
Abstract
Study design:
Experimental rat model of spinal cord contusion.
Objectives:
To reveal the extent of spinal autonomy contributing to recovery of hindlimb function.
Setting:
Experimental laboratory of a neurosurgical university department.
Methods:
F-wave amplitudes as a probe for spinal cord excitability were recorded from both sciatic nerves (lumbar segments L2–L5) before and after an experimental spinal cord contusion performed in the lower thoracic spinal cord. Additionally, transcranial electrically motor evoked potentials from the hindlimbs and cerebral somatosensory potentials evoked by sciatic nerve stimulation were recorded. Clinical evaluation of hindlimb function was done regularly for survival periods of 3 and 50 days, respectively. Electrophysiological testing was performed immediately prior and after lesioning of the cord and at the endpoint of survival periods.
Results:
Hindlimb function recovered from a mean Basso–Beattie–Bresnahan score of 5.6 on day 1 to 9.2 on day 3 (3-day-survivors) and from 7.7 to 17.2 on day 50 (50-day-survivors). This was accompanied by a significant increase of F-wave amplitudes on day 50 compared to baseline values, whereas amplitudes of somatosensory and motor-evoked potentials remained significantly depressed.
Conclusion:
Recovery of hindlimb function may at least in part be attributed to evolving spinal autonomy, which can be assessed by F-wave amplitudes.
Similar content being viewed by others

Introduction
Graded lesions of the rat thoracic spinal cord yield graded clinical and electrophysiological changes.1, 2, 3 These animals exhibit a certain recovery of hindlimb function within different periods of survival. Recovery of function has been attributed to a putative regeneration of function of long spinal fiber tracts. Several authors, however, have described the existence of a ‘central locomotor pattern generator’ in cats and mice as well as in other animals4, 5 which they refer to as a center of locomotion for the hindlimbs situated in the thoracolumbar spinal cord segments. Today, autonomy of this locomotor pattern generator that develops after spinal cord injury is considered to be even more important in the context of functional recovery than regeneration of the long spinal fiber tracts themselves.4
Recordings of F waves from the limbs are currently used as a diagnostic tool in diseases of the peripheral nervous system. In addition, these can be employed as a test of spinal segmental excitability as was described by several authors.6, 7, 8, 9
The following investigation was done to reveal whether evolving spinal autonomy after spinal cord contusion can be detected by simple hindlimb F-wave recording.
Materials and methods
This investigation was carried out under approval and permission of the local government and the ethics committee. The authors certify that all applicable institutional and governmental regulations concerning the ethical use of animals were followed during the course of this research. A total of 23 male Wistar rats (body weight 350–480 g) was split into three groups: group 1 (n=10 rats) receiving laminectomy and spinal cord compression with a survival period of 3 days; group 2 (n=10 rats) receiving laminectomy and spinal cord compression with a survival period of 50 days; group 3 (controls, n=3 rats) receiving laminectomy but no spinal cord compression with a survival period of 50 days. Rats were anesthesized with intraperitoneal application of Nembutal (Narcoren®, 50 mg/kg body weight), placed on a heating pad, and underwent a one-level laminectomy at Th8 under microscopic view to expose the dura mater and the underlying mid-thoracic spinal cord. Both sciatic nerves were exposed for electrical stimulation. After exposure of the spinal cord, the spinal cord compression device (developed and manufactured by Dipl. Ing. J Staszewski, Department of Physiology, University of Cologne) was brought into the field. This device consisted of a blunt plastic rod (tip diameter 2.5 mm), which was driven by a stepper motor and feedback-controlled via a strain gauge. The whole device was held and moved by a micromanipulator. The tip of the plastic rod was put on the exposed spinal cord without exerting any pressure. For groups 1 and 2, the stepper motor was then set on and the spinal cord compressed with a force increasing by 10 g/s to a maximum impact equivalent of 60 g held for 3 s followed by an immediate and complete relief. Animals were rigidly fixed to the ground plate of the compression device. Electrophysiological investigations consisted of recording somatosensory potentials from subdermal needle electrodes placed on the skull evoked by bilateral simultaneous stimulation of the sciatic nerves (suprathreshold constant voltage monophasic pulses of 0.1 ms duration at a frequency of 3 Hz), of motor potentials (evoked by a transcranially applied train of five monophasic constant current pulses (interstimulus interval 2 ms), intensity 10–15 mA, recording of the compound muscle action potential of the plantar muscles using subdermal needle electrodes), and of F waves from the sciatic nerves (corresponding to spinal segments L2–L5) as a parameter of spinal segmental excitability (separate stimulation of both sciatic nerves, suprathreshold constant voltage monophasic pulses of 0.1 ms duration at a frequency of 1 Hz). Electrophysiological measurements were performed using a standard two-channel electrophysiological stimulation and recording device (NihonKohden Inc., Tokyo, Japan) prior to spinal cord compression after laminectomy and immediately after experimental spinal cord injury. Wounds were closed in layers and animals transferred to the housing room where they were kept at a 12/12 h day/night rhythm and access to food and water ad libitum. Analgesics were administered if necessary. After that, 10 rats (group 1) were followed clinically for 3 days by testing hindlimb function using the Basso–Beattie–Bresnahan (BBB) scale10 which allows standardized clinical assessment of hindlimb function in rats. The BBB scale ranges from 0 (‘no observable hindlimb movement’) to 21 (‘consistent plantar stepping and coordinated gait, consistent toe clearance, predominant paw position is parallel throughout stance, consistent trunk stability, tail consistently up’). After 3 days, these rats were again anesthesized as described above, re-examined electrophysiologically, and then sacrificed. Group 2 (10 rats) was observed for a period of 50 days, the hindlimb function being evaluated clinically using the BBB score, re-examined on day 50 electrophysiologically after anesthesia, and afterwards sacrificed. Control rats survived for a period of 50 days and were then tested clinically and reexamined electrophysiologically in general anesthesia and sacrificed thereafter.
