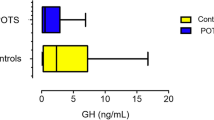
To determine the relationships between the circadian blood pressure profile and left ventricular mass, hormonal pattern and insulin sensitivity indices in patients with active acromegaly, ambulatory 24-h blood pressure monitoring (ABPM) was recorded in 25 subjects (47.0 ± 15.1 years, range 23–72). Serum growth hormone (GH) and insulin-like growth factor-1, fasting and mean plasma glucose and insulin during oral glucose tolerance test (OGTT), insulinogenic index, the sum of the plasma insulin levels and the homeostasis model insulin resistance index (Homa’s index) were determined. Left ventricular mass index (LVMI) was calculated from two-dimensional guided M-mode echocardiogram. The prevalence of hypertension was 56% (n = 14) and 40% (n = 10) according to sphygmomanometric measurements and ABPM, respectively. Non-dipping profile was observed in six of 10 hypertensives and in six of 15 normotensives. Serum growth hormone, fasting glucose, the area under the serum insulin curve and LVMI were higher for acromegalics with non-dipping profile than for dippers (all of them, P < 0.05). In non-dippers daytime heart rate was higher than night time (P < 0.001). In conclusion, the main observations in the present study suggested that both normotensive and hypertensive acromegalics had a highly prevalent non-dipping profile with a preserved circadian pattern of heart rate, that was associated with higher levels of serum GH. The disturbance in nocturnal blood fall in normotensives was associated with a decreased insulin sensitivity. The role of GH in blood pressure circadian rhythm regulation in essential hypertension deserves further studies.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Molitch ME Clinical manifestations of acromegaly Endocrinol Metab Clin North Am 1992 23 597–611
Rajasoorya C et alDeterminants of clinical outcome and survival in acromegaly Clin Endocrinol 1994 41 95–102
Ezzat S et alAcromegaly. Clinical and biochemical features in 500patients Medicine 1994 73 233–241
Hradec J et alLong-term echocardiography follow-up of acromegalic heart disease Am J Cardiol 1993 72 204–212
Fazio S et alImpaired cardiac performance is a distinct feature of uncomplicated acromegaly J Clin Endocrinol Metab 1994 79 441–447
López-Velasco R et alCardiac involvement in acromegaly J Clin Endocrinol Metab 1997 82 1047–1053
Minniti G et alPrevalence of hypertension in acromegalicpatients: clinical measurement versus 24-hour ambulatory blood pressure monitoring Clin Endocrinol 1998 48 149–152
Terzolo M et alTwenty-four hour profile of blood pressure inpatients with acromegaly. Correlation with demographic, clinical and hormonal features J Endocrinol Invest 1999 22 48–54
Shimada K et alDiurnal blood pressure variations and silent cerebrovascular damage in elderlypatients with hypertension J Hypertens 1992 10 875–882
O’Brien E, Sheridan J, O’Malley K Dippers and non-dippers Lancet 1988 ii 397–399
Pickering TG The clinical significance of diurnal blood pressure variations. Dippers and nondippers Circulation 1990 81 700–702
National Diabetes Data Group Classification and diagnosis of diabetes mellitus and other categories of glucose intolerance Diabetes 1976 25 245–249
Soeldner JS, Slone D Critical variables in the radioimmunoassay of serum insulin using the double antibody technique Diabetes 1976 14 775–779
Muller DC et alAn epidemiological test of the hyperinsulinemia-hypertension hypothesis J Clin Endocrinol Metabol 1993 76 544–548
Matthews DR et alHomeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man Diabetologia 1985 28 412–419
Kosaka K, Kuzuya T, Hagura R, Yoshinaga H Insulin response to oral glucose load is consistently decreased in established non-insulin-dependent diabetes mellitus: the usefulness of decreased early insulin response as a predictor of non-insulin-dependent diabetes mellitus Diab Med 1996 13 S109–S119
Kashiwabara H et alInsulin levels during fasting and the glucose tolerance test and Homa’s index predict subsequent development of hypertension J Hypertens 2000 18 83–88
Staessen JA, O’Brien ET, Atkins N, Amery AK Ambulatory blood pressure in normotensive compared with hypertensive subjects. The Ad-Hoc Working Group J Hypertens 1993 11 1289–1297
Devereux RB et alEchocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings Am J Cardiol 1986 57 450–458
Bianchi S, Bigazzi R, Campese VM Altered circadian blood pressure profile and renal damage Blood Press Monit 1997 6 339–346
Sica DA, White W Chronotherapeutics and its role in the treatment of hypertension and cardiovascular disease J Clin Hypertens 2000 2 279–286
Portaluppi C, Cortelli P, Provini F Alterations of sleep and circadian blood pressure profile Blood Press Monit 1997 6 301–313
Wilson DK, Sica DA, Miller SB Ambulatory blood pressure and dipping status in salt-sensitive and salt-resistant black adolescents Am J Hypertens 1999 12 159–165
Wilson DK, Sica DA, Miller SB Effects of potassium on blood pressure and dipping status in salt-sensitive and salt-resistant adolescents Hypertension 1999 34 176–181
Chen JW et alDifferential glucose tolerance in dipper and nondipper essential hypertension: the implications of circadian blood pressure regulation on glucose tolerance in hypertension Diabetes Care 1998 21 1743–1748
Verdecchia P, Porcellati C, Schillaci G Ambulatory blood pressure. An independent predictor of prognosis in essential hypertension Hypertension 1994 24 793–801
Lie JT, Grossman SJ Pathology of the heart in acromegaly: Anatomic findings in 27 autopsiedpatients Am Heart J 1980 100 41–46
Bruel A, Oxlund H Biosynthetic growth hormone increases the collagen deposition rate in rat aorta and heart Eur J Endocrinol 1995 132 195–201
Kraatz C et alAcromegaly and hypertension: prevalence and relationship to the renin-angiotensin aldosterone system Klin Wochenschr 1990 68 583–587
Colao A, Merola B, Ferone D, Lombardi G Acromegaly J Clin Endocrinol Metabol 1997 82 2777–2781
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pietrobelli, D., Akopian, M., Olivieri, A. et al. Altered circadian blood pressure profile in patients with active acromegaly. Relationship with left ventricular mass and hormonal values. J Hum Hypertens 15, 601–605 (2001). https://doi.org/10.1038/sj.jhh.1001239
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jhh.1001239
Keywords
This article is cited by
-
HOMA-IR in acromegaly: a systematic review and meta-analysis
Pituitary (2021)
-
Assessment of the awareness and management of cardiovascular complications of acromegaly in Italy. The COM.E.T.A. (COMorbidities Evaluation and Treatment in Acromegaly) Study
Journal of Endocrinological Investigation (2008)
