
Key Points
-
Young people with hypodontia need early referral to a hypodontia team for optimal management
-
Hypodontia occurs in up to 7% of the UK population but is more prevalent in some conditions, notably, ectodermal dysplasias, Down syndrome and clefts of the lip andlor palate
-
Specialist paediatric dental care is essential to ensure retention of the reduced number of teeth
-
Optimization of spaces orthodontically combined with composite additions, resin retained bridges, veneers, onlays and tooth transplants contribute to an improvement in aesthetics and function.
Key Points
The interdisciplinary management of hypodontia:
-
1
Paediatric dentistry
-
2
Restorative dentistry
-
3
Orthodontics
-
4
Oral surgery
-
5
The relationship between an interdisciplinary team and the general dental practitioner
Abstract
This paper is the first of a series on the comprehensive management of young people with hypodontia. The paper looks at the background to the condition, the possible aetiological factors, the prevalence of hypodontia and other related conditions. Lastly there is consideration of the role of the paediatric dentist in interdisciplinary management of the affected child and adolescent patient.
Similar content being viewed by others

Main
Hypodontia, one of the commonest polymorphisms in man, is the congenital absence of teeth. Generally:
-
Hypodontia refers to the condition where there is absence of one or a few teeth only
-
Oligodontia is usually used to describe large numbers of missing teeth, six or more
-
Anodontia, the complete absence of teeth.
Thus, partial anodontia is a meaningless term and should not be used. Oligodontia is seen more frequently in cases where there are other systemic conditions (Figs 1 and 2).

Young boy with an ectodermal dysplasia (eyes obscured)

