
Abstract
Objective: We evaluated the adequacy of nutrient intake in comparison with the Indonesian Estimated Average Requirement (EARs) among pregnant Indonesian women and explain the short-term effect of economic crisis on nutrient intake and iron status.
Design: Cross-sectional study.
Setting: Purworejo District, Central Java, located 60 km west of Yogyakarta Province, Indonesia.
Subjects: During the period from 1996 to 1998, up to six 24 h recalls were performed during the second trimester of pregnancy among 450 women. Nutrient intake and iron status was evaluated in relation to date of data collection relative to the economic crisis that emerged in August 1997. A computer program (Inafood) was developed to calculate nutrient intake.
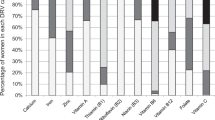
Results: Forty percent of the pregnant women were at risk of inadequate intake of energy and protein, and 70% were at risk of inadequate intake of vitamin A, calcium and iron even before the crisis. Our results also demonstrate an effect of short-term economic crisis on nutrient intake and iron status. When the crisis emerged, urban poor experienced a decrease in intake of most nutrients. During the crisis, rich women experienced a significant decrease in fat (P<0.05). Negative changes in fat density during crisis were experienced by the rich and the rural, poor, and access to rice field subgroups (P<0.01). A significant increase in carbohydrate densities was seen for the rich and rural, poor, and access to rice fields groups (P<0.05). Urban poor experienced decreased serum ferritin concentration (P<0.05), whereas rich women experienced a significant increase (P<0.05).
Conclusions: Urban poor and rural poor landless women were most directly affected by the emerging economic crisis.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Achadi, EL, Hansell, MJ, Sloan, NL & Anderson, MA (1995). Women's nutritional status, iron consumption and weight gain during pregnancy in relation to neonatal weight and length in West Java, Indonesia. Int. J. Gyn. Obstet., 48, (Suppl) S110–S119.
Blundell, JE, Green, S & Burley, V (1994). Carbohydrates and human appetite. Am. J. Clin. Nutr., 59, (Suppl) 728S–734S.
Blundell, JE, Lawton, CL, Cotton, JR & Macdiarmid, JI (1996). Control of human appetite: implications for the intake of dietary fat. A. Rev. Nutr., 16, 285–319.
Booth, SL, Johns, TA & Kulnlein, HV (1997). Culture, Environment, and Food to Prevent Vitamin A Deficiency in the Complexities of Understanding Vitamin A in Food and Diets: the Problem, ed. HV Kuhnlein & GH Pelto Quebec: Centre for Nutrition and the Environment of Indigenous Peoples
Briawan, D & Hardiansyah, (1990). Penilaian dan Perencanaan Konsumsi Pangan, Bogor: Gizi Masyarakat-Institut Pertanian Bogor
Cook, JD & Skikne, BS (1989). Iron deficiency definition and diagnosis. J. Intern. Med., 226, 349–355.
Department of Information (1996). Republic of Indonesia. Indonesia 1996., Jakarta: Promosi Citra Indonesia
de Pee, S & Bloom, M (1999). 24-VASQ Method for Estimating Vitamin A Intake (24-hour Vitamin A Semi-quantitative), DraftJakarta: Helen Keller International (HKI) Asia Pacific Regional Office
Development and Planning Board of District Level & Central Bureau of Statistics (1999). Purworejo Dalam Angka 1998 (Purworejo in Figures 1998), Purworejo: DPBD & CBS
FAO/WFP Special Report (2000). Global Information and Early Warning System on Food and Agriculture, FAO/WFP crop and food supply assessment mission to Indonesia. Available at: www.fao.org/giews/english/alertes/1999/srins994.htm(accessed 9 September 2000)
Gibson, RS & Huddle, JM (1998). Suboptimal zinc status in pregnant Malawian women: its association with low intakes of poorly available zinc, frequent reproductive cycling and malaria. Am. J. Clin. Nutr., 67, 702–709.
Hansen, RG & Wyse, BW (1980). Expression of nutrient allowances per 1000 kilocalories. J. Am. Diet. Assoc., 76, 223–227.
Hartini, TNS, Winkvist, A, Lindholm, L, Stenlund, H, Surjono, A & Hakimi, M (2002). Energy intake during economic crisis depends on initial wealth and access to rice fields: the case of pregnant Indonesian women. Health Policy, Jul61, (1) 57–71.
Helen Keller International (1999). The Posible Impact of the Indonesian Crisis on Maternal and Child Survival through Micronutrient Deficiencies: Trends Toward Higher Rates of Malnutrition in Urban Slums, Jakarta: HKI
Huddle, JM, Gibson, R & Cullinan, TR (1998). Is zinc a limiting nutrient in the diets of rural pregnant Malawian women?. Br. J. Nutr., 79, 257–265.
Hunt, IF, Murphy, NJ, Martner-Hewes, PM, Faraji, B, Swendseid, ME, Reynolds, RD, Sanches, A & Meijia, A (1987). Zinc, vitamin B-6 and other nutrients in pregnant women attending prenatal clinics in Mexico. Am. J. Clin. Nutr., 46, 563–569.
