
Abstract
Objective: To report an unusual presentation of a misplaced suprapubic catheter (SPC) in a spinal cord injury (SCI) patient.
Design: A case report of a SCI patient in whom a SPC was `partially misplaced' in an emergency.
Setting: London Spinal Injuries Unit, Stanmore, UK.
Subject: A 33-year-old man who sustained a C5 SCI in a road traffic accident 6 months ago. He had an indwelling urethral catheter, which blocked off and repeated attempts to reinsert another one per urethra were unsuccessful.
Main outcome measure: A SPC was inserted in an emergency at the bedside, as he developed autonomic dysreflexia. The catheter initially drained clear urine but subsequently the flow became intermittent. He also started complaining of lower abdominal discomfort.
Results: The abdominal examination was unremarkable without signs of peritonism. An ultrasound scan of the abdomen revealed the eye of the catheter in the bladder but the balloon had been inflated in the subcutaneous tissues. It was reinserted under cystoscopic control in the operating theatre.
Conclusion: The insertion of a SPC in a neuropathic patient can be a challenge even for an experienced urologist. As these patients often have small capacity bladders, the SPC should be inserted under cystoscopic control wherever possible. However if they are inserted blindly there should be a high index of suspicion for the potential complication of a misplaced catheter. The patient should undergo regular abdominal examination and an ultrasound scan should be performed as soon as possible for confirmation.
Similar content being viewed by others


Introduction
There are a number of methods for bladder management in patients with a SCI. A SPC can be used for bladder drainage on a temporary or permanent basis in this patient group. There are a number of reports in the literature of small bowel obstruction from a misplaced SPC.1,2
We report an interesting case of a `partially misplaced' SPC leading to intermittent bladder drainage and giving a false sense of security.
Case Report
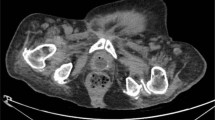
A 33-year-old man with an incomplete C5 SCI developed blockage of the urethral catheter. Repeated attempts at recatheterization failed. He developed autonomic dysreflexia and a decision was made to insert a SPC in an emergency. Ten millilitres of Lignocaine were instilled 2.5 cms above the symphysis pubis and a distended bladder was confirmed with a spinal needle. A 2.5 cms stab incision was made at the site of local anaesthesia and a size 16F ADD-A-Cath® (Femcare Ltd., Nottingham, UK) was inserted. The trocar with sheath was pushed through the abdominal wall into the bladder. On removal of the trocar, urine started to drain immediately. A 16F silicone catheter was pushed through the sheath and after confirming the free flow of urine 10 ml of sterile water was instilled in the catheter balloon without difficulty. The tear off strip was used to remove the sheath from around the catheter. The procedure was uncomplicated. Subsequently the drainage became intermittent and the patient complained of lower abdominal discomfort. The examination revealed a soft, non-tender abdomen. Bowel sounds were present and there was no evidence of peritonism. An ultrasound scan revealed the eye of the catheter in the bladder however the balloon had been inflated in the pre-vesical space (Figures 1 and 2). He underwent an emergency reinsertion of SPC under cystoscopic control in theatre without any complications.

Ultrasound scan in transverse section eye of catheter inside bladder with balloon in pre-vesical space

Ultrasound scan in longitudinal section; catheter balloon in pre-vesical space
Discussion
The blind insertion of a SPC can be a daunting task, especially in a neuropathic patient. We believe that a SPC should always be inserted under cystoscopic control in this patient group. However, if this procedure is undertaken in an emergency then a high index of suspicion should be maintained for potential complications. The patient should undergo regular examinations and an ultrasound scan should be performed at the earliest to confirm the presence of the catheter in the correct position. There are a number of reports in the literature of misplaced SPC injuring the bowel.3,4 We want to emphasise from this particular case that if a SPC initially drains urine freely but subsequently the drainage becomes intermittent, without signs of peritonism then its `partial misplacement' should be suspected. This complication of a misplaced SPC without injuring the bowel is one which is probably more frequent than we suspect but to our knowledge has never been reported. We hope that this particular complication will be recognised and prompt management instituted where appropriate.
Our case once again underlines the extreme vigilance required for this simple procedure in patients with spinal cord injuries.
References
Simpson RR . An unusual cause of bowel obstruction: the misplaced suprapubic catheter J Urol 2001 165: 1998
Sullivan LP, Davidson PG, Kloss DA, D'Anna Jr JA . Small bowel obstruction caused by a long term indwelling urinary catheter Surgery 1990 107: 228–230
Goldblum D, Brugger JJ . Bowel obstruction caused by dislocation of a suprapubic catheter Surg Endosc 1999 13: 283–284
Farina LA . Small-bowel obstruction by bladder catheter Surgery 1991 110: 119
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Hamid, R., Peters, J. & Shah, P. Pitfall in insertion of suprapubic catheter in patients with spinal cord injuries. Spinal Cord 40, 542–543 (2002). https://doi.org/10.1038/sj.sc.3101385
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101385
Keywords
This article is cited by
-
Non-surgical urologic management of neurogenic bladder after spinal cord injury
World Journal of Urology (2018)
-
Preventable long-term complications of suprapubic cystostomy after spinal cord injury: Root cause analysis in a representative case report
Patient Safety in Surgery (2011)
-
Letter to the Editor
Spinal Cord (2003)
