
Key Points
-
Journal based verifiable continuing professional development (CPD) appears to be a valuable method of undertaking life-long learning.
-
The majority of participants felt that this form of CPD increased their knowledge and had resulted in a change in their clinical practice.
-
This form of CPD was one of many undertaken by the majority of respondents.
Abstract
Objective There is little information available on journal based verifiable continuing professional development (CPD). The aim of this study was to survey those dentists who have undertaken this form of CPD and elicit their views.
Design A questionnaire survey.
Method Four hundred dentists who had registered to undertake CPD with the British Dental Journal (BDJ) were randomly selected and sent a questionnaire.
Results Three hundred and twelve questionnaires were returned (78%) of these 181 (58%) were male and 131 (42%) were female. Of the 312, 307 had undertaken the BDJ CPD initiative. Two hundred and sixty eight respondents (87.3%) agreed/strongly agreed that the BDJ CPD satisfied their personal CPD needs. Two hundred and eighty three (92.2%) agreed/strongly agreed that their knowledge has been increased as a result of undertaking the BDJ CPD initiative. Two hundred and twenty agreed/strongly agreed (71.7%) that an element of their clinical practice had changed as a result of undertaking the BDJ CPD initiative.
Conclusion Journal based learning appears to be an effective way of undertaking verifiable CPD.
Similar content being viewed by others


Introduction
Continuing Professional Development (CPD) and lifelong learning are key components of the General Dental Council's (GDC) strategy for enhancing clinical governance within the dental profession in the United Kingdom and ensuring the public's trust of its dentists. At the outset the president of the GDC stated, '...an ongoing commitment to learning must be viewed as a professional responsibility for all those wishing to retain their name on the register.'1
The life-long learning initiative requires all registered dentists in the United Kingdom to engage in 250 hours of continuing professional development over a five year period, at least 75 hours of which should be 'verifiable' — that is defined as having concise educational aims and objectives, clear anticipated outcomes and identified quality control mechanisms.2
It was proposed that publicly funded courses organised by postgraduate dental deans, and courses organised through the British Dental Association (BDA), the Royal Colleges, universities and the Faculty of General Dental Practitioners will form one component of verifiable CPD. General CPD, that is the component of CPD which is not verified, was proposed to include the following: independent study of professional literature; multimedia learning, staff training; and background research. It is anticipated that the burden placed upon the dental practitioner by these requirements will not be an onerous one: 'Recertification formalises study that most GDPs already undertake voluntarily. The profession should therefore have no difficulty in complying with this worthwhile scheme.'3
Broadly speaking, CPD should meet the following requirements:4
-
It should satisfy identified needs of the person involved
-
It should be evaluated to ensure that learning was achieved
-
Something will have changed as a result of the training that will produce benefits to the individual undertaking the training.
In July 2003 the British Dental Journal (BDJ) in partnership with Eastman Continuing Professional Development established a new CPD programme to enable all UK dental practitioners to collect a maximum of 48 hours of verifiable CPD per annum. Each issue of the BDJ now contains two papers that have been selected for verifiable CPD, with four multiple choice questions linked to each article. Practitioners receive one verifiable CPD hour per paper, giving a potential total of two CPD hours per BDJ issue.5
While this has proved to be a very popular method of undertaking CPD, with 7,242 registered by the end of 2004, we actually know relatively little about the practitioners using it or the educational/learning benefit they are obtaining. It is vitally important that as well as practitioners demonstrating that they are keeping up to date with CPD, they are also gaining the maximum benefit from it as well. The aim of this study was to survey those dentists who have undertaken this form of CPD and elicit their views.
Method
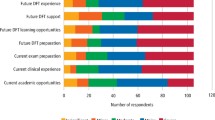
A questionnaire was designed (Fig. 1), the first part of which requested information on: gender, age, time qualified, where they work, and what forms of CPD they undertake. The second part of the survey concentrated on the suitability and level of the CPD questions, and any outcomes of undertaking this form of CPD.

Questionnaire used in this study
Of the 7,242 people who were registered as having undertaken the verifiable BDJ CPD initiative, 400 of those who had stated that they were willing to be contacted by Eastman CPD, were selected at random through a computer generated random number list. These 400 were sent a postal questionnaire with a covering letter and stamped address envelope for return.
Any respondents who had registered, but not undertaken the BDJ CPD were asked not to complete the second part of the questionnaire.
Results
Of the original 400 questionnaires, 312 were returned (78%). Of these five had not undertaken the BDJ CPD initiative and thus did not answer the second part of the questionnaire. Nine questionnaires were returned to sender stating that the address was unknown.
The results of the questionnaire are as follows:
Gender of responder
Of the questionnaires returned 181 (58%) were from males and 131 (42%) females.
Age group and time qualified
With reference to Figures 2 and 3 this demonstrated a good spread throughout all the age groups and of times qualified.

Bar graph to show age group of respondents

Bar graph to show how long respondents had been qualified dentists (years)
Where spends most of working week
As would be expected, since the majority of dentists in the UK work in general dental practice, the vast majority of respondents were in this category — 256 (82.1%). The rest were as follows: community dentistry 31 (9.9%), hospital-NHS 10 (3.2%), hospital-academic five (1.6%), armed forces six (1.9%), industrial one (0.3%). Three respondents did not answer this question.
Forms of CPD in last year
Table 1 shows that those people using BDJ CPD were in the vast majority not using this as the sole mechanism for obtaining their overall verifiable CPD, ie it was only forming a part of their CPD with 88% also attending postgraduate courses.
BDJ CPD satisfies personal CPD needs
Figure 4 shows that 268 respondents (87.3%) either agreed or strongly agreed with this statement.

