
Abstract
Traditional flexible endoscopy has been limited to the confines of the gastrointestinal lumen; however, recent developments involving transluminal access to intra-abdominal structures hold the potential to revolutionize flexible endoscopy. Over the past few years various studies have detailed techniques that intentionally breach the lumen and provide endoscopic access to the peritoneal cavity for diagnostic and therapeutic procedures. Unlike standard surgical approaches, which require incisions to be made in the abdominal wall, natural orifice transluminal endoscopic surgery (NOTES) avoids the need for abdominal incisions and can offer specific advantages to select patient populations. Animal models have been used to demonstrate the possible applications of NOTES, including transgastric peritoneoscopy, tubal ligation, gastrojejunostomy, partial hysterectomy, oophorectomy, and transcolonic exploration, liver biopsy and cholecystectomy. In this Review, we highlight important advances in NOTES since it was first described and analyze the hazards and potential benefits associated with this innovative approach.
Key Points
-
Endoscopic access to the peritoneal cavity via transgastric and transcolonic routes has been recently described in animal models and termed Natural Orifice Transluminal Endoscopic Surgery (NOTES)
-
This 'scarless' surgery avoids abdominal incisions and could be advantageous in specific patient populations
-
With improved endoscopic tools, NOTES could become an acceptable alternative and the preferred approach for management of certain abdominopelvic conditions in select cases
-
The proposed benefits and safety of scarless access to the peritoneal cavity need to be conclusively demonstrated in clinical studies before universal acceptance of NOTES
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Litynski GS (1999) Endoscopic surgery: the history, the pioneers. World J Surg 23: 745–753
Decker A et al. (1944) Culdoscopy: A new method in the diagnosis of pelvic disease—a preliminary report. Am J Surg 64: 40–44
Litynski GS (1998) Erich Muhe and the rejection of laparoscopic cholecystectomy (1985): a surgeon ahead of his time. J Soc Laparoendosc Surg 2: 341–346
Mouret P (1991) From the first laparoscopic cholecystectomy to the frontiers of laparoscopic surgery: the future perspectives. Dig Surg 8: 1124–1125
Keus F et al. Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database of Systematic Reviews 2006, Issue 4. Art. No.: CD006231. DOI: 10.1002/14651858.CD006231
Ceppa FA et al. (2007) Laparoscopic transgastric endoscopy after Roux-en-Y gastric bypass. Surg Obes Relat Dis 3: 21–24
Peters M et al. (2002) Laparoscopic transgastric endoscopic retrograde cholangiopancreatography for benign common bile duct stricture after Roux-en-Y gastric bypass. Surg Endosc 16: 1106
Kalloo AN et al. (2004) Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest Endosc 60: 114–117
ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery White Paper 2005 (2006) Gastrointest Endosc 63: 199–203
Jagannath SB et al. (2005) Peroral transgastric endoscopic ligation of fallopian tubes with long-term survival in a porcine model. Gastrointest Endosc 61: 449–453
Kantsevoy SV et al. (2005) Endoscopic gastrojejunostomy with survival in a porcine model. Gastrointest Endosc 62: 287–292
Park PO et al. (2005) Experimental studies of transgastric gallbladder surgery: cholecystectomy and cholecystogastric anastomosis. Gastrointest Endosc 61: 601–606
Wagh MS et al. (2005) Endoscopic transgastric abdominal exploration and organ resection: initial experience in a porcine model. Clin Gastroenterol Hepatol 3: 892–896
Wagh MS et al. (2006) Survival studies after endoscopic transgastric oophorectomy and tubectomy in a porcine model. Gastrointest Endosc 63: 473–478
Merrifield BF et al. (2006) Peroral transgastric organ resection: a feasibility study in pigs. Gastrointest Endosc 63: 693–697
Kantsevoy SV et al. (2006) Transgastric endoscopic splenectomy: is it possible? Surg Endosc 20: 522–525
Wilk PJ (1994) Method for use in intra-abdominal surgery. US Patent 5,297,536
Tsin DA et al. (2003) Culdolaparoscopic cholecystectomy during vaginal hysterectomy. J Soc Laparoendosc Surg 7: 171–172
Natural Orifice Surgery Consortium for Assessment and Research (NOSCAR™) International Conference on Natural Orifice Translumenal Endoscopic Surgery (NOTES™) [http://www.noscar.org/conference06.html]
Pai RD et al. (2006) Transcolonic endoscopic cholecystectomy: a NOTES survival study in a porcine model (with video). Gastrointest Endosc 64: 428–434
Fong DG et al. (2007) Transcolonic endoscopic abdominal exploration: a NOTES survival study in a porcine model. Gastrointest Endosc 65: 312–318
Fong DG et al. (2006) Transcolonic hepatic wedge resection in a porcine model [abstract]. Gastrointest Endosc 63: AB102
Chak A et al. (2006) EUS Guided natural orifice transvisceral endoscopic surgical (NOTES) approach to the retroperitoneum [abstract]. Gastrointest Endosc 63: AB264
Matthes K et al. (2006) Feasibility of endoscopic transgastric distal pancreatectomy (ETDP) in the pig [abstract]. Gastrointest Endosc 63: AB229
Fong DG et al. (2006) Transcolonic access to the peritoneal cavity using a novel incision and closure device [abstract]. Gastrointest Endosc 63: AB233
Pasricha P et al. (2005) A next generation therapeutic endoscope: development of a novel endoluminal surgery system with “birds-eye” visualization and triangulating instruments [abstract]. Gastrointest Endosc 61: AB106
Swanstrom LL et al. (2005) Development of a new access device for transgastric surgery. J Gastrointest Surg 9: 1129–1137
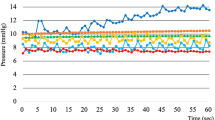
Park PO et al. (2006) Measurements of intraperitoneal pressure during flexible transgastric surgery and the development of a feed-back control valve for regulating pressure [abstract]. Gastrointest Endosc 63: AB101
Hu B et al. (2005) Endoscopic suturing without extracorporeal knots: a laboratory study. Gastrointest Endosc 62: 230–233
Kuhry E et al. (2004) Effect of laparoscopy on the immune system. Semin Laparosc Surg 11: 37–44
Sylla P et al. (2005) Immunological advantages of advanced laparoscopy. Surg Clin North Am 85: 1–18
NOSCAR website [www.noscar.org]
Acknowledgements
Charles P Vega, University of California, Irvine, CA, is the author of and is solely responsible for the content of the learning objectives, questions and answers of the Medscape-accredited continuing medical education activity associated with this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
About this article
Cite this article
Wagh, M., Thompson, C. Surgery Insight: natural orifice transluminal endoscopic surgery—an analysis of work to date. Nat Rev Gastroenterol Hepatol 4, 386–392 (2007). https://doi.org/10.1038/ncpgasthep0867
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1038/ncpgasthep0867
This article is cited by
-
Use of magnets in gastrointestinal surgery
Surgical Endoscopy (2019)
-
Force sensing in natural orifice transluminal endoscopic surgery
Surgical Endoscopy (2011)
-
Transgastric cecectomy in canine models: natural orifice transluminal endoscopic surgery (NOTES)
Surgical Endoscopy (2010)
-
Endoscopic Interventions for Weight Loss Surgery
Obesity (2009)
-
Evaluation for transvaginal and transgastric NOTES cholecystectomy in human and animal natural orifice translumenal endoscopic surgery
Journal of Hepato-Biliary-Pancreatic Surgery (2009)
