
Abstract
In this double-blind study, patients with an acute exacerbation of schizophrenia or schizoaffective disorder were randomized to receive either ziprasidone 80 mg/day (n = 106) or 160 mg/day (n = 104) or placebo (n = 92), for 6 weeks. Both doses of ziprasidone were statistically significantly more effective than placebo in improving the PANSS total, BPRS total, BPRS core items, CGI-S, and PANSS negative subscale scores (p < .05). Ziprasidone 160 mg/day significantly improved depressive symptoms in patients with clinically significant depression at baseline (MADRS ≥ 14, over-all mean 23.5) (p < .05) as compared with placebo. The percentage of patients experiencing adverse events was similar in each treatment group, and resultant discontinuation was rare. The most frequent adverse events associated with ziprasidone were generally mild dyspepsia, nausea, dizziness, and transient somnolence. Ziprasidone was shown to have a very low liability for inducing movement disorders and weight gain. The results indicate that ziprasidone is effective and well tolerated in the treatment of the positive, negative, and depressive symptoms of an acute exacerbation of schizophrenia or schizoaffective disorder.
Similar content being viewed by others


Main
Ziprasidone (5-[2-[4-(1,2-Benzisothiazol-3-yl)piperazin-1-yl]ethyl]-6-chloroindolin-2-one hydrochloride hydrate) is a novel antipsychotic with high affinity for dopamine D2 and D3, serotonin 5HT2A, 5HT2C, and 5HT1D receptors and high affinity for the 5HT1A receptor, where it acts as a potent agonist (Seeger et al. 1995) (Table 1). Ziprasidone moderately inhibits 5HT and norepinephrine re-uptake into nerve terminals, has relatively modest affinity for histamine H1 and adrenergic α1 receptors, low affinity for dopamine D1 and α2 receptors, and negligible affinity for M1 receptors.
In vitro functional dopamine receptor antagonism by ziprasidone has been demonstrated by concentration-dependent blockade of effects induced by a D2 agonist, quinpirole (inhibition of forskolin-stimulated adenylate cyclase) (Seeger et al. 1995). After systemic administration, ziprasidone produced relatively modest increases in dopamine metabolites as compared with haloperidol (Seeger et al. 1995). The inhibition by ziprasidone of the firing of dorsal raphe 5HT neurons was antagonized by the selective 5HT1A antagonist WAY-100,635, as was the elevation of extracellular levels of dopamine in the medial frontal cortex, establishing in vivo 5HT1A agonist activity (Reynolds et al. 1997; Lu et al. 1997). Ziprasidone also exhibited selectivity for prefrontal cortical vs. striatal dopamine release (Lu et al. 1997).
The pharmacological properties of ziprasidone may be predictive of enhanced clinical efficacy and a favorable tolerability profile, as compared with other agents, in the treatment of schizophrenia (Seeger et al. 1995; Tandon et al. 1997) (Table 1). These properties include a high ratio of 5HT2A to D2 receptor affinities (Meltzer, 1995, for review; Meltzer et al. 1989, for review; Deutch et al. 1991; Matsubara et al. 1993; Stockmeier et al. 1993) stimulation of 5HT1A receptors (Sharma and Shapiro 1996, for review; Newman-Tancredi et al. 1996; Neal-Beliveau et al. 1993). Blockade of 5HT1D receptors and moderate affinity in blocking synaptic re-uptake of serotonin and norepinephrine distinguishes ziprasidone from conventional and other newer antipsychotics and have been associated with the therapeutic effects of antidepressant agents (Rickels and Schweizer 1993; Briley and Moret 1993). Ziprasidone's negligible affinity for muscarinic M1 receptors (Seeger et al. 1995) contrasts with clozapine and olanzapine (Moore et al. 1993; Seeman and van Tol 1993; Bymaster et al. 1996); its relatively modest affinity for α1 receptors contrasts with risperidone and sertindole (Seeger et al. 1995; Schotte et al. 1996); and its agonist properties at the 5HT1A receptor are in contrast to olanzapine, quetiapine (Reynolds et al. 1997), risperidone (Seeger et al. 1995), sertindole and clozapine (Schotte et al. 1996).