The same child showing the severe hypodontia
Management
The congenital absence of teeth can seriously disable a young person both physically and emotionally, especially during the turbulent years of adolescence. Yet, there are reports of patients with hypodontia1 being referred late with all that that implies – treatment disrupting the examination years, reluctance to wear appliances because of the impact on the young person's social life, for example.
There is much to be gained from the interdisciplinary management of young people who have hypodontia. Many patients are looked after by multidisciplinary teams – and each clinician does their own thing in isolation. True interdisciplinary working involves the close working of a committed team where each member contributes their expertise to achieve an optimum outcome for the patient and their family.1,2
Aetiology
Congenital absence of teeth is a consequence of:
-
Physical obstruction or disruption of the dental lamina
-
Space limitation
-
Functional abnormalities of the dental epithelium
-
Failure of initiation of the underlying mesenchyme.
What determines these events is still open to speculation.3 As with other conditions the causes of missing teeth can be broadly classified into general and local. General encompasses those cases where there is a genetic cause, in some cases related to other underlying conditions, particularly syndromes. Local factors result in acquired hypodontia, for example, early irradiation of tooth germs, hormonal and metabolic influences, trauma, osteomyelitis, and unintended removal of a tooth germ during the extraction of a primary tooth.
Hypodontia does not present in isolation but is related to the frequency of other missing teeth, the size of the remaining teeth and the rate of dental development.4 An early investigator5 has shown that there is an antero-posterior gradient in relative crown size reduction and a posterior-anterior gradient for tooth formation in people with missing third molar teeth. Relatives too may show dental effects other than hypodontia; In comparison with a control group, relatives of people with hypodontia demonstrated a reduction in crown dimension despite the fact that they themselves did not have hypodontia.6
Pirinen et al.7 postulated from their studies that the relationship of palatal canines and absent or diminutive maxillary lateral incisors could be caused by the same genetic effect that causes incisor-premolar hypodontia. In their series of 106 patients, palatally impacted canines were seen in 4.9% of cases and in several generations related to the affected subject, over twice the population prevalence. Bacceti,8 in a sample of 1,620 young people with a mean age of 14.8 years, found a significant relationship between tooth rotations and adjacent tooth hypodontia; a rotated maxillary lateral incisor was associated with absence of the homologous tooth with a similar result for premolars,
There is, thus, a genetic component to hypodontia that is regarded, in the absence of other systemic conditions, as an autosomally inherited, dominant condition with varying expression, for example, peg-shaped maxillary lateral incisors, and incomplete penetrance.9 In twins, a significantly higher prevalence of hypodontia is recorded with a high index of heritability indicative of a genetic determinant.10 Some workers are concentrating on candidate genes that are thought to have an important role in tooth development.8 Others have demonstrated a mutation in the homeobox gene MSX1 that may be critical to the normal development of specific human teeth.11
It is known that not all teeth are equally heritable.12 The 'key' tooth in each morphological class has the highest heritability and is the more stable tooth morphologically. The more distal a tooth, for example, lateral incisors and second premolars, the more it seems to be influenced by environment.13However, given the very different development times of these two teeth, they are more likely to be influenced by genetic factors. What this research points to is that there is a polygenic mode of inheritance such that there is an interaction between the environment and genes.
Prevalence
Overall prevalence
The approximate ages at which clinicians would expect to see teeth present either radiographically or erupted into the mouth are shown in Table 1.14 Assuming a correct diagnosis, the prevalence rate for hypodontia in British children is of the order of 0.1–0.9% in the primary dentition and in the permanent dentition, is 3.5 to 6.5%.15
In a sample of 193 Danish children with absent primary teeth, 54.9% were missing only one primary tooth.16
Tooth predilection
There is variation in the literature as to which tooth types are commonly missing due partly perhaps to ethnic variation; in African negroes and Australian aborigines the prevalence is 1% but can be as high as 30% in Japanese people. Assuming that third molars are the most frequently missing teeth, the next most frequently missing teeth, in reducing order of prevalence are:
Mandibular second premolar teeth (2.8%)
Maxillary lateral incisors (1.6%)
Maxillary second premolars, and mandibular incisors (0.23%–0.08%).17,18
In Swedish and Japanese populations, lower central incisors are more commonly missing than in other races.19
Dentition predilection
In the primary dentition maxillary lateral incisors are twice as likely to be missing as mandibular lateral incisors. Congenital absence of the remaining primary teeth is very rare.16 However, there does appear to be a strong relationship between missing primary teeth and permanent successors; Daugaard-Jensen and co-workers20in Denmark showed that, in a radiographic survey of 213 children, where there was hypodontia in the primary dentition, it was always a feature in the permanent dentition. The pattern however, was different: incisors missing in the primary dentition, premolars in the permanent and the numbers missing in the permanent dentition were always greater than in the primary dentition. Hypodontia affecting teeth that are rarely missing, for example, first permanent molars, was usually associated with missing primary teeth.
In a study of 1,680 children in New Zealand, of the 23 children with hypodontia of the primary dentition, 61% had a permanent dentition similarly affected. Boys were more commonly affected than girls.21
Other conditions
General conditions
Hypodontia is a feature of more generalised systemic conditions. The most familiar is Down syndrome with missing teeth reported commonly in one series of 395 patients aged 12–36 years.22 In people with a cleft lip and palate, the prevalence of hypodontia of premolar teeth was 18%. There was a significantly higher number of missing teeth affected in the maxilla than in the mandible, and especially on the side that is more often affected by clefting.23 Other, rarer conditions associated with hypodontia as a feature often present with missing teeth that are otherwise rarely absent, for example, first permanent molars. This is important for dentists to note since they should consider referring children with missing teeth for screening for other anomalies of ectoderm to rule out the possibility of a syndrome being present.24,25
Ectodermal dysplasias (ED)
The one group of conditions classically associated with hypodontia are the ectodermal dysplasias (ED). The condition occurs as a consequence of disturbances in the ectoderm of the developing embryo. Two major types are described, based on the number and functioning of the sweat glands:
-
X-linked anhidrotic or hypohidrotic, where sweat glands are either absent or significantly reduced in number,
-
Hidrotic where sweat glands are normal and the condition is inherited as autosomal dominant.
Approximately 132 different clinical syndromes have been identified. The incidence is 1:100,000 with a mortality of 28% in males by 3 years of age.26,27,28
The condition is usually transmitted as an X-linked recessive trait although there is a rarer form, clinically identical to the X-linked condition but inherited as an autosomal recessive trait, which affects females severely. In the former, the carrier mother demonstrates minimal expression of the gene, perhaps only hypodontia/ microdontia and some diminution in sweating. She has a 50% chance of passing the gene on to male offspring. Female offspring have a 50% chance of inheriting the gene and thus becoming a carrier too. Spontaneous gene mutation is also possible.14 Up to 75% of female carriers display hypodontia in the permanent dentition and its occurrence in the primary dentition increases the diagnostic validity.
There are a number of familiar syndromes which are classified with ED, for example, Ellis-van Creveld and incontinentia pigmenti.
Dentists have a responsibility in the detection of carrier status since hypodontia in either of the dentitions may be the only sign of what can be a potentially life-threatening condition.26
Clinically (Fig. 3) children present with features of :

