
Abstract
Study design:
This is a retrospective study.
Objectives:
The aim of this study is to examine the main features and short-term neurological outcomes associated with injuries to the spine due to diving into water in a Latin American country.
Setting:
Salvador, Brazil.
Patient sample:
A total of 1324 subjects were admitted with spinal trauma between 1991 and 2006 (inclusive). Subjects aged between 14 and 65 years who sustained diving injuries corresponded to 10.6% (N=140) of the cases.
Outcome measures:
Neurological status was determined by the Frankel Functional Scale (FFS) on admission and discharge. The FFS was secondarily converted to the American Spinal Injury Association impairment scale.
Methods:
This study is a patient record database review that examines demographic and injury-related characteristics, details of hospital treatment and neurological status at the time of discharge.
Results:
Males (N=129) outnumbered females (N=11) in a proportion of 12:1 (mean age: 28.62 years). The cervical spine region was the most affected area (92.1%) and 45% of the cases presented with tetraplegia. On admission, neurologically complete lesions accounted for 32.1% of the overall cases and 45.7% were neurologically intact. The mean length of stay (7.7 weeks) did not differ with regard to treatment option (P=0.83). During hospitalization, patients with incomplete neurological impairment had shorter lengths of stay and showed more neurological improvement than those with complete lesions (P=0.26 and 64.5 versus 2.2%, P<0.0001).
Conclusion:
Diving spine injuries have a high tetraplegia rate. Neurological recovery and shorter length of stay are associated with incomplete lesions.
Similar content being viewed by others


Introduction
When thinking about the dangers associated with water-related activities, the first risk that comes to mind is drowning. However, many people are often unaware of other disastrous consequences surrounding these practices.1 After death, spinal cord injuries (SCIs) are the most devastating result of water sports accidents, with regard to morbidity, permanent disability and cost.2 In the United States, spinal cord injury due to diving (SCID) is the fourth leading etiology of SCI, accounting for 8.5% of overall cases.3 Its prevalence varies throughout the world, ranging from 1.3% in Japan up to 23% in Russia.3 The cervical segment is most commonly affected, and tetraplegia results in the majority of these cases.2, 3 Reckless behavior, lack of diving training and alcohol use together contribute to highly avoidable incidence rates.2, 3, 4 This study aims to depict the main features and short-term neurological outcomes associated with injuries to the spine due to diving into water in a Latin American scenario.
Materials and methods
The medical records of 1324 subjects with the diagnosis of SCI between January 1991 and August 2006 (inclusive) were reviewed. Patients aged between 14 and 65 years (inclusive) who sustained injuries due to diving or jumping into water corresponded to 10.6% (N=140) of the cases. No SCI secondary to scuba diving were present, and clifftop diving is not a common practice in our geographical area. An electronic databank system provided information with regard to subjects’ age, sex, marital status, trauma environment (rural or urban area), level of injury of the spine, type of spine trauma, treatment plan, length of stay, and neurological status at the time of admission and discharge. Conservative treatment is defined as any nonoperative intervention: traction, closed reduction under fluoroscopic guidance, halo, spinal orthotic vest or brace. Surgical treatment is defined as any operative procedure. Before 2003, all subjects were assessed with plain X-ray films. Computerized tomography (CT) or magnetic resonance imaging were reserved only for cases with unclear radiological diagnosis. After 2003, all subjects were assessed with CT and plain X-ray films, with magnetic resonance imaging being performed according to specialist indication. Plain X-ray films of the whole spine are the protocol for patients with altered mental status. In the remaining cases, plain films and CT of other spine levels are performed following expert recommendation. The neurological function was assessed by a spine surgeon using the Frankel Functional Scale (FFS). During the databank processing, the FFS was converted to the American Spinal Injury Association (ASIA) impairment scale.5 This conversion was based on FFS grade and limbs sensory and motor function on admission and discharge. On discharge, neurological function change is considered as a one-grade variation on the initial ASIA impairment scale rating. Data concerning patients with fatal outcome in the emergency room, early transfer to another unit or, discharge from the hospital before being admitted in the Spine Trauma Unit could not be assessed. This study was approved by the local ethics committee.
Study location
The state of Bahia is localized in the northeastern part of Brazil (Figure 1). In 2008, the population was estimated as 14 109 000 of which 67.8% live in urbanized areas. Salvador is the capital of Bahia and the third largest Brazilian city, and it is located on the seacoast. Its metropolitan area accounts for 3 475 000 habitants, with a 98.4% urbanization rate.6 Almost half (44.3%) of the cases in this study occurred in Salvador. Brazil has universal health-care system, and the Bahia State General Hospital is the only public specialized unit in SCI care in the entire state of Bahia. The Bahia State General Hospital is located in Salvador.

Location of Salvador, Bahia, Brazil.
