
Abstract
OBJECTIVE: This study examines the relationship between obesity and foot structure in prepubescent children.
DESIGN: Field-based, experimental data on BMI (body mass index) and foot structure were collected for 431 consenting children from 18 randomly selected primary schools.
SUBJECTS: Of the 431 participants, 62 obese (BMI>95th percentile) and 62 non-obese (10th percentile<BMI>90th percentile) children (age=8.5±0.5 y) were selected.
MEASUREMENTS: Height and weight were measured to calculate BMI. Static weight-bearing footprints for the right and left foot of each subject were then taken using a pedograph to calculate the Footprint Angle and the Chippaux-Smirak Index as representative measures of the surface area of the foot in contact with the ground.
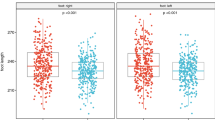
RESULTS: A significant difference was found between the Footprint Angle of the obese and non-obese subjects for both the left (t=3.663; P<0.001) and right (t=3.742; P<0.001) feet whereby obese subjects displayed a reduced angle. Chippaux–Smirak Index scores were also significantly different for both the left (t=−6.362; P<0.001) and right (t=−5.675; P<0.001) feet between the two subject groups where a greater score for the obese subjects was evident. A decreased footprint angle and an increased Chippaux–Smirak Index are characteristic of structural foot changes that have been associated with compromised foot function.
CONCLUSIONS: Excess body mass appears to have a significant effect on the foot structure of prepubescent children whereby young obese children display structural foot characteristics which may develop into problematic symptoms if excessive weight gain continues. Further investigation into possible consequences, particularly any effects on foot function, is warranted.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others
References
Lancashire J . More Americans of all ages are overweight. http://www.cdc.gov/nchswww/releases/97news/97news/fatmmwr.htm, 6 March 1997.
Hardcastle DM, Shrimptom S, Renigeris AS, Baptist Ed, Baur LA . Increasing prevalence of childhood obesity Med J Austral 1997 167: 342.
Norkin CC, Levangie PK . Joint structure and function, 2nd edn FA Davis: Philadelphia, PA 1992.
Cailliet R . Foot and ankle pain, 12th edn FA Davis: Philadelphia, PA 1980.
Wenger DR, Mauldin D, Speck G, Morgan D, Lieber RL . Corrective shoes and inserts as treatment for flexible flatfoot in infants and children J Bone Joint Surg 1989 71A: 800–810.
Donatelli R . The biomechanics of the foot and ankle. FA Davis: Philadelphia, PA 1990.
Hicks JH . The mechanics of the foot. I. The joints J Anat 1953 87: 345–357.
Kleiger B, Mankin HJ . A roentgenological study of the development of the calcaneus by means of a posterior tangential view J Bone Joint Surg 1961 43A: 961.
Davis PSW, Gregory J, White, A . Physical activity and body fatness in pre-school children Int J Obes 1995 19: 6–10.
National Health and Medical Research Council (NHMRC) . Acting on Australia's weight: a strategy for the prevention of overweight and obesity. Australian Government Publishing Service: Canberra 1997.
World Health Organisation . Obesity: preventing and managing the global epidemic Report of a WHO Consultation on Obesity (WHO/NUT/NCD/98.1) WHO: Geneva 1997.
Wilcken DEL, Lynch JF, Marshall MD, Scott RL, Wang XL . Relevance of body weight to apolipoprotein levels in Australian children Med J Austral 1996 164: 22–25.
National Health and Medical Research Council (NHMRC) . Statement on human experimentation. Australian Government Publishing Service: Canberra 1993.
Stamler J . Epidemic obesity in the United States Arch Intern Med 1993 153: 1040–1044.
Hammer LD, Kraemer HC, Wilson DM, Ritter PL, Dornbusch SM . Standard percentile curves of body-mass index for children and adolescents Am J Dis Child 1991 145: 259–263.
Wu KK . Foot orthoses. Williams &Wilkins: Baltimore, MD 1990.
Forriol F, Pascual J . Footprint analysis between three and seventeen years of age Foot Ankle 1990 11: 101–104.
Keppel G . Design and analysis. A research's handbook, 2nd edn Prentice-Hall England ChHs, New Jersey 1982.
Cavanagh PR, Rodgers MM . The arch index: a useful measure from footprints J Biomech 1987 20: 547–551.
Welton EA . The Harris & Beath footprint: interpretation and clinical value Foot Ankle 1992 13: 462–468.
Hennig EM, Staats A, Rosenbaum D . Plantar pressure distribution patterns of young school children in comparison to adults Foot Ankle 1994 15: 35–40.
Acknowledgements
We thank staff and students from the Wollongong Education District primary schools who consented to participate in this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Riddiford-Harland, D., Steele, J. & Storlien, L. Does obesity influence foot structure in prepubescent children?. Int J Obes 24, 541–544 (2000). https://doi.org/10.1038/sj.ijo.0801192
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijo.0801192
Keywords
This article is cited by
-
Children’s foot parameters and basic anthropometry — do arch height and midfoot width change?
European Journal of Pediatrics (2022)
-
Foot characteristics during walking in 6–14- year-old children
Scientific Reports (2020)
-
An investigation of the foot ankle joint mobility, muscle strength, and foot structure in adolescent with type 1 diabetes
International Journal of Diabetes in Developing Countries (2018)
-
The association between functional movement and overweight and obesity in British primary school children
Sports Medicine, Arthroscopy, Rehabilitation, Therapy & Technology (2013)
-
Four classes of physical fitness in German children and adolescents: only differences in performance or at-risk groups?
International Journal of Public Health (2013)