Young boy with all the external features of an ectodermal dysplasia (eyes obscured)
General Dental Prominent forehead Hypodontia Protruding, low-set ears Microdontia Periorbital wrinkling and pigmentation Hypoplasia/hypo-mineralisation Saddle nose deformity Xerostomia Protruding and everted lips Hypoplastic alveoli Reduced lower face height Dental caries Prominent mental sulcus Taurodontism Dysplastic nails Thickened fraena Sparse eyebrows, hair and eyelashes Absent uvula/clefts Eczema
Role of the dental team
The role of dental care is to:
-
Maintain the existing dentition
-
Improve aesthetics
-
Enable patients to eat a wide range of foods
-
Improve speech
-
Promote emotional and psychological well-being
-
Improve acceptance by family and peers
There is little research to indicate the impact of extensive hypodontia on a young person.29 It is known that from around 9 years of age, children with disabilities realise that they will remain different from other children. This realisation may produce a state of depression in the child with severe hypodontia and the dental team has a role in helping that young person to cope with issues of attractiveness during the important, formative years.30
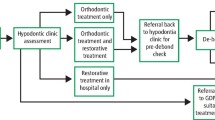
Role of the paediatric dentist on the interdisciplinary hypodontia team
Early referral of patients with hypodontia is helpful in the long-term planning of care.
However, evidence in the UK indicates that referral to a hypodontia team in one centre was as late as 12 years of age suggestive either of non-demand from patients/parents or lack of awareness of need by primary care providers.1 Whilst shared care is feasible in most instances, only 17% of cases in the UK study cited above were referred back to their primary practitioner for management.
The issues for the paediatric dentist are:
-
Behaviour management in a challenged young person
-
Prevention of caries, especially in xerostomic ED patients
-
Maintenance of, usually good, oral hygiene and awareness of the potential for wear of retained primary teeth
-
Management of infraocclusion of primary teeth
-
Intermediate restoration of diminutive teeth with composite additions
-
Endodontic care in autotransplantation
-
Resin-retained bridgework/veneers
Behaviour management
Children with hypodontia may suffer from social isolation and may exhibit poor dental co-operation.31 There may be a need to use different behaviour management techniques, including sedation for dental treatment. In patients with ED, the lack of sweat glands could theoretically lead to overheating and so, in cases where nitrous oxide sedation is contemplated, the associated peripheral vasodilatation and the patient's ability to cope with this physiologically, should be borne in mind. Likewise, the effect of the condition on mucous secreting glands and as a consequence, rhinitis, and chronic bronchitis, may be a contraindication to this form of sedation.27
Preventive care
It is important to protect the remaining tooth tissue in young people with hypodontia and so prevention of dental disease is paramount. Dental caries may be less prevalent because of spaced dentitions but conversely, xerostomia in ED may increase the risk. Enamel defects, hypoplasia and hypomineralisation, increase the potential for caries to develop. Such children should be treated as high risk and the guidelines, as laid down in relevant paediatric dentistry policy documents, adhered to.32,33,34,35
Oral hygiene is usually very good in these young people, perhaps because there is ease of access to all surfaces or because concern over aesthetics means that the child is focused on doing anything to improve appearance and care for what teeth they have.
Parents report difficulties in cleaning lone standing teeth and need advice on how to manage this as well as the most suitable way to clean unfamiliar prostheses.36
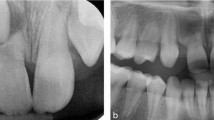
Management of infraocclusion in primary teeth
Retention of primary molar teeth where the permanent successor is absent is important in cases of hypodontia since they retain bone in an area which may be a site for future transplantation or implant therapy. The prevalence of infraocclusion is not well documented but it is increased in these patients.37 Altered pulp pathology will determine the most appropriate management38but may involve pulp therapy and restoration with pre-formed metal crowns. Where restoration for caries is not necessary, an infraoccluded tooth that is static may have onlays placed39 in order to facilitate cleaning as well as preventing food packing and its sequelae (Figs 4 5 6). If seen early enough it may be prudent, in conjunction with orthodontists, to remove the primary molar tooth where there is no successor to achieve an optimum outcome.40

Onlays on infraocluded primary molar teeth (teeth no LLD (74) and LLE (75))

Buccal view of the onlays in figure 4

Gold onlay on an infraoccluded tooth in combination with a lower partial denture
The longevity of the primary dentition, where there are no permanent successors, is uncertain. One study has reported on a retrospective radiographic review of children with severe hypodontia. It would appear from this that it is only the primary canine teeth, rather than molar teeth that have a predictable lifespan.41
Intermediate restorations – planning principles
Interim restorations may be indicated before definitive care to ease the transition of the child into early adolescence. These may include resin-modified additions to the existing teeth as well as more sophisticated restorations (Figs 7, 8).