Bar graph to show response that BDJ verifiable CPD initiative satisfies personal CPD needs
Articles are applicable to CPD needs
Two hundred and seventy eight respondents (90.6%) strongly agreed or agreed that the articles selected for use in the CPD were applicable to their CPD needs.
Levels of questions about the articles
Two hundred and eighty respondents (89.7%) felt that the level of questions about the selected articles were appropriate, 10 (3.2%) felt they were too difficult, 17 (5.4%) felt they were too easy.
Knowledge has been increased as a result of undertaking BDJ CPD
Figure 5 shows that 39 respondents strongly agreed (12.5%), 244 agreed (78.2%), 13 (4.2%) disagreed and 11 (3.5%) strongly disagreed with the statement that their knowledge had been increased as a result of undertaking this form of CPD.

Bar graph to show response to the question: has knowledge been increased as a result of undertaking BDJ CPD initiative?
Any element of clinical practice changed as a result of BDJ CPD?
Figure 6 shows that 19 respondents strongly agreed (6.1%), 201 agreed (64.4%), 84 disagreed (26.9%) and three strongly disagreed (1%) with the statement that an element of their clinical practice has changed as a result of undertaking this form of CPD.

Bar graph to show response to the question: has any element of clinical practice changed as a result of BDJ CPD initiative?
Statistical analysis
Chi-squared statistical testing was carried out on the data to assess for any differences in responses as a function of gender, age or time qualified. This showed no evidence (p>0.05) of statistically significant differences in responses given by gender, age or time qualified.
Discussion
It is important that as well as practitioners demonstrating that they are keeping up to date with CPD, they are also gaining a benefit from it as well. While the idea of journal based learning is not new, we actually know relatively little about it as a learning/training method. Clearly since verifiable CPD is now an essential part of recertification of all dentists in the United Kingdom,2 it is desirable to establish the merits of each method of obtaining it.
Currently there are 32,517 dentists registered in the United Kingdom, of which 32.5% are female and 67.5% male.6 Within the limitations of this study it is interesting to note that the random sample that we selected showed an increased female to male ratio compared to the overall population (42%: 58%). This may suggest that this form of CPD is more popular with females than males.
This form of CPD is becoming increasingly popular, with 7,242 (22%) of the dentists currently registered with the General Dental Council having enrolled to participate with the BDJ CPD. Of the 7,242, 5,669 (78.3%) have answered the BDJ CPD at least once in the last year. It is interesting to note that in the overwhelming majority of cases, it did not form the sole method of the respondents obtaining their verifiable CPD, but was effectively an adjunct to more traditional forms eg postgraduate courses.
In general the respondents were very positive in their overall opinion of this form of CPD and this may pave the way for other such journal based verifiable initiatives to take place.
One of the key elements that was identified about the requirements of CPD was that 'something will have changed as a result of the training that will produce benefits to the individual undertaking the training.'4 The results of this questionnaire suggest that this form of verifiable CPD has resulted in changes and benefits to the individuals involved. The vast majority of respondents felt that their knowledge had been increased as a result of participating in this form of CPD, and more than two thirds felt that an element of their clinical practice had changed as a result of participating in this form of CPD.
Conclusions
Within the limitations of the techniques employed in this study it is possible to draw the following conclusions:
-
1
BDJ CPD forms part — but not all of the CPD undertaken by the respondents.
-
2
The majority of the respondents' CPD is undertaken through postgraduate courses.
-
3
The majority of respondents are highly satisfied with the BDJ CPD.
-
4
The articles selected are applicable for the CPD needs of those undertaking the BDJ CPD.
-
5
The level of the articles selected in the BDJ is appropriate.
-
6
The majority of respondents feel that their knowledge has been increased as a result of undertaking BDJ CPD.
-
7
The majority of respondents report some form of change in their clinical practice as a result of undertaking BDJ CPD.
References
Wilson NHF . Lifelong learning. Br Dent J 2000; 188: 469.
General Dental Council. Lifelong learning; taking dentistry forward. London: General Dental Council, 2002.
Ross A . In Recertification for the dental profession. What it means for you ... http://www.gdc-uk.org/lifelong/lifelonglearning.htm, 2000.
Grace M . Evaluating the training. Br Dent J 2001; 191: 229–230.
Grace M . Verifiable CPD. Br Dent J 2003; 194: 643.
General Dental Council Registration Team, 5 August 2004, London.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Tredwin, C., Eder, A., Moles, D. et al. British Dental Journal based Continuing Professional Development: A survey of participating dentists and their views. Br Dent J 199, 665–669 (2005). https://doi.org/10.1038/sj.bdj.4812928
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4812928
This article is cited by
-
Perception of studying dental law and ethics among postgraduate dental students in the UK
British Dental Journal (2015)
-
BDJ UCL Eastman CPD programme: an online survey
British Dental Journal (2013)
-
Criteria for CPD
British Dental Journal (2006)
-
CPD revisited
British Dental Journal (2005)
-
Dentists' views on BDJ CPD
British Dental Journal (2005)