BBB scores, evoked potentials amplitudes, and F-wave amplitudes of the separate groups (3-day-survivors, 50-day-survivors, controls) were analyzed separately using student's t-test for paired samples, facilitated by a standard statistical software package (SPSS).
Results
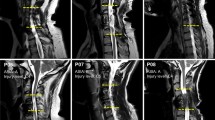
Histological analysis revealed that the predominant lesion of the cord by application of the compression model described above occurred in the dorsal part of the medulla where corticospinal fiber tracts are located (Figure 1). An example of evoked potential and F-wave recordings is given in Figure 2.

Histological section of a rat spinal cord lesioned by the compression technique described above. Note the predominant contusion of the dorsal fiber tracts

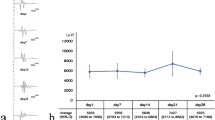
Electrophysiological recordings (MEP, SEP, F waves) obtained before spinal cord compression (‘baseline’), on day 3, and on day 50 after spinal cord compression
Statistical comparison of F-wave and MEP amplitudes of left and right hindlimbs did not reveal interside differences. Therefore, amplitudes of both sides were averaged for further analysis. Spinal cord compression had different effects on SEP, MEP, and F-wave amplitudes: whereas SEP and MEP amplitudes decreased, F-wave amplitudes were only moderately depressed compared to amplitudes measured immediately prior to compression.
Among the 3-day-survivor group, the initially severe impairment of hindlimb function (mean BBB score on day 1:5.6 (SD 5.0)) had improved (mean BBB score on day 3:9.2 (SD 5.4)). This improvement – in terms of the BBB scale: from ‘extensive movement of all three joints of the hindlimb’ to ‘occasional weight supported plantar steps, no forelimb-hindlimb coordination’ – was statistically significant (P<0.001). Electrophysiological parameters (MEP and SEP amplitudes) obtained at this time point were depressed (P<0.001) except for F-wave amplitudes (Table 1, Figure 2).
After a survival period of 50 days, BBB scores had raised to a mean value of 17.2 (SD 1.7; P<0.001 for significance compared to BBB score on day 1) corresponding to a near-normal function of the hindlimbs with consistent coordinated gait, frequent to consistent toe clearance, and a predominantly parallel position of the paw during sweeping. MEP and SEP amplitudes, in contrast, remained severely and significantly (P<0.001) depressed (Table 2, Figure 2) at reexamination on day 50. F-wave amplitudes, however, had increased significantly (P<0.001) at this time point.
Control rats exhibited normal hindlimb function (BBB score 20–21) during the whole observation period. MEP and SEP as well as F-wave amplitudes obtained after laminectomy and 50 days after surgery bore only minor variations lacking statistical significance (Table 3).
Discussion
The results presented above can be summarized as follows: Recovery of hindlimb function in rat spinal cord contusion occurs without significant functional restoration of descendent and ascendent long fiber tracts of the dorsal spinal cord. Recovery is paralleled by an increase in spinal segmental excitability below the site of lesion of the cord. Recovery may, therefore, at least in part be attributed to evolving autonomy of spinal locomotor pattern generators.4, 5
F-wave amplitudes as a probe for segmental spinal excitability
Several reports have emphasized the usefulness of F-wave recording to reveal changes in the spinal cord excitatory state.6, 7, 8, 9 Specifically, under the condition of a loss of supraspinal control conveyed by corticospinal fiber tracts, developing hyperexcitability can be monitored by means of F-wave amplitudes.6, 7 F waves have been used to demonstrate the impact of cortical modulation on segmental spinal excitability.8 As was recently reviewed in the context of spinal locomotion pattern generation,5 a CNS motor lesion yields a loss of supraspinal drive as well as an impairment of spinal reflex control which is then followed by hyperexcitability resulting in spasticity. According to the conclusions made by the authors cited, defective supraspinal control with a corresponding change of the spinal segmental excitatory state can be measured by changes of F-wave amplitudes.6, 7, 8, 9 The findings reported above extend support to this hypothesis.
