
Abstract
Background:
Obese women are reported to be at higher risk from gynecological cancers than nonobese women, yet these women are less likely to get cancer-screening tests. The specific factors that contribute to obese women not obtaining timely cancer screening have not been identified.
Objective:
To investigate the factors that contribute to lower rates of gynecological cancer screening as related to women's body size.
Design:
A purposeful sample of 498 White and African-American women with body mass index (BMI) from 25 to 122 kg/m2, including 60 women with BMI>55 kg/m2, was surveyed concerning access to gynecological cancer screening and potential barriers that could cause delay. Health care providers (N=129) were surveyed concerning their education, practices, and attitudes about providing care and gynecological cancer-screening tests for obese women.
Results:
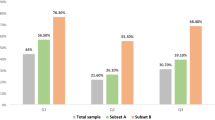
Obese women reported that they delay cancer-screening tests and perceive that their weight is a barrier to obtaining appropriate health care. The percent of women reporting these statements increased significantly as the women's BMI increased. Women with BMI>55 kg/m2 had a significantly lower rate (68%) of Papanicolaou (Pap) tests compared to others (86%). The lower screening rate was not a result of lack of available health care since more than 90% of the women had health insurance. Women report that barriers related to their weight contribute to delay of health care. These barriers include disrespectful treatment, embarrassment at being weighed, negative attitudes of providers, unsolicited advice to lose weight, and medical equipment that was too small to be functional. The percentage of women who reported these barriers increased as the women's BMI increased. Women who delay were significantly less likely to have timely pelvic examinations, Pap tests, and mammograms than the comparison group, even though they reported that they were ‘moderately’ or ‘very concerned’ about cancer symptoms. The women who delay care were also more likely to have been on weight-loss programs five or more times. Many health care providers reported that they had little specific education concerning care of obese women, found that examining and providing care for large patients was more difficult than for other patients, and were not satisfied with the resources and referrals available to provide care for them.
Conclusion:
Since the goal of preventive cancer screening is to improve health outcomes for all women and since obese women are at greater risk, strategies must be designed to reduce the weight barriers to these tests and improve the quality of the health care experience. Providers should receive specific training related to care of large women.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ . Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 2003; 348: 1625–1638.
Wee CC, McCarthy EP, Davis RB, Phillips RS . Screening for cervical and breast cancer: is obesity an unrecognized barrier to preventive care? Ann Intern Med 2000; 132: 697–704.
Fontaine K, Bartlett S . Access and use of medical care among obese persons. Obes Res 2000; 8: 403–406.
Flegal KM, Carroll MD, Ogden CL, Johnson CL . Prevalence and trends in obesity among US adults, 1999–2000. JAMA 2002; 288: 1723–1727.
Freedman DS, Khan LK, Serdula MK, Galuska DA, Dietz WH . Trends and correlates of class 3 obesity in the United States from 1990 through 2000. JAMA 2002; 288: 1758–1761.
McTigue KM, Harris R, Hemphill B, Lux L, Sutton S, Bunton AJ et al. Screening and interventions for obesity in adults: summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2003; 139: 933–949.
Taplin SH, Ichikawa L, Yood MU, Manos MM, Geiger AM, Weinmann S . Reason for late-stage breast cancer: absence of screening or detection, or breakdown in follow-up? J Natl Cancer Inst 2004; 96: 1518–1527.
Puhl R, Brownell K . Bias, discrimination, and obesity. Obes Res 2001; 9: 788–805.
Teachman BA, Brownell KD . Implicit anti-fat bias among health professionals: is anyone immune? Int J Obes Relat Metab Disord 2001; 25: 1525–1531.
Teachman B, Brownell K . Implicit anti-fat bias among health professionals: is anyone immune? Int J Obes Relat Metab Disord 2001; 25: 1525–1531.
Puhl RM, Brownell KD . Psychosocial origins of obesity stigma: toward changing a powerful and pervasive bias. Obes Rev 2003; 4: 213–227.
