
Abstract
Purpose
To describe the clinical and angiographic features of three cases of secondary syphilis in immunocompetent patients, which presented as acute posterior placoid chorioretinitis (APPC) to the ophthalmologist.
Methods
Interventional case series. The aetiology of the APPC was confirmed by serology to be secondary syphilis. Optical coherence tomography, electrophysiology, fundus fluorescein, and indocyanine green (ICG) angiography were performed at presentation and after resolution. Appropriate treatment for secondary syphilis was instituted in each patient.
Results
The clinical features, fundus fluorescein and ICG angiography, multifocal electroretinography (mfERG), and optical coherence tomography findings of APPC are described. All three patients had a satisfactory resolution of the APPC with improvement in visual acuity.
Conclusions
APPC in secondary syphilis can occur even in immunocompetent patients. A high index of suspicion is required for early diagnosis of this condition resulting in a good visual outcome with adequate treatment. mfERG and optical coherence tomography are useful in the diagnosis and follow-up of these patients.
Similar content being viewed by others

Introduction
Syphilitc acute posterior placoid chorioretinitis (APPC) has been recognized for a number of years and was thought to complicate syphilis in predominantly immunosuppressed patients.1 With its distinct features and the recent re-emergence of syphilis in the UK, it is becoming more important to recognize the disease early so that prompt treatment can be initiated. We present three recent cases of secondary syphilis in immunocompetent patients, which initially presented to the ophthalmologist. The rapid diagnosis of APPC allowed early recognition and treatment of the disease with good visual outcomes.
Case reports
Case 1
A 40-year-old female patient presented to the eye casualty with a 3-day history of reduced vision and floaters in both eyes. Before this she had a 3-week history of sore throat and hoarseness of voice. She was a known intravenous drug abuser and smoker. Further questioning revealed a history of being sexually assaulted 6 months before presentation. Her visual acuities were 1/60 in both eyes, visual fields were markedly constricted, and colour vision was impaired in both eyes. There were bilateral fine keratic precipitates and 2+ and 3+ cells in the right and left anterior chambers, respectively. Both pupils reacted sluggishly to light and there were cells in the vitreous with a binocular indirect ophthalmoscopy score of 1 in the right eye and 3 in the left eye. Fundus examination showed an area of elevated chorioretinal pallor within the temporal arcades in both eyes (Figure 1a). There were multiple bilateral inferior retinal infiltrates. Fundus fluorescein angiogram (FFA) showed mottled hyper- and hypofluorescence in the area of retinal pallor in both eyes (Figure 1b and c). There was no leakage from the disc in either eye. On electrophysiological testing, she had reduced flash electroretinograms (ERG) and VEP in both eyes, absent pattern VEP in both eyes, absent pattern ERG in the right eye, and reduced pattern ERG in the left eye.

Patient 1: (a) colour fundus photograph of the right eye at presentation showing the large yellowish elevated area temporal to the disc; (b) early and (c) late phase of the FFA showing mottled hyper- and hypofluorescence in the area of pallor with late leak of fluorescein; (d) colour fundus photograph of the right eye after resolution of the lesion, showing retinal pigment epithelial hypertrophy and atrophy at the macula.
General physical examination revealed laryngitis, bilateral shotty inguinal lymphadenopathy, and multiple chronic ulcers on the right leg secondary to intravenous drug abuse. She also had some abnormalities of the vulva that were consistent with healing patches of secondary syphilis.
Full blood count, urea, and electrolytes and liver function tests were normal. Blood cultures, hepatitis B and C serology, and HIV tests were negative. Rapid plasma reagin was positive (RPR+8) and Treponema pallidum haemagglutination test was also positive (TPHA+32).
The patient, who was allergic to penicillin, was treated with oral doxycycline 100 mg b.d. for a period of 3 weeks. Over the period of treatment, visual acuities progressively improved to 6/9 in the right eye and 6/12 in the left eye. The anterior and posterior segment inflammation resolved leaving mottled areas of retinal pigment epithelial hypertrophy at the macula and peripheral retina in both eyes (Figure 1d). The colour vision and visual fields continued to be markedly impaired when she was lost to follow-up 2 months after presentation.
Case 2
A 40-year-old homosexual man presented with a painless reduction of vision in his right eye. He had experienced an episode of photopsia in this eye 3 days earlier, which was followed by gradual blurring of his central vision. He was also aware of similar symptoms and a blurred patch in the paracentral visual field of his left eye. Past ophthalmic history was unremarkable. Of note, he had developed a rash, resembling lichen planus, in the previous 2 weeks affecting his arms, legs, and genitals. There was no history of urethral discharge. Over the last 2 weeks he had also developed painful mouth ulcers. There was no history of intravenous drug usage.
On examination, visual acuity was 6/60 OD, 6/9 OS. The anterior segments were quiet with normal intraocular pressures. He had bilateral vitritis. Fundus examination revealed a raised creamy yellow choroidal lesion at the right macula and a similar slightly elevated lesion superior to the left fovea (Figure 2a and b). Both optic discs appeared swollen. OCT scans were performed through these lesions and showed increased thickening of the neuroretina and underlying layers.