In behavioral pharmacology, assays with predictive value for antipsychotic action (Niemegeers and Janssen 1979), ziprasidone antagonized d-amphetamine-induced hyperactivity and apomorphine-induced stereotypy and inhibited conditioned avoidance (Seeger et al. 1995). Ziprasidone also reversed both dopamine agonist- (apomorphine) and NMDA antagonist- (ketamine) induced prepulse inhibition deficits (Brooks and Mansbach 1997). In models considered to have predictive value for extrapyramidal side-effect liability (Niemegeers and Janssen 1979), the in vivo potency of ziprasidone in blocking a 5HT2A agonist-(quipazine) induced head twitches and amphetamine-induced locomotor activity each occurred at substantially lower doses than those needed to produce catalepsy (Seeger et al. 1995). These data suggest that there is good separation of the therapeutic efficacy of ziprasidone vs. the propensity to produce extrapyramidal side effects (Seeger et al. 1995).
Ziprasidone was selected for clinical development, because its preclinical profile was considered predictive of antipsychotic efficacy, with modest anti-adrenergic and antihistaminergic and no anticholinergic side-effect liability. Its high ratio of 5HT2A to D2 antagonism, low potency to produce catalepsy, agonist effects at the 5HT1A receptor, reversal of ketamine disruption of prepulse inhibition, preferential release of dopamine in the prefrontal cortex vs. the striatum, and blockade of synaptic re-uptake of 5HT and norepinephrine were considered favorable predictors of low liability for motor side effects and benefits in negative symptoms, cognition, and mood.
In healthy volunteers, positron emission computed tomography (PET) studies confirmed that the occupancy by ziprasidone of 5HT2 receptors substantially exceeded that of D2 receptors (Fischman et al. 1996; Bench et al. 1993; Bench et al. 1996). In a 28-day clinical trial in which the majority of patients (84/90) had an acute exacerbation of schizophrenia or schizoaffective disorder, ziprasidone 160 mg/day reduced Brief Psychiatric Rating Scale (BPRS) total and core item scores and Clinical Global Impression of Severity (CGI-S) scores similarly to haloperidol 15 mg/day (Goff et al. 1998). In a second 28-day clinical trial, involving 139 patients with an acute exacerbation of schizophrenia or schizoaffective disorder, ziprasidone 120 mg/day was significantly more effective than placebo in improving BPRS total, BPRS anxiety–depression cluster, BPRS anergia factor scores, and CGI-S (Keck et al. 1998).
In the present article, we report the results of a large, Phase III, randomized, placebo-controlled, parallel group, fixed dose study designed to evaluate the efficacy and safety of 6 weeks of treatment with ziprasidone (80 mg/day and 160 mg/day) in patients with an acute exacerbation of schizophrenia or schizoaffective disorder.
METHODS
Subjects
Men or women aged over 18 years, with an acute exacerbation of chronic or subchronic schizophrenia (295.x3) or schizoaffective disorder (295.x4) as defined in DSM-III-R (American Psychiatric Association 1987) were eligible to enter. They were to have been hospitalized within the previous 4 weeks and been diagnosed at least 6 months before the study. The patients were required to have a total score ≥ 60 on the Positive and Negative Syndrome Scale (PANSS) (Kay et al. 1989) and a score of at least 4 on two or more core items in the PANSS (conceptual disorganization, hallucinatory behavior, suspiciousness, and unusual thought content) in the 24 hours before study treatment was started. In addition, the patients were required to have a score of 3 (minimally improved) or greater (worse) on the Clinical Global Impression Improvement Scale (CGI-I) (National Institutes of Mental Health 1976a) at baseline as compared with screening.
Patients were excluded if they were resistant to neuroleptic treatment (defined as failure to respond to two or more marketed antipsychotic agents given at an adequate dose for sufficient time), had been hospitalized for more than 4 weeks before screening, or had DSM-III-R-defined psychoactive substance abuse/dependence in the preceding 3 months. Also excluded were those with mental retardation, an organic mental disorder, previous brief reactive psychosis, those who had received long-acting intramuscular neuroleptic medication within 4 weeks of the first day of double-blind treatment (unless blood level was below therapeutic level), and those judged by the investigator to be at imminent risk of suicide or homicide.