Locomotion control via propriospinal and reticulospinal pathways
While the lesion induced in the rat spinal cord as described above particularly affects the dorsal white matter and thus the pyramidal tract, more ventrally located pathways, for example the propriospinal and reticulospinal pathways, are spared. These tracts are known to control locomotion patterns and to provide interlimb coordination which regenerate to a major extent in the rats studied here (cf. Tracey11 and Jordan12 for a review). The discrepancy between depression of MEP and SEP amplitudes on one hand, and the extent of clinical recovery on the other could also be explained by a restoration of function in the ventrolateral propriospinal and reticulospinal tracts while function of dorsal fiber tracts remains impaired. Selective lesioning of the corticospinal tract can also account for major changes in segmental excitability, as has been demonstrated recently in the rat.13
Spinal locomotion pattern generators and functional recovery after spinal cord injury
The existence of a neuronal network generating locomotor patterns of activity has been described extensively in the neonatal rat and cat as well as in other species (reviewed by Grillner4). Lumbar segments L2 and L5 appeared to possess the most elaborate encoding capacity. Not only in neonate, but also in adult animals after complete transsection of the spinal cord, appropriate locomotor coordination with weight support is observed after several weeks of treadmill training.4, 14, 15 The spinal locomotor pattern generator serves as a substitute to initiate and maintain locomotor function in rat spinal cord contusion – the increase of spinal segmental excitability with time (as documented by increasing F-wave amplitudes) accompanied by functional recovery without restoration of cerebrospinal tract function represents an argument to support this notion.
References
Nacimiento AC, Bartels M, Loew F . Acute changes in somatosensory evoked potentials following graded experimental spinal cord compression. Surg Neurol 1986; 25: 62–66.
Baskin DS, Simpson RK . Corticomotor and somatosensory evoked potential evaluation of acute spinal cord injury in the rat. Neurosurgery 1987; 20: 871–877.
Fehlings MG, Tator CH, Linden RD . The relationship among the severity of spinal cord injury, motor and somatosensory evoked potentials and spinal cord blood flow. Electroencephalogr Clin Neurophysiol 1989; 74: 241–259.
Grillner S . The spinal locomotor CPG: a target after spinal cord injury. Prog Brain Res 2002; 137: 97–108.
Dietz V . Spinal cord pattern generators for locomotion. Clin Neurophysiol 2003; 114: 1379–1389.
Eisen A, Odusote K . Amplitude of the F wave: a potential means of documenting spasticity. Neurology 1979; 29: 1306–1309.
Milanov IG . F-wave for assessment of segmental motoneurone excitability. Electromyogr Clin Neurophysiol 1992; 32: 11–15.
Mercuri B, Wassermann EM, Manganotti P, Ikoma K, Samii A, Hallett M . Cortical modulation of spinal excitability: an F-wave study. Electroencephalogr Clin Neurophysiol 1996; 101: 16–24.
Fisher MA . F-wave studies: clinical utility. Muscle Nerve 1998; 21: 1098–1101.
Basso DM, Beattie MS, Bresnahan JC . A sensitive and reliable locomotor rating scale for open field testing in rats. J Neurotrauma 1995; 12: 1–21.
Tracey DJ . Ascending and descending pathways in the spinal cord. In: Paxinos G (ed). The Rat Nervous System 2nd edn. Academic Press: New York 1995, pp 67–80.
Jordan LM . Brainstem and spinal cord mechanisms for the initiation of locomotion. In: Shimamura M, Grillner S, Edgerton VR (eds). Neurobiological Basis of Human Locomotion. Japan Scientific Societies Press: Tokyo 1991, pp 3–20.
Chen XY, Wolpaw JR . Probable corticospinal tract control of spinal cord plasticity in the rat. J Neurophysiol 2001; 87: 645–652.
Rossignol S . Neural control of stereotypic limb movements. In: Rowell LB, Sheperd JT (eds). Handbook of Physiology. Oxford University Press: New York 1996, pp 173–216.
Edgerton VR et al. Retraining the injured spinal cord. J Physiol 2001; 533: 15–22.
Acknowledgements
We are indebted to Dr H Stützer, Department of Medical Statistics, University of Cologne, for helpful statistical advice.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Wedekind, C., Ullrich, R. & Klug, N. F-wave amplitudes indicate evolving spinal autonomy during spontaneous recovery of hindlimb function in rat spinal cord contusion. Spinal Cord 44, 44–48 (2006). https://doi.org/10.1038/sj.sc.3101791
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101791