The spaced dentition of a young person with hypodontia

A combination of composite additions and a resin retained bridge to restore the spaces in the young person after orthodontic care in Figure 7
Some orthodontic treatment may be indicated prior to placement of restorations to optimise spaces (Fig. 9) and close co-operation between orthodontist and the clinician providing this restorative care cannot be stressed too often42 (see Parts 2 and 3 of this series). It is known that apical root resorption during orthodontic treatment is more prevalent in maxillary incisors of patients with extensive hypodontia as well as abnormal root form. This is especially the case with some arch mechanics – rectangular arch wires and intermaxillary elastics. The orthodontist needs to monitor this regularly and the paediatric dentist may need to provide appropriate endodontic therapy.43

Localised space closure using a sectional upper fixed appliance
Early treatment may involve the placement of dentures which young children adapt to readily but with continued growth will need to be replaced frequently. Whilst theoretically facial growth may be compromised in these children, there is no evidence to support this supposition.44 Overdentures, which allow the retention of retained primary teeth, can also be used as a reservoir for topical fluoride therapy (Fig. 10).45

An overdenture fitted to the patient in Figure 9
Resin-retained bridgework is preferable to fixed prosthetic reconstructions at a young age because of the size of immature pulps (Fig. 8). However, unfavourable occlusions, rotated teeth and translucent, microdont teeth may mitigate against this form of treatment. Large lateral loads on primary teeth are to be avoided as it may bring about premature root resorption. Contingencies should be built in to the treatment plan to allow for the loss of such teeth and their addition to the existing prosthesis without recourse to costly re-planning and fabrication of new dentures.46
Where tooth tissue is at a premium yet some quadrants are crowded, auto-transplantation of teeth may be a viable option (see Part 4 of this series) especially if this can be carried out before apical closure of the donor tooth root has occurred.47
Close liaison between surgeon, orthodontist and paediatric dentist is crucial to maximise outcome, for example in the timing of orthodontic and paediatric intervention if indicated (Fig. 11).48

The tooth as well as the microdont maxillary lateral incisor (tooth no. UL2 (22)) adjacent have been restored with porcelain veneers
In the longer term, some of these children will be offered implant retained prostheses49,50,51 (see Part 3 of this series). Normally these will be placed when the period of growth has ceased to prevent infraocclusion of the 'ankylosed' implant. However, in children with no teeth and thus no alveolar bone, this is not as important a consideration and implants have been successfully placed in children as young as 3 years of age. Provided the implants are not intermixed with natural teeth problems are minimised (Fig. 12). To date there is no evidence that such placement promotes craniofacial growth and development but there is evidence that it fosters psychological well being.50