Patients were required to have normal electrocardiograms (ECG, with the exception of abnormalities considered by the investigator to be clinically unimportant) and normal laboratory test results (with the exception of minor deviations considered by the investigator to be clinically unimportant). Body weight was generally at least 80% of the lower limit of normal and no greater than 160% of the upper limit of normal according to sex, height, and frame (Metropolitan Life Insurance Company 1993). Urine samples obtained during screening were required to be negative for all illicit drugs, except cannabinoids and benzodiazepines that were allowed based on the investigators’ discretion. Patients were excluded if they had received any investigational drug in the 4 weeks immediately preceding the baseline visit of the study, fluoxetine within 5 weeks of the first day of double-blind treatment, or phencyclidine during the 90 days before admission. They were also excluded if they had a history of clinically significant or currently relevant illness, or if they had a history of hypersensitivity to, or malignant syndrome developing from, the administration of antipsychotic compounds.
Women were either of nonchildbearing potential, had been using an oral or injectable contraceptive for at least 1 month before entry into the study, and agreed to continuing using it or another reliable barrier method of contraception during the study. The study was approved by appropriate institutional review boards at each site. Before initiation of any study-related procedure, written informed consent was obtained from all patients who were competent to give it. In the case of patients who were not competent to give informed consent, a pre-existing legal representative consented on their behalf.
Study Design
This randomized, double-blind, fixed-dose, placebo-controlled, parallel-group, multicenter clinical trial was carried out at 34 sites; 32 in the United States and two in Canada. Patients who met the study entry criteria entered a mandatory, single-blind placebo washout period lasting 3 to 7 days. During this washout period, any pre-existing neuroleptic or antidepressant treatment was discontinued. Sedative, anxiolytic, or hypnotic treatments (except lorazepam) were also discontinued or substituted with an appropriate dose of lorazepam. Anticholinergic and β-adrenoceptor antagonist treatment were also withdrawn by reducing the daily dose by one-third each day during the washout period. After washout, patients who still met the study entry criteria were randomized to receive orally either ziprasidone 80 mg/day (given 40 mg BID), ziprasidone 160 mg/day (given 80 mg BID), or placebo for 6 weeks. Patients randomized to receive ziprasidone 160 mg/day received 80 mg/day for the first 2 days of the study, and then received the full dose for the remainder of the study. Patients were to remain in hospital for the first 14 days of the study. Concomitant lorazepam (for insomnia or agitation), benztropine (for extrapyramidal symptoms), and a β-adrenoceptor antagonists (for akathisia) were allowed if required during the study but were not administered prophylactically.
Efficacy Assessments
The following efficacy variables were used to evaluate the efficacy of ziprasidone: PANSS total score (the sum of all 30 items); the PANSS negative subscale score (the sum of the seven negative items on PANSS); the CGI-severity (CGI-S) score, ranging from 1 (normal) to 7 (most severely ill) (National Institutes of Mental Health 1976b), and the CGI-I score. The BPRS (BPRSd) total score was derived from the PANSS, as was the BPRSd core items score (the sum of items P2, conceptual disorganization, P6, suspiciousness, P3, hallucinatory behavior, and G9, unusual thought content). Responder rates based on the PANSS total score (defined as a ≥30% decrease from baseline to last observation) and the CGI-I score (defined as a score of 1, very much improved, or 2, much improved at the last observation) were also determined. The Montgomery-Åsberg Depression Rating Scale (MADRS) (Montgomery and Åsberg, 1979) total score (the sum of all 10 items) was also measured. Discontinuations because of insufficient clinical response and adverse events were recorded.
Efficacy variables, with the exception of MADRS, were measured at baseline (Day 0), and weekly for 6 weeks or on early termination (within 24 hours of receiving the last dose). For CGI-I, the baseline value was based on the comparison with screening, and subsequent weekly assessments were based on comparisons with baseline. The MADRS total score was assessed at baseline and at weeks 1, 2, 3, and 6, or on early termination.
Safety and Tolerability Assessments
All adverse events volunteered and observed during the study or within 6 days of the last day of treatment were recorded using the COSTART dictionary, together with their date of onset, duration, concurrent therapy, the investigator's assessment of severity, and the possible causative relationship to study drug, and whether a change in dose or withdrawal of treatment was required. All serious adverse events were recorded.