Patient 2: (a) colour fundus photograph of the right eye at presentation showing the raised creamy yellow choroidal lesion at the right macula and (b) a similar slightly elevated lesion superior to the left fovea. (c, d) Colour photographs after resolution of the lesions demonstrating mottling of the maculae in both eyes.
A provisional diagnosis of syphilitic APPC was made and a genitourinary medicine opinion was sought. He was admitted and given a stat dose of 2.4 mega unit of intramuscular benzathine benzylpenicillin with 40 mg oral prednisolone cover. A lumbar puncture was performed. Analysis of both cerebrospinal fluid and serum was positive for active syphilis infection (Treponema pallidum particle agglutination test (TPPA), Syphilis Total antibody enzyme immunoassay and RPR test positive). He was HIV negative.
After 1 week, his vision had improved to 6/12 OD and 6/9 OS. Clinically, the choroidal lesions were less prominent and there was moderate disc swelling and hyperaemia. In view of his good response to treatment, he was given a further 18 days of intravenous benzylpenicillin.
By the end of this course, his vision continued to improve to 6/6 bilaterally. Fundus examination showed marked improvement of the disc swelling with mottling of the maculae in both eyes (Figure 2c and d). Repeat OCT scans were also performed at this time and showed restoration of the normal chorioretinal architecture.
Case 3
A 55-year-old male patient presented with a 3-week history of floaters and photopsiae followed by a 3-day history of reduced vision in the right eye. Four months before presentation, the patient had experienced an episode of skin rashes with painful joints and deafness in the right ear, all of which had been attributed to a viral illness. He had multiple tattoos and evidence of body piercing.
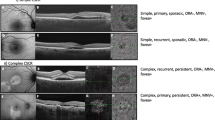
On examination, his visual acuities were counting fingers OD, 6/9 OS. There was a right afferent pupillary defect, with fine keratic precipitates+cells in the anterior chamber and normal intraocular pressures. There was right vitritis with inferior snowballs and peripheral retinal haemorrhages. Macular oedema with surrounding creamy elevated chorioretinal pallor was noted in the right eye (Figure 3a). Examination of the left eye showed mild inflammation in the anterior chamber. FFA and indocyanine green (ICG) findings are as shown in figure (Figure 3b–d) and OCT confirmed the presence of subretinal fluid at the right macula (Figure 3e). Examination by the ENT surgeons revealed bilateral symmetrical high-frequency hearing loss.

Right eye of patient 3 at presentation: (a) colour fundus photograph showing the raised creamy yellow choroidal lesion and retinal haemorrhages; (b) early and (c) late phase of the FFA showing early hyper- and hypofluorescence and late leak; (d) ICG of the right eye showing hyperfluorescent spots nasal to the disc; and (e) OCT demonstrating the presence of subretinal fluid.
A provisional diagnosis of syphilitic APPC was made and the patient was initially treated with oral tetracycline 2 g/day with oral prednisolone 20 mg and topical steroids, while awaiting syphilis serology. Syphilis serology was positive on both serum (VDRL>16, TPPA>128) and CSF (VDRL and TPPA positive). HIV testing was negative.
The patient was then treated in collaboration with the genitourinary physicians with a 21-day course of 1.2 mega units of intramuscular procaine penicillin with probenacid. Two weeks after initiating treatment, his macula was dry as shown by OCT (Figure 4e), but right visual acuity remained at 1/60. His right visual acuity had improved to 6/9 by 6 weeks. FFA and ICG findings at 3 months are shown in figure (Figure 4b–d).

(a–e) Colour photograph, FFA and ICG, and OCT of the right eye of patient 3 after resolution of symptoms showing return to normal chorioretinal architecture.
This patient also had serial multifocal electroretinograms (mfERG) during the course of his illness. One week after presentation when the visual acuity was 6/36 OD and 6/6 OS, the mfERG was extinguished in the right eye. Two weeks later, the right mfERG and visual acuity remained unchanged. Three months later, his vision was 6/9 OD and the right mfERG had improved to approximately half the amplitude of the left eye responses. At 7 months his vision had continued to improve to 6/6 OD and the right mfERG had recovered to almost normal for the peripheral stimuli and 65% of normal for the central stimuli. Figure 5 shows the time lag between improvement in mfERG and improvement in visual acuity over time in patient 3.

