
Abstract
Objectives: (a) to explore the relationship between waist circumference and certain cardiovascular risk factors in a group of girls; and (b) to assess the clinical relevance of waist circumference in identifying girls with higher cardiovascular risk across puberty.
Subjects and methods: One-hundred and fifty-five overweight or obese girls aged 5–16 y were recruited. Overweight and obesity were defined on the basis of BMI, according to Cole.
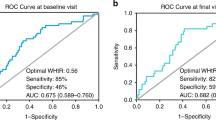
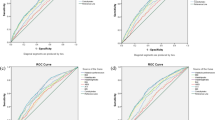
Results: Waist circumference was significantly correlated with plasma insulin (r=0.43; P<0.001), systolic blood pressure (r=0.22; P=0.007) and IRHOMA (r=0.40; P<0.001). A multivariate linear correlation analysis showed that, when adjusted for age and Tanner stage, waist circumference was significantly associated with plasma insulin (r2=0.23; P<0.01), IRHOMA (r2=0.17; P<0.02), systolic and diastolic blood pressure (r2=0.20; P=0.006 and r2=0.32; P<0.001, respectively). A logistic regression analysis, using IRHOMA as the dependent variable, showed that waist circumference was a significant independent risk factor of insulin resistance (IRHOMA≥2.6) in this group of girls (OR 1.10; 95% CI 1.03–1.18; P=0.003), independently of their age and Tanner stage.
Conclusions: Waist circumference of these girls was independently associated with certain cardiovascular risk factors, in particular insulin resistance and diastolic blood pressure, independently of age and Tanner stage. Thus suggesting that waist circumference may be reasonably included in clinical practice as a simple tool that may help to identify sub-groups of obese girls at higher metabolic risk across puberty.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Amiel, SA, Sherwin, RS, Simonson, DC, Lauritano, AA & Tamborlane, WV (1986). Impaired insulin action in puberty. N. Engl. J. Med., 315, 215–219.
Bonora, E, Targher, G, Alberiche, M, Bonadonna, RC, Saggiani, F, Zenere, MB, Monauni, T & Muggeo, M (2000). Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity: studies in subjects with various degrees of glucose tolerance and insulin sensitivity. Diabetes Care, 23, 57–63.
Caprio, S, Bronson, M, Sherwin, RS, Rife, F & Tamborlane, WV (1996a). Co-existence of severe insulin resistance and hyperinsulinaemia in pre-adolescent obese children. Diabetologia, 39, 1489–1497.
Caprio, S, Hyman, LD, McCarthy, S, Lange, R, Bronson, M & Tamborlane, WV (1996). Fat distribution and cardiovascular risk factors in obese adolescent girls: importance of the intraabdominal fat depot. Am. J. Clin. Nutr., 64, 12–17.
Cole, TJ, Bellizzi, MC, Flegal, KM & Dietz, WH (2000). Establishing a standard definition for child overweight and obesity worldwide: international survey. Br. Med. J., 320, 1240–1243.
Cook, JS, Hoffman, RP, Stene, MA & Hansen, JR (1993). Effects of maturational stage on insulin sensitivity during puberty. J. Clin. Endocrinol. Metab., 80, 172–178.
Daniels, SR, Khoury, PR & Morrison, JA (1977). The utility of body mass index as a measure of body fatness in children and adolescents: difference by race and gender. Pediatrics, 99, 804–807.
Deeg, R & Ziegenhorn, J (1983). Kinetic enzymatic method of automated determination of total cholesterol in serum. Clin. Chem., 29, 1798–1802.
de Ridder, CM, de Boer, RW, Seidell, JC, Nieuwenhoff, CM, Jeneson, JA, Bakker, CJ, Zonderland, ML & Erich, WB (1992). Body fat distribution in pubertal girls quantified by magnetic resonance imaging. Int. J. Obes. Relat. Metab. Disord., 16, 443–449.
Dietz, WH & Bellizzi, MC (1999). Introduction: the use of body mass index to assess obesity in children. Am. J. Clin. Nutr., 70, 123S–125S.
Ellis, KJ, Abrams, SA & Wong, WW (1999). Monitoring childhood obesity: assessment of the weight/height2 index. Am. J. Epidemiol., 150, 939–946.
Fagot-Campagna, A, Narayan, KM & Imperatore, G (2001). Type 2 diabetes in children. Br. Med. J., 322, 377–378.
Forbes, GB (1987). Human Body Composition. Growth, Aging, Nutrition, and Activity, New York: Springer
Franklin, MF (1999). Comparison of weight and height relations in boys from 4 countries. Am. J. Clin. Nutr., 70, (Suppl) 157S–162S.
Freedman, DS, Serdula, MK, Srinivasan, SR & Berenson, GS (1999). Relation of circumferences and skinfold thicknesses to lipid and insulin concentrations in children and adolescents: the Bogalusa Heart Study. Am. J. Clin. Nutr., 69, 308–317.
Friedewald, WT, Levy, R & Fredrickson, DS (1972). Estimation of the concentration of low density lipoprotein cholesterol in plasma without use of the preparative ultracentrifuge. Clin. Chem., 18, 499–502.
Goran, MI, Kaskoun, M & Shuman, WP (1995). Intra-abdominal adipose tissue in young children. Int. J. Obes. Relat. Metab. Disord., 19, 279–283.