Safety assessments were performed at regular intervals or within 24 hours of early termination. Movement disorders were assessed using the 10-item Simpson–Angus Rating scale (Simpson and Angus, 1970), to measure extrapyramidal symptoms (0 = normal to 4 = most severe), the Barnes Akathisia scale (Barnes 1989) to evaluate akathisia (0 = normal to 5 = most severe), and the Abnormal Involuntary Movement Scale (AIMS) (0 = normal to 4 = most severe) (National Institutes of Mental Health 1976c) to evaluate tardive dyskinesia. The Simpson–Angus Rating scale incorporated a new item 7, head rotation, in place of the original item 7, head dropping. The Simpson–Angus Rating and Barnes Akathisia assessments were conducted at baseline and at weeks 1, 3, and 6. The AIMS was assessed at baseline and at week 6. Concomitant use of benztropine, β-adrenoceptor antagonists, and lorazepam was recorded.
Vital signs, including blood pressure (sitting and standing) and pulse rate, were measured weekly. A 12-lead ECG was done at baseline and at weeks 2 and 6. Patients were weighed at baseline and at week 6. Clinical laboratory tests, including routine hematology, serum chemistry, urinalysis with microscopic evaluation, and liver function tests, were done at baseline and at weeks 1, 3, and 6.
Serum Ziprasidone Concentrations
Venous blood samples were collected for the determination of serum ziprasidone concentrations before administration of the morning dose of study drug at weeks 1, 2, and 6 (and, in some cases, week 3). Samples were analyzed using a validated high-pressure liquid chromatography (HPLC) assay with solid phase extraction and detection by ultraviolet absorption (Janiszewski et al. 1995).
Statistical Analysis
It was estimated that approximately 100 patients per group would be required to detect a difference of five points between the placebo group and a ziprasidone treatment group in the mean change from baseline in the BPRSd total score with at least 80% power and a comparison-wise error rate of 0.05 (two-sided).
The primary statistical analysis used for all efficacy variables was an intention-to-treat (ITT) analysis with the last observation being carried forward (LOCF). All patients with a baseline assessment and at least one postbaseline assessment were included in the ITT LOCF analysis. MADRS scores were calculated for the entire ITT cohort, for the subset of patients with baseline MADRS scores ≥14, and for patients with a primary diagnosis of schizoaffective disorder.
Mean baseline to endpoint changes were compared between the placebo group and each of the ziprasidone groups. Estimates of treatment effects were based on least-squares means derived from an analysis of covariance (ANCOVA) model, with the measured value as the dependent variable and the baseline value as the covariate, with fixed terms for the study centers and treatment. Comparisons between treatments were estimated using least-squares means from a type III sum of squares analysis of PROC GLM of SAS®. Confidence intervals and p-values were derived from a Student's t-test. Responder rate p-values and confidence intervals for the PANSS total score and the CGI-I score and were obtained using normal approximation to binomial, with correction for continuity.
All statistical tests performed were two-sided, and values of test statistics were considered significant if p < .05. No adjustments for multiple comparisons were made to significance levels.
Descriptive statistics were used to compare features of the history of illness, baseline characteristics, the incidence of adverse events and laboratory test abnormalities, discontinuations because of insufficient clinical response, and concomitant use of benztropine, β-adrenoceptor antagonists, and lorazepam among treatment groups. Serum ziprasidone concentrations were summarized as means and standard deviations, but no formal hypothesis testing was performed.
RESULTS
Clinical Characteristics
A total of 440 patients were screened. Of these, 302 (215 men and 87 women) were randomized and received at least one dose of double-blind treatment. Baseline patient characteristics and illness characteristics were generally similar across treatment groups (Table 2). Psychiatric illness history was highly variable within each group, but mean values for each attribute were generally consistent across the treatment groups (Table 2). One exception was the duration of the last psychiatric hospitalization, where the mean value in the ziprasidone 160 mg/day group was considerably greater than those in the other two groups. This was mainly attributable to two patients whose previous psychiatric hospitalizations lasted 900 and 1300 days, respectively. Almost all patients had received antipsychotic treatment in the previous 12 months.