Rowland ML . Self-reported weight and height. Am J Clin Nutr 1990; 52: 1125–1133.
National Taskforce on the Prevention and Treatment of Obesity. Medical care for obese patients: advice for health care professionals. Am Fam Physician 2002; 65: 81–88.
U.S. Department of Health and Human Services. Healthy People 2010, 2nd edn. US Government Printing Office: Washington, DC, 2000.
Steptoe A, Kerry S, Rink E, Hilton S . The impact of behavioral counseling on stage of change in fat intake, physical activity, and cigarette smoking in adults at increased risk of coronary heart disease. Am J Public Health 2001; 91: 265–269.
Runkle C, Osterholm A, Hoban R, McAdam E, Tull R . Brief negotiation program for promoting behavior change: the Kaiser Permanente approach to continuing professional development. Educ Health (Abingdon) 2000; 13: 377–386.
Whitlock EP, Orleans CT, Pender N, Allan J . Evaluating primary care behavioral counseling interventions: an evidence-based approach. Am J Prev Med 2002; 22: 267–284.
Glasgow RE, Goldstein MG, Ockene JK, Pronk NP . Translating what we have learned into practice. Principles and hypotheses for interventions addressing multiple behaviors in primary care. Am J Prev Med 2004; 27: 88–101.
Foster GD, Wadden TA, Makris AP, Davidson D, Sanderson RS, Allison DB et al. Primary care physicians’ attitudes about obesity and its treatment. Obes Res 2003; 11: 1168–1177.
Kristeller JL, Hoerr RA . Physician attitudes toward managing obesity: differences among six specialty groups. Prev Med 1997; 26: 542–549.
Wadden TA, Anderson DA, Foster GD, Bennett A, Steinberg C, Sarwer DB . Obese women's perceptions of their physicians' weight management attitudes and practices. Arch Fam Med 2000; 9: 854–860.
Wiese HJ, Wilson JF, Jones RA, Neises M . Obesity stigma reduction in medical students. Int J Obes Relat Metab Disord 1992; 16: 859–868.
Wigton RS, McGaghie WC . The effect of obesity on medical students' approach to patients with abdominal pain. J Gen Intern Med 2001; 16: 262–265.
Sackett DL . The arrogance of preventive medicine. Can Med Assoc J 2002; 167: 363–364.
Getz L, Sigurdsson JA, Hetlevik I . Is opportunistic disease prevention in the consultation ethically justifiable? BMJ 2003; 327: 498–500.
Sarlio-Lahteenkorva S, Rissanen A, Kaprio J . A descriptive study of weight loss maintenance: 6 and 15 year follow-up of initially overweight adults. Int J Obes Relat Metab Disord 2000; 24: 116–125.
Acknowledgements
The research was supported by California Cancer Research Grant #99-00492V-10225 and the California Agricultural Experiment Station. We thank our many study participants for offering insights into their medical experiences, the California Black Women's Project, Michelle Soeffer, MS, for project management and data entry, and Mark Hudes, PhD, for statistical support.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Amy, N., Aalborg, A., Lyons, P. et al. Barriers to routine gynecological cancer screening for White and African-American obese women. Int J Obes 30, 147–155 (2006). https://doi.org/10.1038/sj.ijo.0803105
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijo.0803105
Keywords
This article is cited by
-
Weight stigma in healthcare settings: the experience of Arab and Jewish bariatric surgery candidates in Israel
Israel Journal of Health Policy Research (2024)
-
The impact of body mass index and physical disability on home-based anal self-sampling
Cancer Causes & Control (2024)
-
Obesity Stigma: Causes, Consequences, and Potential Solutions
Current Obesity Reports (2023)
-
Experiences of weight stigmatization in the Israeli healthcare system among overweight and obese individuals
Israel Journal of Health Policy Research (2022)
-
Weight stigma speaks Italian, too
Journal of Endocrinological Investigation (2022)