Institute of Medicine (1990). Subcommittees on Nutritional Status and Weight Gain During Pregnancy and Dietary Intake and Nutrient Supplements During Pregnancy, Committee on Nutrition During Pregnancy and Lactation, Food and Nutrition Board. Nutrition During Pregnancy: Part I, Weight Gain; Part II, Nutrient Supplements, Washington, DC: National Academy Press
Kardjati, S, Kusin, JA & Renqvist, UH (1994). Nutrition during Pregnancy in Maternal and Child Nutrition in Madura, Indonesia, Netherlands: The Netherlands Royal Tropical Institute
Kodyat, BA, Mukrie, N, Latief, D, Alhabsyi, A & Palupi, L (1996). Indonesian Weaning Food Program (Lesson Learned), Paper in the International Workshop on infant and young child feeding. Surabaya, 14–18 January
Ladipo, OA (2000). Nutrition in pregnancy: mineral and vitamin supplements. Am. J. Clin. Nutr., 72, (Suppl) 280S–290S.
Latief, D, Harianto, B & Kartono, J (1997). Penanggulangan kekurangan energi kronis pada ibu hamil dengan pemberian makanan tambahan. Gizi Indonesia, 12, 20–30.
Latief, D, Atmarita,, Minarto,, Johari, A & Tilden, R (2000). The tendency of household food consumption before and during the crisis in Indonesia. In:Proceedings, Prosiding Widya Karya Nasional Pangan dan Gizi VI (National Symposium on Food and Nutrition), 29 February–2 March Jakarta: LIPI
Mahmud, MK, Slamet, DS, Apriyanto, RR & Hermana, (1990). Komposisi Zat Gizi Pangan Indonesia, Jakarta: Dit Bina Gizi Masyarakat dan Pusat Penelitian dan Pengembangan Gizi
Ministry of Health (1995). Nutritional Guidelines for Indonesia (Basic Messages), Jakarta: Directorate of Community Nutrition, MOH
Ministry of Health (1998). Pedoman penanggulangan anemi gizi untuk remaja putri dan wanita usia subur, Jakarta: Dit. Bina Gizi Masyarakat, MOH
Ministry of Health, WHO (2000). National Plan of Action on Food and Nutrition 2001–2005, Jakarta: MOH & WHO
Muhilal, (2002). (Inaugural speech). Peran gizi dalam meningkatkan kualitas sumber daya manusia: Telaah dari aspek biokimia gizi hingga pedoman gizi seimbang. Pidato pengukuhan jabatan Guru Besar dalam ilmu gizi, Bandung: Universitas Padjadjaran
Muhilal,, Jalal, F & Hardiansyah, (1998). Angka Kecukupan yang Dianjurkan (RDA). Prosiding Widya Karya Nasional Pangan dan Gizi VI (Proceedings of National Symposium on Food and Nutrition), 17–20 February Jakarta: LIPI
Mukrie, NA, Chatijah, S, Mosoar, S, Alhabsyi, A, Djasmidar,, Bernadus, HA, Mahmud, MK, Hermana,, Dewi, SS, Rossi, RA, Soebagyo, S & Dedy, M (1995). Daftar Komposisi Zat Gizi Pangan Indonesia, Jakarta: Dirjen Binkesmas Dit Bina Gizi Masyarakat, Pusat Penelitian dan Pengembangan Gizi
National Academy of Sciences (1997). Dietary Reference Intakes: Calcium, Phosporus, Magnesium, Vitamin D and Fluoride, Food and Nutrition Board, Institute of Medicine Washington, DC: National Academy Press
National Development Planning Agency (2000). Indonesia's social safety nets, programs and safeguarding activities. Available at: www.pin-jps.or.id/data/publikasi/JPS-English1.htm (accessed 16 May 2000)
National Research Council (1989). Recommended Dietary Allowances, 10th edn Washington, DC: National Academy Press
Nurdiati, DS, Hakimi, M, Wahab, A & Winkvist, A (1998). Concurrent prevalence of cronic energy deficiency and obesity among women in Purworejo, Central Java, Indonesia. Food Nutr. Bul., 19, (4) 321–333.
Panwar, B & Punia, D (1998). Nutrient intake of rural pregnant women of Haryana State, Northern India: relationship between income and education. Int. J. Food Sci. Nutr., 49, 391–395.
Persson, V, Winkvist, A, Hartini, TNS, Greiner, T, Hakimi, M & Stenlund, H (2001). Variability in nutrient intakes among pregnant women in Indonesia: Implications for the design of epidemiological studies using the 24-h recall method. J. Nutr., 131, 325–330.
Prentice, A, Lasley, MA, Shaw, J, Hudson, GJ, Day, KC, Jarjou, LM, Dibba, B & Paul, A (1993). The calcium and phosphorus intakes of rural Gambian women during pregnancy and lactation. Br. J. Nutr., 69, 885–896.