Mandibular implants in a young man with an ectodermal dysplasia
Summary
Crucial to a successful outcome for these young people is good communication both between professionals in an interdisciplinary team but also with patient/parents/carers. To that end, written information before a visit can answer many of the general questions a family has and serves to allay initial anxieties.
Optimising clinical outcome is one consideration, doing it cost-effectively is another, and increasingly important aim. The comparative costs of the different approaches to be adopted in the comprehensive care of young people with hypodontia in Denmark are given in Table 2.52Despite the cultural differences in the approach to healthcare between countries, these figures give an indication of the direction in which services should be focused.
References
Hobkirk JA, Goodman JR, Jones SP Presenting complaints and findings in a group of patients attending a hypodontia clinic. Br Dent J 1994; 177: 337–339.
Bergendal B, Bergendal T, Hallonsten A-L, Koch G, Kurol J, Kvint S A multidisciplinary approach to oral rehabilitation with osseointegrated implants in children and adolescents with multiple aplasia. Eur J Orthod 1996; 18: 119–129.
Meon R Hypodontia of the primary and permanent dentition. J Clin Paed Dent 1992; 16: 121–123.
Suarez BK, Spence MA The genetics of hypodontia. J Dent Res 1974; 53: 781–785.
Butler PM Studies of the mammalian dentition. Differentiation of the post-canine dentition. Proc Zoo Soc (Lond) 1939; 109: 1–36.
Schalk-vander Weide Y, Bosman F Tooth size in relatives of individuals with oligodontia. Arch Oral Biol 1996; 41: 469–472.
Pirinen S, Arte S, Apajalahti S Palatal displacement of canine is genetic and related to congenital absence of teeth. J Dent Res 1996; 75: 1742–1746.
Baccetti T Tooth rotation associated with aplasia of nonadjacent teeth. Angle Orthod 1998; 68: 471–474.
Arte S, Nieminen P, Pirinen S, Thesleff I, Peltonen L Gene defect in hypodontia: exclusion of EGF, EGFR and FGR-3 as candidate genes. J Dent Res 1996; 75: 1346–1352.
Lapter M, Slaj M, Skrinjaric I, Muretic Z Inheritance of hypodontia in twins. Collegioum Antropol 1998; 22: 291–298.
Vastardis H, Karimbux N, Guthua SW, Seidman JG, Seidman CE A human MSZ1 homeodomain missence mutation causes selective tooth agenesis. Nature Genetics 1996; 13: 417–421.
Bailit HL Dental variations among populations, an anthropologic view. Dent Clin N Am 1975; 19: 125–139.
Schalk-vander Weide Y, Steen WHA, Bosman F Distribution of missing teeth and tooth morphology in patients with oligodontia. J Dent Child 1992; 59: 133–140.
Kupietzky A, Houpt M Hypohidrotic ectodermal dysplasia: characteristic and treatment. Quintessence Int 1995; 26: 285–291.
Brook AH Dental anomalies of number, form and size: their prevalence in British schoolchildren. J Int Assoc Dent Child 1974; 5: 37–53.
Daugaard-Jensen J, Nodal M, Kjaer I Pattern of agenesis in the primary dentition: a radiographic study of 193 cases. Int J Paed Dent 1997(a); 7: 3–7.
Grahnen H Hypodontia in the permanent dentition. Clinical and genetic investigations. Thesis. Odont Revy 1956 (Suppl) 7: 3.
Cameron J, Sampson WJ Hypodontia of the permanent dentition. Case reports. Aust Dent J 1996; 41: 1–5.
Arita M, Iwagaki H Studies on the serial observations of dentofacial regions in Japanese children Monographs Tokyo: Nikon University School of dentistry 1963.
Daugaard-Jensen J, Nodal M, Skovgaard LT, Kjaer I Comparison of the pattern of agenesis in the primary and permanent dentitions in a population characterised by agenesis in the primary dentition. Int J Paed Dent 1997(b); 7: 143–148.
Whittington BR, Durward CS Survey of anomalies in primary teeth and their correlation with the permanent dentition. N Z Dent J 1996; 92: 4–8.
Mestrovic SR, Rajic Z, Papic JS Hypodontia in patients with Down's syndrome. Collegium Antropologicum 1998; 22: 69–72.
Shapira Y, Lubit E, Kuftinee MM Congenitally missing second premolars in cleft lip and cleft palate children. Am J Orthodont Dentofacial Orthopedics 1999; 115: 396–400.
Stimson JM, Stivers JE, Hava GL Features of oligodontia in three generations. J Clin Ped Dent 1997; 21: 269–275.
Guckes AD, Roberts MW, McCarthy GR Pattern of permanent teeth present in individuals with ectodermal dysplasia and severe hypodontia suggests treatment with dental implants. Ped Dent 1998; 20: 278–280.
McLaughlin WS Congenital absence of all primary and permanent lateral incisors in a carrier of x-linked hypohidrotic ectodermal dysplasia. Int J Paed Dent 1991; 2: 99–103.
Ellis SGS, Ahmed H Hypohidrotic ectodermal dysplasia affecting a female patient. Dent Update 1993; 20: 447–450.
Ziada H, Holland T Ectodermal dysplasia: a case report. J Irish Dent Assoc 1997; 43: 127–130.