The mean baseline PANSS total and negative subscale scores, BPRSd total and core items scores, as well as the CGI-S scores, indicate that all three treatment groups had moderately severe levels of over-all psychopathology, positive symptoms, and negative symptoms (Table 2). Furthermore, over 50% of patients in each treatment group had clinically significant depression at baseline (MADRS score ≥ 14) (Table 3).
Study Therapy
The median duration (range) of treatment was 36 (2–45), 40 (1–46), and 42 (2–46) days for patients in the placebo, ziprasidone 80 mg/day, and ziprasidone 160 mg/day groups, respectively. The percentage of patients discontinuing because of an insufficient clinical response was lower in the ziprasidone 160 mg/day (15%) and ziprasidone 80 mg/day groups (25%) than in the placebo group (35%). Although infrequent, discontinuations because of adverse events occurred more often in the ziprasidone 160 mg/day group than the other two groups in which they were similar (Table 4). No patient discontinued as a result of a laboratory test abnormality. The percentage of patients who discontinued for other reasons (protocol violation, lost to follow-up, withdrawn consent, failure to meet randomization criteria, or other unspecified reasons) was 15, 23, and 13% in the placebo, ziprasidone 80 mg/day, and ziprasidone 160 mg/day groups, respectively. The majority of patients in each the placebo (92%), ziprasidone 80 mg/day (81%), and ziprasidone 160 mg/day (87%) groups took lorazepam at some time during the study. In all three groups, the percentage of patients who required lorazepam was greatest in the first week and decreased throughout the study.
Efficacy Analysis
Both doses of ziprasidone were statistically significantly more effective than placebo in treating psychosis as measured by reduction between baseline and 6 weeks (endpoint) in all assessments of global, positive, and negative symptoms (p < .05) (Figure 1 ). The efficacy of ziprasidone was also evident when the responses to treatment were expressed as the percentage of patients classified as responders (Figure 2 ). The percentage of patients classified as PANSS responders was significantly greater than placebo (17.6%) in the ziprasidone 160 mg/day group (31.1%, p < .05) and numerically greater in ziprasidone 80 mg/day group, (28.8% p = .09). Similarly, the percentage of patients classified as CGI-I responders was significantly greater than placebo (26.1%) in the ziprasidone 160 mg/day group (42.7%, p < .05) and numerically greater in ziprasidone 80 mg/day group (32.7%, p = .39).

Percentage mean improvement from baseline at 6 weeks In assessments of over-all psychopathology, positive symptoms, and negative symptoms (ITT LOCF)

PANSS total and CGI-I responder rates (ITT LOCF)
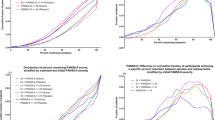
In the all patient group, ziprasidone had no significant effect on MADRS scores (Table 3). However, in patients with clinically significant depressive symptoms at baseline (baseline MADRS ≥ 14; over-all mean 23.5), ziprasidone 160 mg/day produced a statistically significant reduction in MADRS scores as compared with placebo (31.3% vs. 12.6%) (p < .05) (Figure 3 ). In the small subset of patients with schizoaffective disorder, the severity of depressive symptoms at baseline was less than in the subset with baseline MADRS ≥ 14, and ziprasidone 80 mg/day and 160 mg/day were associated with numerically, but statistically, nonsignificantly greater improvements (18.5 and 30.0%, respectively) in depressive symptoms than placebo (11.9%).

Percentage improvement from baseline at 6 weeks in mean MADRS total score in all patients, patients with schizoaffective disorder and in patients with baseline MADRS ≥ 14 (ITT LOCF)
In addition to the analysis of mean baseline to endpoint changes, the time course for symptom improvement was also investigated. At week 1, both the 80 mg/day and 160 mg/day doses of ziprasidone produced reductions from baseline in mean PANSS total, BPRSd total, BPRSd core items, CGI-S, and PANSS negative subscale scores that were statistically significantly greater than placebo (p < .05, Figure 4 ). With few exceptions, further statistically significant improvement compared to placebo was observed at each subsequent weekly assessment in both ziprasidone treatment groups.

Mean change from baseline over time in assessments of over-all psychopathology, positive symptoms, and negative symptoms (ITT LOCF)
Safety–Adverse Events
A total of 264 out of the 302 patients (87%) who received at least one dose of double-blind medication experienced an adverse event (Table 4). The over-all incidence of adverse events associated with ziprasidone was similar to placebo. The majority of treatment-emergent adverse events were of mild or moderate severity. Although infrequent, discontinuations because of adverse events occurred with higher frequency in the ziprasidone 160 mg/day group than the other two groups in which they were similar.