Statistics
Statistical analyses were made using the Epi Info Version 6.04a (Centers for Disease Control and Prevention, Atlanta, GA, USA).7 Data from the initial survey were analyzed using descriptive and comparative statistics. Comparative statistical analysis was performed using Student's t-test for continuous variables with normal distribution, and χ2-test for categorical variables frequencies. Confidence intervals at the 95% level were used to analyze data, and P<0.05 was considered statistically significant.
Results
The majority of study participants were male (92. 1%), outnumbering females in a ratio of 12:1 (Table 1). Among all subjects, the largest portion fell between 15 and 29 years of age (63%). Females were older than males at the time of the accident (mean age: female, 39.7 years; male: 27.7 years; P=0.002). Patients were resident of 54 different cities, with 86% coming from urban areas. Almost half of the cases (49.3%) happened during the summer (between December and March in the southern hemisphere) (Figure 2).

SCID monthly distribution.
In all, 129 (92.1%) injuries involved the cervical region, 4 (2.9%) thoracic and 7 (5%) lumbar. No sacral injuries were observed. The C5 level was affected in 42.1% of the cases, followed by C6 (19.3%). Seven subjects (5%) had multilevel lesions, all exclusively cervical. Fractures were responsible for more than half of the spine lesions (51.4%) and 52.8% of those were neurologically intact. (Table 2) On admission, 32.1% had complete lesions (ASIA A), 22.1% had incomplete lesions (ASIA B, C or D) and 45.7% of the patients were neurologically intact (Table 3). Most ASIA E subjects were submitted to surgery (85.9%, N=55).
Thirteen subjects (10.2%) were hospitalized for more than 90 days and there were no differences with regard to mean length of stay according to treatment option (P=0.82). Patients with incomplete lesions (ASIA B, C or D) had shorter hospitalization than those with complete lesions (44.6 versus 59.6 days, P=0.026). Subjects with noncervical trauma had a nonsignificant trend for shorter length of stay (mean 39.2 versus 55.7 days for cervical trauma, P=0.052).
At discharge, 15% (N=21) of the patients had some neurological improvement and 1.4% (N=2) deteriorated (Table 3). The two cases with neurological deterioration were located at the cervical level (traumatic discal hernia at C4 and medullary contusion at C3) and presented with a one- and two-level deterioration in the ASIA scale, respectively. Both were submitted to surgery. Neurological recovery was more likely for patients with incomplete lesions than complete (64.5 versus 2.2%, P<0.0001) and was not associated with vertebral lesion treatment choice (P=0.2) or influenced by age (P=0.97). Improvement of one grade on the ASIA impairment scale was present in 85% (N=17) of the cases that evolved with recovery. Of these, nine cases progressed from ASIA D to ASIA E. Only one subject out of the 45 with complete lesions on admission presented with partial neurological improvement at discharge.
Discussion and conclusions
Diving is a major cause of sport/recreational SCI.2, 3, 4, 8, 9, 10, 11, 12, 13, 14, 15 Demographic features of diving spinal trauma in this study corresponded to international literature: adolescents and young adults, males and unmarried. The observed ratio for gender (12:1) was also comparable to the 5:1 to 32:1 range found in other studies.2, 3, 4, 8, 9, 10, 11, 12, 13, 14, 15
Overall, the cervical segment was the most commonly affected region, with the C5 level, followed by C6, accounting for the majority of the spinal trauma. Similar findings were published in numerous other studies, and may be associated with the narrower vertebral canal and broad range of motion at this spine level.3, 4, 11, 12, 13, 14
All multilevel injuries in this study were located exclusively in the cervical segment. In other previous investigations, multilevel lesions had an overall higher incidence rate, with thoracic and lumbar segments seldom involved.2, 12 Multilevel injuries assessment in this study was likewise insufficient. Systematic whole-spine radiographic screening exclusively for subjects with altered mental status could have been an inefficient strategy to identify occult vertebral injuries. The sensitivity of clinical history and physical examination to determine further investigation is generally questionable, and all patients with documented spine trauma should have received whole-spine radiological evaluation independently of initial level of consciousness.16
Fracture and fracture–luxation are the predominant types of spinal trauma due to diving.2, 12 SCIs without radiological evidence of trauma could be associated with preexisting cervical spine abnormalities and hyperflexion–hyperextension movements, mechanisms related to wave-forced impact.17
Despite lacking neurological involvement, 85.9% of the neurologically intact cases were submitted to surgery. The formal indications for surgical intervention are post-traumatic instability and persistent neurological deficit.13 The high overall surgical rate presented (92.1%) could also reflect Bahia State General Hospital's health system role. As a tertiary center, it receives referrals from smaller units across the state that can exclusively handle SCI conservative management. The rate for surgical intervention varied from 20 to 83.2% in other studies.4, 9
Recovery is unusual for complete injuries, and when improvement is present for incomplete lesions, it is often partial with important functional compromise.5, 9, 12, 14, 15 Patients with complete lesions or cervical spine trauma tend to stay longer in the hospital.18 This situation occurs mostly due to their extended neurological impairment, potential mechanical ventilation support need and subsequent complications.18 In this study, subjects with complete neurological injuries had longer hospitalizations (P=0.026) and victims of noncervical lesions had a nonsignificant trend for shorter length of stay (P=0.052).