Hummel P, Guddack S Psychosocial stress and adaptive functioning in children and adolescents suffering from hypohidrotic ectodermal dysplasia. Ped Dermatol 1997; 14: 180–185.
Lagerheim B Why me? – A depressive crisis at the age of nine in handicapped children. In: Gyllensvard A, Lauren K (Eds). Psychosomatic disease in childhood. Stockholm: Sven Jerring Foundation.
Nussbaum B, Carrel R The behaviour modification of a dentally disabled child. J Dent Child 1976; 43: 255–261.
Holt RD, Nunn JH, Rock WP, Page J Fluoride dietary supplements and fluoride toothpastes for children: a policy document. Int J Paed Dent 1996 6: 139–142.
Nunn JH, Murray JJ, Smallridge J British Society of Paediatric Dentistry: a policy document on fissure sealants in paediatric dentistry. Int J Paed Dent 2000; 10: 174–177.
Royal College of Surgeons of England Faculty of Dental Surgery. Prevention of dental caries in children. In: National Clinical Guidelines 1997.
Royal College of Surgeons of England Faculty of Dental Surgery. Continuing oral care – review and recall. In: National Clinical Guidelines 1997.
Nunn JH Ectodermal Dysplasia and oral health. EDLines 2002; 2: 1–3.
McGivern BM, Nunn JH, Carter NE A review of the outcome of infraoccluded primary teeth in a population of referred young people. Int J Paed Dent 1999; 9 (Suppl) 85.
Saad AY Regressive changes of the dental pulp complex in retained primary molars with congenitally missing successor teeth. J Clin Ped Dent 1997; 22: 63–67.
Evans RD, Briggs PF Restoration of an infraoccluded primary molar with an indirect composite onlay: a case report and literature review. Dent Update 1996; 23: 52–54.
Mamopoulou A, Hagg U, Schroder U, Hansen K Agenesis of mandibular second premolars. Spontaneous space closure after extraction therapy. A 4-year follow-up. Eur J Orthodont 1996; 18: 589–600.
Haselden K, Hobkirk JA, Goodman JR, Jones SP, Hemmings KW Root resorption in retained deciduous canine and molar teeth without permanent successors in patients with severe hypodontia. Int J Paed Dent 2001; 11: 171–178.
Miller TE Implications of congenitally missing teeth: orthodontic and restorative procedures in the adult patient. J Pros Dent 1995; 73: 115–122.
Levander E, Malmgren O, Stenback K Apical root resorption during orthodontic treatment of patients with multiple aplasia: a study of maxillary incisors. Eur J Orthodont 1998; 20: 427–434.
Yuksel S, Ucem T The effect of tooth agenesis on dentofacial structures. Eur J Orthodont 1997; 19: 71–78.
Renner RP, Kleinerman V Overdenture techniques in management of oligodontia – a case report. Quintessence Int 1980; 4: 57–65.
Hobkirk J, Brook AH The management of patients with severe hypodontia. J Oral Rehab 1980; 7: 289–298.
Thilander B, Odman J, Grondhal K, Friberg B Osseointegrated implants in adolescents. An alternative in replacing teeth? Eur J Orthodont 1994; 16: 84–95.
Paulsen HU, Andreasen JO, Scwartz O Pulp and periodontal healing, root development and root resorption subsequent to transplantation and orthodontic rotation: a long-term study of autotransplanted premolars. Am J Orthod Dentofac Orthop 1995; 108: 630–640.
Bergendal T, Eckerdal O, Hallonsten A-L, Koch G, Kurol J, Kvint S Osseointegrated implants in the oral rehabilitation of a boy with ectodermal dysplasia: a case report. Int Dent J 1991; 41: 149–156.
Guckes AD, McCarthy GR, Brahim J Use of endosseous implants in a 3-year-old child with ectodermal dysplasia:case report and 5-year follow-up. Ped Dent 1997; 19: 282–285.
McMillan AS, Nunn JH, Postlethwaite K Implant supported prosthesis in a child with hereditary mandibular anodontia: the role of ball attachments. Int J Paed Dent 1998; 8: 65–70.
Andreasen J Personal communication 1997.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Nunn, J., Carter, N., Gillgrass, T. et al. The interdisciplinary management of hypodontia: background and role of paediatric dentistry. Br Dent J 194, 245–251 (2003). https://doi.org/10.1038/sj.bdj.4809925
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4809925
This article is cited by
-
A service evaluation of the multidisciplinary team approach to hypodontia
British Dental Journal (2023)
-
Restorative dentistry clinical decision-making for hypodontia: retained primary molars
British Dental Journal (2023)
-
Familial colorectal cancer and tooth agenesis caused by an AXIN2 variant: how do we detect families with rare cancer predisposition syndromes?
Familial Cancer (2022)
-
Tooth agenesis in German orthodontic patients with non-syndromic craniofacial disorder: a retrospective evaluation of panoramic radiographs
Clinical Oral Investigations (2022)
-
More patient-centred measures required to evaluate hypodontia care outcomes and drive health service improvements
Evidence-Based Dentistry (2018)
