
Abstract
Objective: Faecal bifidobacteria and lactobacilli, perceived as exerting health-promoting properties, may be increased by ingestion of high-dose lactulose in humans. The effects of low and well-tolerated doses of lactulose are not well known. The aim of the study was to assess the effects of prolonged low-dose lactulose administration on faecal bifidobacteria and selected metabolic indexes potentially involved in colonic carcinogenesis.
Subjects and methods: In all, 16 healthy volunteers were included in this controlled, randomised, double-blind, parallel group trial. Participants ingested lactulose or placebo (sucrose) at a dose of 5 g b.i.d. for 6 weeks. Stools were regularly collected at baseline (d0), and after 3 (d21) and 6 (d42) weeks of sugar ingestion. Tolerance was evaluated using a daily chart.
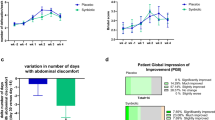
Results: Faecal bifidobacterial counts were higher in lactulose than in sucrose group (P=0.03). Lactulose ingestion led to a significant increase in faecal bifidobacteria counts from d0 to d21 and d42 ((m±s.e.m.) 8.25±0.53, 8.96±0.40 and 9.54±0.28 log colony-forming units/g wet wt (CFU/g), respectively (P=0.048)). Placebo ingestion did not lead to any faecal bifidobacterial count change. Total anaerobes, Lactobacillus and pH were not significantly changed throughout the study in the two groups. Neither faecal bile acids nor neutral sterols were modified by lactulose. Excess flatus was more common in the lactulose group (P=0.03), but was very mild. Bloating and borborygmi did not differ between both the groups.
Conclusions: A measure of 10 g lactulose/day increases faecal bifidobacterial counts, and lactulose fulfils the criteria requested to be considered as a prebiotic.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others


References
Andrieux C, Gadelle D, Leprince C & Sacquet E (1989): Effects of some poorly digestible carbohydrates on bile acid bacterial transformations in the rat. Br. J. Nutr. 62, 103–119.
Ballongue J, Schumann C & Quignon P (1997): Effects of lactulose and lactitol on colonic microflora and enzymatic activity. Scand. J. Gastroenterol. Suppl. 222, 41–44.
Beerens H (1991): Detection of bifidobacteria by using propionic acid as a selective agent. Appl. Environ. Microbiol. 57, 2418–2419.
Berge Henegouwen GP, van der Werf SD & Ruben AT (1987): Effect of long term lactulose ingestion on secondary bile salt metabolism in man: potential protective effect of lactulose in colonic carcinogenesis. Gut 28, 675–680.
Bouhnik Y, Pochart P, Marteau P, Arlet G, Goderel I & Rambaud JC (1992): Fecal recovery in humans of viable Bifidobacterium sp ingested in fermented milk. Gastroenterology 102, 875–878.
Buddington RK, Williams CH, Chen SC & Witherly SA (1996): Dietary supplement of neosugar alters the fecal flora and decreases activities of some reductive enzymes in human subjects. Am. J. Clin. Nutr. 63, 709–716.
Challa A, Rao DR, Chawan CB & Shackelford L (1997): Bifidobacterium longum and lactulose suppress azoxymethane-induced colonic aberrant crypt foci in rats. Carcinogenesis 18, 517–521.
Gibson GR, Roberfroid MB (1995): Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. J. Nutr. 125, 1401–1412.
Hennigan TW, Sian M, Matthews J & Allen-Mersh TG (1995): Protective role of lactulose in intestinal carcinogenesis. Surg. Oncol. 4, 31–34.
Hoffmann K, Bircher J (1969): Changes in the bacterial population of the intestine following lactulose administration. Schweiz. Med. Wochenschr. 99, 608–609.
Nagengast FM, Hectors MP, Buys WA & van Tongeren JH (1988): Inhibition of secondary bile acid formation in the large intestine by lactulose in healthy subjects of two different age groups. Eur. J. Clin. Invest. 18, 56–61.
Nair PP (1988): Role of bile acids and neutral sterols in carcinogenesis. Am. J. Clin. Nutr. 48, 768–774.
Owen RW (1997): Faecal steroids and colorectal carcinogenesis. Scand. J. Gastroenterol. Suppl. 222, 76–82.
Riggio O, Varriale M, Testore GP, Di Rosa R, Di Rosa E, Merli M, Romiti A, Candiani C & Capocaccia L (1990): Effect of lactitol and lactulose administration on the fecal flora in cirrhotic patients. J. Clin. Gastroenterol. 12, 433–436.
Salminen S, Salminen E (1997): Lactulose, lactic acid bacteria, intestinal microecology and mucosal protection. Scand. J. Gastroenterol. Suppl. 222, 45–48.
Singh J, Rivenson A, Tomita M, Shimamura S, Ishibashi N & Reddy BS (1997): Bifidobacterium longum, a lactic acid-producing intestinal bacterium inhibits colon cancer and modulates the intermediate biomarkers of colon carcinogenesis. Carcinogenesis 18, 833–841.
Terada A, Hara H, Kataoka M & Mitsuoka T (1992): Effect of lactulose on composition and metabolic activity of the human fecal flora. Microb. Ecol. Health Dis. 5, 43–50.
Tuohy KM, Ziemer CJ, Klinder A, Knöbel Y, Pool-Zobel BL & Gibson GR (2002): A human volunteer study to determine the prebiotic effects of lactulose powder on human colonic microbiota. Microb. Ecol. Health Dis. 14, 165–173.
Author information
Authors and Affiliations
Contributions
Guarantor: Y Bouhnik.
Contributors: YB carried out the data checking and was responsible for writing the manuscript. AA carried out data analysis and assisted in the preparation of the manuscript. JFA was involved in the data checking and in assisting manuscript preparation. RM was responsible for neutral sterol and bile acids analysis. FD and BF participated for the design of the study and in writing the manuscript.
Corresponding author
Rights and permissions
About this article
Cite this article
Bouhnik, Y., Attar, A., Joly, F. et al. Lactulose ingestion increases faecal bifidobacterial counts: A randomised double-blind study in healthy humans. Eur J Clin Nutr 58, 462–466 (2004). https://doi.org/10.1038/sj.ejcn.1601829
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejcn.1601829
Keywords
This article is cited by
-
Review of history and mechanisms of action of lactulose (4-O-β-D-Galactopyranosyl-β-D-fructofuranose): present and future applications in food
Journal of Food Science and Technology (2024)
-
Bifidobacterium response to lactulose ingestion in the gut relies on a solute-binding protein-dependent ABC transporter
Communications Biology (2021)
-
Lactulose drives a reversible reduction and qualitative modulation of the faecal microbiota diversity in healthy dogs
Scientific Reports (2019)
-
Lactulose: a prebiotic, laxative and detoxifying agent
Drugs & Therapy Perspectives (2017)
-
Effect of lactic acid bacteria on intestinal E. coli in Caenorhabditis elegans
Food Science and Biotechnology (2015)