Notably, the low availability of CT scans before 2003 has an important role in this study. CT studies offer detailed information about spinal canal involvement, epidural space constriction and presence of interspinal fragments, critical information for diagnosis and treatment decision-making. Furthermore, additional injuries may have been missed in this incomplete assessment—even after acknowledging that cases with indeterminate diagnosis were submitted to further radiological evaluation. Barrett et al.19 found that over a third of patients with an identified cervical spine fracture on initial plain X-ray can have a secondary cervical spine fracture detected by CT that was not evident on the plain radiograph, and the majority of these concomitant injuries had clinical significance.
The warm weather throughout the year in Brazil and other Latin American countries stimulates the practice of water-related sports for a longer period than subtropical climate regions, which prompts higher exposure to SCID. Despite the fact that almost half of the cases in this series occurred during the summer, the case distribution was more spread out across the year. This pattern contrasts with some European studies with more than 70% of the accidents taking place in the summertime.9, 13 This aspect is particularly important for injury prevention education in tropical countries, which would benefit longer-duration campaigns before, during and after the summer.
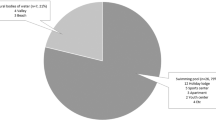
Detailed information about the specific setting involving the injuries included in this study was not available in our records. However, in urban settings special attention should be given to private swimming pools.3 Almost a third of all SCID in the United States occurs in pools, particularly during parties, usually where no lifeguard or depth indicators are available.3, 10 Swimming is the third national sport in Brazil, placed behind soccer and volleyball. Brazil has over 1 300 000 swimming pools, twice as many as France and Spain (which are the leading European countries with respect to number of swimming pools) combined. It is surpassed only by the United States with 7.6 times as many pools.20 At least 11 million Brazilians frequent swimming pools, and unmeasurable more have access to rivers, lakes and sea, which exponentially increases the population at risk.20
The establishment of universal health care in Brazil in 1988 brought great advancements to health-care attention, especially to the poor underserved population. However, the resources available today still do not meet basic necessities of a great portion of the Brazilian people, yielding the innumerous structural adversities faced on health-care attention in Brazil. Despite having a Spine Trauma Unit providing advanced care in the state, one of the major obstacles faced is basic transportation between facilities. Life flight is not available and the majority of the ambulances across the state's countryside do not have equipment to provide safe transference for SCI victims. Neurological impaired patients require complex transportation management, especially with regard to proper immobilization, associated injuries care and respiratory support. SCID cases can be even more challenging when near-drowning complications are present. Therefore, many of these patients have to receive medical care in local nonspecialized hospitals and do not have the opportunity to receive attention of spine surgery experts. In addition, small hospitals in Brazil frequently do not have equipment or staff to perform appropriate radiological evaluation of SCI, potentially leading to diagnostic failure.
Tetraplegia is frequently the rule for SCID, and complete lesions were the number one neurological outcome in several previous studies.2, 3, 4, 10, 11, 12, 14, 15 In this investigation, an uncommonly high frequency of neurological intact vertebral injuries were present (N=64, 45.7%). This numbers could be a consequence of the transportation and radiological assessment issues addressed above. Stable victims who do not require advanced life support or major special needs secondary to SCID would be in better condition for transference to the Spine Trauma Unit than neurologically impaired victims.
It is difficult to compare data between several published studies of SCID. There are many differences in their inclusion and categorization criteria.4, 9 Furthermore, neurological function assessment varies between SCID studies started before the ASIA impairment scale establishment.2, 4, 12, 14, 15
The nature of the administrative databases also imposes potential limitations. In particular, this study lacks information with regard to associated injuries, methylprednisolone use, complications and other functional outcomes. Furthermore, the FFS was the primary neurological evaluation, and the conversion to the ASIA impairment scale occurred only during the databank research stage. This is a significant drawback especially for functional changes assessment and clinical syndromes presentation.
Case observation was most likely incomplete. Victims who died immediately from drowning, before reaching the hospital or during emergency initial treatment, may have had undetected spinal injuries. Individuals with rapidly resolving neurological deficits at the emergency room or those who died in the critical care unit may have contributed to an underestimation of cases. Patients discharged from the hospital before being admitted in the Spine Trauma Unit commonly had minor spinal trauma, were neurologically intact and received outpatient conservative management, which also could cause a biased profile of this population.