Improvement in amplitude of central zone mfERG (peak-to-trough N1) and visual acuity (logmar) over time in patient 3.
Discussion
Chorioretinitis has been reported to be the predominant uveitic pattern in patients with syphilitic posterior uveitis and may be localized or diffuse.2 The localized posterior placoid type of chorioretinitis has been reported to be associated with bilateral large solitary placoid pale yellowish subretinal lesions that show evidence of central fading and coarsely stippled hyperpigmentation of the retinal pigment epithelium.1 FFA shows early hypofluorescence with a leopard spot pattern of hypo- and hyperfluorescence in the faded part of the lesions with late retinal pigment epithelial staining.
Gass et al1 have described syphilitic APPC in six patients in 1990. Three of the six patients were immunocompromised and were positive for HIV. It was postulated that the clinical picture of APPC may be secondary to the immunocompromised status of the patient.1 This was further substantiated by Zamani and Garfinkel,3 who reported the development of placoid lesions in an immunocompetent patient with ocular syphilis only after exposure to corticosteroids without antitreponemal treatment. All our patients were immunocompetent and HIV negative, nevertheless they all developed the typical lesions of APPC with positive serology for syphilis.
Gass et al1 postulated that, in secondary syphilis, the widely disseminated spirochaetes may also be present in the inflammation around the retinal pigment epithelium in the placoid lesions of acute syphilitic posterior placoid chorioretinitis. Another explanation was that the clinical appearance was due to deposition of soluble immune complexes.4 The development of acute syphilitic posterior placoid chorioretinitis in all our immunocompetent patients suggests that the clinical appearance of these lesions does not necessarily depend on the immune status of the patient, but may be part of the natural course of the disease. The FFA findings in patients 1 and 3 were similar to the previously described FFA features in APPC.1 ICG anomalies of ocular syphilis include multiple scattered hyperfluorescent spots in the midperiphery during the late phase of the angiogram as seen in the ICG of patient 3 or late hyperfluorescence of the retinal arteries and veins.5 OCT and mfERG features of syphilitic APPC have not been described previously. Patient 3 had serial mfERGs that showed that there is a delay in improvement of mfERG when compared to the improvement in visual acuity. These changes in the mfERG suggest that the outer retina (photoreceptors) are significantly affected by the chorioretinitis furthermore, the recovery of the photoreceptors is significantly delayed compared to the apparent anatomical recovery.
Although ocular syphilis is a rare disease, there has been a recent resurgence in the incidence of syphilis cases with a 158% increase in reported positive cases from Scotland in 2004, as compared to 2003.6 A high index of suspicion must be maintained in order to identify possible cases of syphilis among the numerous forms of uveitis that present in the ophthalmology clinic, particularly as all three cases in this report presented with their ocular features before the diagnosis of systemic syphilis.
References
Gass JD, Braunstein RA, Chenoweth RG . Acute syphilitic posterior placoid chorioretinitis. Ophthalmology 1990; 97: 1288–1297.
Villanueva AV, Sahouri MJ, Ormerod LD, Puklin JE, Reyes MP . Posterior uveitis in patients with positive serology for syphilis. Clin Infect Dis 2000; 30: 479–485.
Zamani M, Garfinkel RA . Corticosteroid-induced modulation of acute syphilitic posterior placoid chorioretinitis. Am J Ophthalmol 2003; 135: 891–894.
de Souza EC, Jalkh AE, Trempe CL, Cunha S, Schepens CL . Unusual central chorioretinitis as the first manifestation of early secondary syphilis. Am J Ophthalmol 1988; 105: 271–276.
Mora P, Borruat FX, Guex-Crosier Y . Indocyanine green angiography anomalies in ocular syphilis. Retina 2005; 25: 171–181.
Wallace LW, Goldberg AD . Increase in reported syphilis infections in Scotland in 2004. Eurosurveillance 2005; 10: 050728.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Joseph, A., Rogers, S., Browning, A. et al. Syphilitic acute posterior placoid chorioretinitis in nonimmunocompromised patients. Eye 21, 1114–1119 (2007). https://doi.org/10.1038/sj.eye.6702504
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702504
Keywords
This article is cited by
-
Acute syphilitic posterior placoid chorioretinitis: when the great mimicker cannot pretend any more; new insight of an old acquaintance
Journal of Ophthalmic Inflammation and Infection (2022)
-
Ocular syphilis with optic disc neovascularization treated with bevacizumab evaluated by OCT angiography and electroretinography
Journal of Ophthalmic Inflammation and Infection (2020)
-
Multimodal imaging patterns of posterior syphilitic uveitis: a review of the literature, laboratory evaluation and treatment
International Ophthalmology (2020)
-
Multi-modal imaging and anatomic classification of the white dot syndromes
International Journal of Retina and Vitreous (2017)
-
Multimodal imaging analyses of hyperreflective dot-like lesions in acute syphilitic posterior placoid chorioretinopathy
Journal of Ophthalmic Inflammation and Infection (2017)