Purworejo District Health Office (2000). Profil Kesehatan Kabupaten Purworejo (Purworejo District Health Profile) 1999, Purworejo: District Health Office
Rad, AH, Omidvar, N, Mabmood, M, Kolahdooz, F & Amini, M (1998). Dietary intake, anthropometry and birth outcome of rural pregnant women in two Iranian Districts. Nutr. Res., 18, (9) 1469–1482.
Rolls, BJ & Hammer, VA (1995). Fat, carbohydrate, and the regulation of energy intake. Am. J. Clin. Nutr., 62, (Suppl) 1086S–1095S.
Schneeman, BO (2001). Carbohydrate: friend or foe? Summary of research needs. J. Nutr., 131, 2764S–2765S.
Sen, A (1997). Poverty and Famines: an Essay on Entitlement and Deprivation, New York: Clarendon Press
Siong, TE, Noor, MI, Azudin, MN & Idrus, K (1988). Nutrient Composition of Malaysian Food (Komposisi zat dalam makanan Malaysia), Malaysia: ASEAN Food habits Project–National Sub Committee on Protein, Food Habits Research and Development
Soekirman,, Tarwotjo, I, Jus'at, I, Sumodiningrat, G & Djalal, F (1992). Economic Growth, Equity and Nutritional Improvement in Indonesia, United Nations, ACC/SCN
Suara Merdeka, (1998). Harga bahan pokok melonjak, Pasar Rejowinangun sepi, Kamis, 8 January
Suharno, D, West, CE, Muhilal,, Logman, MHGM, Waart, FGD, Karyadi, D & Hautvast, GAJ (1993). Cross-sectional study on the iron and vitamin A status of pregnant women in West Java, Indonesia. Am. J. Clin. Nutr., 56, 988–993.
Sumarno, I, Latinulu, S & Saraswati, E (1997). Food consumption pattern of households in Indonesia. Gizi Indonesia, 22, 39–61.
Sundararaj, R & Pereira, SM (1973). Diets of pregnant women in South Indian Community. Trop. Geogr. Med., 25, 381–386.
Vitolo, MR, Gama, CM, Kondo, MR, Barrere, APN & Nobrega, FJC (1997). Food intake of pregnant adolescent women. Ann. NY Acad. Sci., 817, 386–388.
Warta kesehatan perkotaan (1992). Masalah gizi di daerah perkotaan, no. 0081–2.
Wasito, E, Pritasari,, Susilowati, D, Iswarawati, DN, Schultink, W & Gross, R (2001). Temporary stability of Urban food and nutrition security: the East Jakarta Study. Asia Pasific. J. Clin. Nutr., 10, (Suppl) S29–S33.
Whiteford, LM (1993). Child and maternal health and international economic policies. Soc. Sci. Med., 37, (11) 1391–1400.
Willett, WC, Howe, GR & Kushi, LH (1997). Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr., 6, (Suppl) 1220S–1228S.
Wilopo, SA (2001). Community Health and Nutrition Research Laboratories (CHN-RL), Faculty of Medicine, Gadjah Mada University: Key Issues on the Research Design, Data Collection and Management, Available at: www.chnrl.org/survaillance/page.htm (accessed 2 November 2001)
Winkvist, A, Persson, V & Hartini, TNS (2001). Under reporting of energy intake is less common among pregnant women in Indonesia. Publ. Hlth. Nutr., Aug5, (4) 523–529.
World Bank (2000). GNP per Capita 1998. Atlas Method and PPP, Available at: www.worldbank.org/databytop/GNPPC.pdf (accessed 21 May 2000)
Yip, R & Ramakrishnan, U (2002). Experiences and challenges in developing countries. J. Clin. Nutr., Apr132, (4 Suppl) 827S–830S.
Acknowledgements
We would like to thank all the women in Purworejo District who participated in the study and the staff of CHN-RL. We would also like to thank the following organisations for funding the project: Sida/SAREC (the Swedish International Development Authority/the Swedish Agency for Research Cooperation in Developing Countries), Mother Care, John Snow Inc., Washington, DC, USA, UNICEF, Jakarta, Indonesia, and STINT (the Swedish Foundation for International Cooperation in Research and Higher Education) and the World Bank through the Community Health and Nutrition Development Project of the Ministry of Health, Indonesia (IBRD Loan no. 3550-IND).
Author information
Authors and Affiliations
Contributions
Guarantor: TNS Hartini.
Contributors: A Winkvist, L Lindholm, H Stenlund, DS Nurdiati, A Surjono.
Corresponding author
Rights and permissions
About this article
Cite this article
Hartini, T., Winkvist, A., Lindholm, L. et al. Nutrient intake and iron status of urban poor and rural poor without access to rice fields are affected by the emerging economic crisis: the case of pregnant Indonesian women. Eur J Clin Nutr 57, 654–666 (2003). https://doi.org/10.1038/sj.ejcn.1601595
Received:
Revised:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejcn.1601595
Keywords
This article is cited by
-
Rethinking the measurement of food security: from first principles to best practice
Food Security (2013)