To the best of our knowledge, this study represents the most comprehensive study on spine trauma due to diving established in Latin America reported to date. Many elements contribute to a high incidence of SCID, nonetheless, the gross part of these injuries is potentially preventable. We highlight the claim for educational campaigns with a main focus on the young, male and single population, especially during the summer. The high need for investments in infrastructure for transportation and medical technology should be stressed.
References
Blitvich JD, McElroy GK, Blanksby BA, Douglas GA . Characteristics of ‘low risk’ and ‘high risk’ dives by young adults: risk reduction in spinal cord injury. Spinal Cord 1999; 37: 553–559.
Green BA, Gabrielsen MA, Hall WJ, O’Heir J . Analysis of swimming pool accidents resulting in spinal cord injury. Paraplegia 1980; 18: 94–100.
DeVivo MJ, Sekar P . Prevention of spinal cord injuries that occur in swimming pools. Spinal Cord 1997; 35: 509–515.
Bailes JE, Herman JM, Quigley MR, Cerullo LJ, Meyer Jr PR . Diving injuries to the cervical spine. Surg Neurol 1990; 34: 155–158.
Maynard Jr FM, Bracken MB, Creasey G, Ditunno Jr JF, Donovan WH, Ducker TB et al. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association. Spinal Cord 1997; 35: 266–274.
Oliveira LAP . In: Bivar W (ed). Síntese de indicadores sociais: uma análise das condições de vida da população brasileira. Instituto Brasileiro de Geografia e Estatística: Rio de Janeiro, 2008, pp 31–37.
Dean AG, Dean JA, Coulombier D, Brendel KA, Smith DC, Burton AH et al. Epi Info, Version 6.04a, a word processing, database, and statistics program for public health on IBM-compatible microcomputers. Centers for Disease Control and Prevention: Atlanta, GA, USA, 1996.
Shields Jr CL, Fox JM, Stauffer ES . Cervical cord injuries in sports. Phys Sports Med 1978; 6: 71–76.
Aito S, D’Andrea M, Werhagen L . Spinal cord injuries due to diving accidents. Spinal Cord 2005; 43: 109–116.
Kluger YK, Jarosz D, Paul DB, Townsend RN, Diamond DL . Diving injuries: a preventable catastrophe. J Trauma 1994; 36: 349–351.
Schmitt H, Gerner HJ . Paralysis from sport and diving accidents. Clin J Sport 2001; 11: 17–22.
Tator CH, Edmonds VE, New ML . Diving: a frequent an potentially preventable cause of spinal cord injury. Can Med Assoc J 1981; 124: 1323–1324.
Korres DS, Benetos IS, Themistocleous GS, Mavrogenis AF, Nikolakakos L, Liantis PT . Diving injuries of the cervical spine in amateur divers. Spine J 2006; 6: 44–49.
Albrand OW, Corkhill G . Broken neck from diving accidents: a summer epidemic in young men. Am J Sports Med 1976; 4: 107–110.
Kiwerski JE . Cervical spine injuries caused by diving into water. Paraplegia 1980; 18: 101–109.
American College of Surgeons In: Advanced Trauma Life Support Student Manual. 6th edn. American College of Surgeons: Brazil, 1999, pp 226.
Chang SK, Tominaga GT, Wong JH, Weldon EJ, Kaan KT . Risk factors for water sports-related cervical spine injuries. J Trauma 2006; 60: 1041–1046.
Tooth L, McKenna K, Geraghty T . Rehabilitation outcomes in traumatic spinal cord injury in Australia: functional status, length of stay and discharge setting. Spinal Cord 2003; 41: 220–230.
Barrett TW, Mower WR, Zucker MI, Hoffman JR . Injuries missed by limited computed tomographic imaging of patients with cervical spine injuries. Ann Emerg Med 2006; 47: 129–133.
Nolasco VP, Pável RC, Moura R . In: DaCosta L (ed). Atlas do Esporte no Brasil. CONFEF: Rio de Janeiro, 2006, pp 8232–8235.
Acknowledgements
We express appreciation to all members of the Liga do Trauma—Escola Bahiana de Medicina e Saúde Pública, Dr Juarez Dias, physicians, hospital and rehabilitation personnel of the Hospital Geral do Estado who assisted in the data collection, entry or by providing technical advice. We especially thank Cassandra Delp for detailed help during preparation of the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Amorim, E., Vetter, H., Mascarenhas, L. et al. Spine trauma due to diving: main features and short-term neurological outcome. Spinal Cord 49, 206–210 (2011). https://doi.org/10.1038/sc.2010.79
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.79
Keywords
This article is cited by
-
Rehabilitation outcome in people with spinal cord injuries resulting from diving in South Korea
Spinal Cord Series and Cases (2022)
-
Prevention of diving-induced spinal cord injuries—preliminary results of the first Romanian mass media prophylactic educational intervention
Spinal Cord Series and Cases (2017)
