
Abstract
Objective: To investigate the relationship between stunting and levels of overweight/obesity among South African school children, using two definitions of overweight and obesity, based on the WHO and International Obesity Task Force (IOTF) criteria.
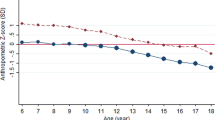
Design: Cross-sectional descriptive analysis of the nutritional status of primary school children, using primary data from a rural community-based study undertaken in 1995 and secondary data from the South African National Primary Schools (SANPS) survey conducted in 1994. Stunting was measured according to the WHO definition of −2 Z scores height-for-age. Two sets of criteria were used to measure overweight and obesity—the WHO/NCHS standard based on the 85th and 95th centiles and the IOTF criteria.
Setting: The primary data source was from a rural KwaZulu-Natal community based survey. The secondary data source SANPS consisted of data at National and Provincial level; for this study only data from the province of KwaZulu-Natal was considered.
Subjects: Primary school children aged between 8 and 11 y of age; 802 from the primary data source and 24 391 from the secondary source.
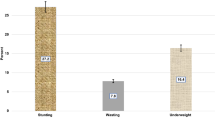
Results: Moderate stunting ranged from 2.9 to 40.2%, and mild stunting ranged from 31.4 to 75%. The prevalence of overweight ranged from 0.4 to 13.3% (WHO criteria) and from 0.4 to 11.9% using the IOTF criteria; while obesity ranged from 0.1 to 3.7% (WHO) and from 0.1 to 1.5% (IOTF criteria). The prevalence of overweight and obesity was observed to be higher using the WHO definition than that of IOTF (0.05<P<0.10). However, good kappa coefficient (κ) levels of agreement were observed between the WHO and IOTF definitions of overweight and obesity (κ>0.55, in all cases). The levels of agreement in all cases were less for obesity than overweight (both ranged from 0.55 to 1.0). Females were observed to have higher κ levels than their male counterparts; they also had higher prevalence levels of overweight and obesity across age and geographical group. Uniformly high levels of both mild and moderate stunting were observed both nationally and provincially. However, no excess relative risk of being overweight if stunted was observed in this study (P>0.05).
Conclusions: Caution must be applied when using either definition for obesity. However, very high levels of agreement occur for overweight. There is no obvious relationship between overweight and stunting in this study, but high levels of mild stunting were observed. Regular clinical and epidemiological monitoring of nutritional status needs to be undertaken in South Africa to examine possible future trends of overweight/obesity and their relationship with stunting, and for comparisons with global trends.
Sponsorship: The British Council supported the academic link between the UK and SA partners, which facilitated the research programme.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Bellizzi, MC & Dietz, WH (1999). Workshop on childhood obesity: summary of the discussion. Am. J. Clin. Nutr., 70, 173–175.
Budlender, D (2000). Human development. In:Poverty and Inequality in South Africa: Meeting the Challenge, ed. J May London: David Philip and Zed Press
Chinn, S & Rona, RJ (2001). Prevalence and trends in overweight and obesity in three sectional studies of British children, 1974–94. Br. Med. J., 322, 24–26.
Cole, TJ, Bellizzi, MC, Flegal, KM & Dietz, WH (2000). Establishing a standard definition for child overweight and obesity worldwide: international survey. Br. Med. J., 320, 1–6.
Department of Health (1994). Anthropometric survey in primary schools in the RSA, Sub-Directorate Statistical Analysis Pretoria: DOH
Department of Health (1999). South Africa Demographic and Health Survey 1998. Preliminary report, Department of Health, Pretoria: DOH
Gulliford, MC, Mahabir, D, Rocke, B, Chinn, S & Rona, R (2001). Overweight, obesity and skinfold thickness of children of African or Indian descent in Trinidad and Tobago. Int. J. Epidemiol., 30, 989–998.
Hansen, J (1989). Food and nutrition policy with relation to poverty: the child malnutrition problem in South Africa. In:Uprooting Poverty, the South African Challenge. Report for the Second Carnegie Inquiry into Poverty and Development in Southern Africa, ed. F Wilson & M Ramphele Johannesburg: David Philip Publishers
Hesketh, T & Ding, QJ (2000). Young Chinese people in Hong Kong are not representative of those in China. (Letter to Editor.). Br. Med. J., 321, 1158
Jinabhai, CC, Taylor, M, Coutsoudis, A, Coovadia, HM, Tomkins, AM & Sullivan, KR (2001). A health and nutritional profile of rural school children in KwaZulu-Natal, South Africa. Ann. Trop. Paediatr., 21, 50–58.
Jinabhai, CC, Taylor, M, Coutsoudis, A, Coovadia, HM, Tomkins, AM & Sullivan, KR (2001). A randomised controlled trial of the effect of anthelminthic treatment and micronutrient fortification on health status and school performance of rural primary school children. Ann. Trop. Paediatr., 21, 319–333.
Kinra, S (2000). Reanalysis suggests questionable validity of new definition during puberty. (Letter to Editor.). bmj.com, 29 May
Leung, SSF (2000). Establishing a standard definition for child overweight and obesity worldwide. (Letter to Editor.). bmj.com, 20 August
May, J (ed.) (2000). Poverty and Inequality in South Africa: Meeting the Challenge, London: David Philip and Zed Press
Monyeki, KD, van Lenthe, FJ & Steyn, NP (1999). Obesity: does it occur in African children in a rural community in South Africa. Int. J. Epidemiol., 28, 287–292.
Moreno, LA, Fleta, J, Sarria, A & Bueno, (2001). Prevalence and trends in childhood obesity in Zaragoza (Spain). (Letter to the Editor.). bmj.com, 2 February
Mulligan, J (2000). Body Mass Index is harder to interpret in children than adults. (Letter to Editor). Br. Med. J., 321, 1158
Popkin, B (1994). The nutrition transition in low-income countries: an emerging crisis. Nutr. Rev., 52, 285–298.
Popkin, BM, Richards, MK & Montiero, CA (1996). Stunting is associated with overweight in children of four nations that are undergoing the nutrition transition. J. Nutr., 126, 3009–3016.
United Nations Development Programme (2000). Human Development Indicators, www.undp.org/hdr/2000/english/book/back1.pdf
Wang, Y & Wang, J (2000). Standard definition of child overweight and obesity worldwide. (Letter to Editor.). Br. Med. J., 321, 1158
WHO (1995). Physical status: the use and interpretation of anthropometry, Report of a WHO Expert Committee. Technical Report Series 854 Geneva: WHO
WHO (2000). Obesity: preventing and managing the global epidemic, Report of a WHO Consultation. World Health Organization, Technical Report Series 894 Geneva: WHO
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jinabhai, C., Taylor, M. & Sullivan, K. Implications of the prevalence of stunting, overweight and obesity amongst South African primary school children: a possible nutritional transition?. Eur J Clin Nutr 57, 358–365 (2003). https://doi.org/10.1038/sj.ejcn.1601534
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejcn.1601534
Keywords
This article is cited by
-
Socioeconomic-related inequalities in child malnutrition: evidence from the Ghana multiple indicator cluster survey
Health Economics Review (2015)
-
Correlates of objectively measured overweight/obesity and physical activity in Kenyan school children: results from ISCOLE-Kenya
BMC Public Health (2014)
-
Secular trends in the prevalence of stunting, overweight and obesity among South African children (1994–2004)
European Journal of Clinical Nutrition (2011)
-
Gendered dimensions of obesity in childhood and adolescence
Nutrition Journal (2008)
-
Nature and strength of epidemiological evidence for origins of childhood and adulthood obesity in the first year of life
International Journal of Obesity (2007)