Goran, MI, Driscoll, P & Jhonson, R et al (1996). Cross-calibration of body-composition techniques against dual-energy X-ray absorptimetry in young children. Am. J. Clin. Nutr., 63, 299–305.
Kanai, H, Matsuzawa, Y, Kotani, K, Keno, Y, Kobatake, T, Nagai, Y, Fujioka, S, Tokunaga, K & Tarui, S (1990). Close correlation of intra-abdominal fat accumulation to hypertension in obese women. Hypertension, 16, 484–490.
Larsson, B, Svardsudd, K, Welin, L, Wilhelmsen, L, Bjorntorp, P & Tibblin, G (1984). Abdominal adipose tissue distribution, obesity, and risk of cardiovascular disease and death: 13 year follow up of participants in the study of men born in 1913. Br. Med. J. (Clin. Res. Edn)., 288, 1401–1404.
Lean, MEJ, Han, TS & Seidell, JC (1998). Impairment of health and quality of life in people with large waist circumference. Lancet, 351, 853–856.
Lillioja, S, Mott, DM, Spraul, M, Ferraro, R, Foley, JE, Ravussin, E, Knowler, WC, Bennett, PH & Bogardus, C (1993). Insulin resistance and insulin secretory dysfunction as precursors of non-insulin-dependent diabetes mellitus. Prospective studies of Pima Indians. N. Engl. J. Med., 329, 1988–1992.
Lindsay, RS, Hanson, RL & Roumain, J et al (2001). Body mass index as a measure of adiposity in children and adolescents: relationship to adiposity by dual energy x-ray absorptiometry and to cardiovascular risk factors. J. Clin. Endocrinol. Metab., 86, 4061–4067.
Lohman, TG (1986). Applicability of body composition techniques and constants for children and youth. Exerc. Sport. Sci. Rev., 14, 325–357.
Maffeis, C, Pietrobelli, A, Grezzani, A, Provera, S & Tato, L (2001). Waist circumference and cardiovascular risk factors in prepubertal children. Obes. Res., 9, 179–187.
Moran, A, Jacobs, DR, Steinberger, J, Hong, CP, Prineas, R, Luepker, R & Sinaiko, AR (1999). Insulin resistance during puberty. Results from clamp studies in 357 children. Diabetes, 48, 2039–2044.
Must, A, Jacques, PF, Dallal, GE, Bajema, CJ & Dietz, WH (1992). Long-term morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922 to 1935. N. Engl. J. Med., 327, 1350–1355.
Nagele, U, Hagele, EO & Sauer, G et al (1984). Reagent for the enzymatic determination of serum total triacylglycerols with improved lipolytic efficiency. J. Clin. Chem. Clin. Biochem., 26, 1775–1779.
Pietrobelli, A, Faith, MS & Allison, DB et al (1998). Body mass index as a measure of adiposity among children and adolescents: a validation study. J. Pediatr., 32, 204–210.
Pi-Sunyer, FX (1991). Health implications of obesity. Am. J. Clin. Nutr., 53, 1595S–1603S.
Rankinen, T, Kim, SY, Perusse, L, Despres, JP & Bouchard, C (1999). The prediction of abdominal visceral fat level from body composition and anthropometry: ROC analysis. Int. J. Obes. Relat. Metab. Disord., 23, 801–809.
Stumvoll, M, Mitrakou, A, Pimenta, W, Jenssen, T, Yki-Jarvinen, H, Van Haeften, T, Renn, W & Gerich, J (2000). Use of the oral glucose tolerance test to assess insulin release and insulin sensitivity. Diabetes Care, 23, 295–301.
Tanner, JM (1962). Growth at Adolescence, 2nd edn. Blackwell: Oxford
Troiano, RP & Flegal, KM (1998). Overweight children and adolescents: description, epidemiology and demographics. Pediatrics, 101, 497–504.
WHO (1998). Preventing and managing the global epidemic, Report of a WHO Consultation on Obesity. Geneva, 3–5 June 1997 Geneva: World Health Organization
Author information
Authors and Affiliations
Contributions
Guarantor: Claudio Maffels, MO.
Contributors: Serone Ptlarma SpA, Via Casilina, 125 00 176, Roma, Italia.
Corresponding author
Rights and permissions
About this article
Cite this article
Maffeis, C., Corciulo, N., Livieri, C. et al. Waist circumference as a predictor of cardiovascular and metabolic risk factors in obese girls. Eur J Clin Nutr 57, 566–572 (2003). https://doi.org/10.1038/sj.ejcn.1601573
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejcn.1601573
Keywords
This article is cited by
-
Prevalence of abdominal obesity and associated risk factors among women civil servants in Addis Ababa, Ethiopia, 2021: an institution-based study
BMC Nutrition (2022)
-
Individual fatty acids in erythrocyte membranes are associated with several features of the metabolic syndrome in obese children
European Journal of Nutrition (2019)
-
Waist-to-height ratio and its associations with body mass index in a sample of Tuscan children in primary school
Italian Journal of Pediatrics (2017)
-
Body shape and size in 6-year old children: assessment by three-dimensional photonic scanning
International Journal of Obesity (2016)
-
Infant weight growth velocity patterns and general and abdominal adiposity in school-age children. The Generation R Study
European Journal of Clinical Nutrition (2016)