The incidence of individual adverse events was generally very low in all treatment groups (Table 4). Headache was the most frequently reported adverse event, occurring with similar frequency in the ziprasidone 160 mg/day group and placebo groups (31 and 33%, respectively) but with lower frequency in the ziprasidone 80 mg/day group (17%). Overall, the most frequently reported adverse events associated with ziprasidone were somnolence, dizziness, dyspepsia, and nausea (Table 4). Dry mouth occurred with higher frequency in the ziprasidone 160 mg/day group than the other two groups, but constipation was no more frequent than with placebo. Insomnia was less frequent with ziprasidone 80 mg/day and 160 mg/day (12.3 and 11.5%, respectively) than placebo (14.1%). Tachycardia and orthostatic hypotension were very infrequent with ziprasidone (2 and 1% in both groups, respectively). There were no reports of increased body weight as an adverse event, and only two patients in the ziprasidone 80 mg/day group reported an increase in appetite. Notable was the extremely low incidence of dystonia with ziprasidone 160 mg/day (3.8%) relative to placebo (2.2%). Although the incidence of akathisia was higher with ziprasidone than placebo, this was not dose related. The reported incidence of extrapyramidal syndrome (EPS) was 1, 2, and 7% in the placebo, ziprasidone 80 mg/day, and ziprasidone 160 mg/day groups, respectively. Severe EPS occurred in only one patient (160 mg/day group). There was only one report each of male sexual dysfunction and impotence in the ziprasidone 160 mg/day group. No seizures were reported.
One patient discontinued ziprasidone 80 mg/day because of nausea and vomiting, which were not considered related to study treatment by the investigator. Similarly, one patient discontinued ziprasidone 160 mg/day because of fever (and a positive laboratory test for Epstein–Barr virus) not considered to be related to study treatment. One patient in the placebo group was discontinued as a result of an intentional lorazepam overdose. The seven other discontinuations occurred in the ziprasidone 160 mg/day group and were attributable to adverse events considered related to study treatment. Among these cases, three discontinued treatment following a mild adverse event: rash (n = 1); allergic reaction (welts) (n = 1); and dizziness (n = 1). The other four discontinued treatment following a moderate adverse event: rash (n = 2); insomnia (n = 1); and akathisia, parkinsonism, and sedation (n = 1). All adverse events resulting in the discontinuation of ziprasidone therapy resolved within 3 days of the cessation of therapy.
Five, five, and six serious adverse events were reported in the ziprasidone 80 mg/day, ziprasidone 160 mg/day, and placebo groups, respectively. None of these was considered by the investigator to be related to the study drug.
Safety–Movement Disorders
The percentage of patients who required benztropine at any time during the study was 20% in the ziprasidone 80 mg/day group, 25% in the ziprasidone 160 mg/day group, and 13% in the placebo group. The percentage of patients who required β-adrenoceptor antagonists at any time during the study was very low and similar to placebo (6.5%) in both the ziprasidone 80 mg/day (9.4%) and ziprasidone 160 mg/day (5.8%) groups.
There were no notable differences between either ziprasidone group and the placebo group in mean changes between baseline and the last observation in Simpson–Angus, Barnes Akathisia, or AIMS scores (Figure 5 ). These findings persisted when a subgroup analysis of changes from baseline in Simpson–Angus and Barnes Akathisia score was performed for subjects who received, respectively, no benztropine or β-blockers.

Mean change from baseline at 6 weeks in specific assessments of movement disorders (ITT LOCF)
Safety–Cardiovascular and Body Weight
Median changes from baseline to last observation in standing and sitting pulse rate and blood pressure with ziprasidone 80 and 160 mg/day were indistinguishable from placebo. There were only random occurrences of individual patients having clinically relevant changes in these assessments in each group, and no apparent pattern emerged. Compared with placebo, there were no clinically significant mean changes from baseline to last observation in ECG variables. Ziprasidone was indistinguishable from placebo in median changes from baseline to last observation in effects on body weight. Ziprasidone 80 mg/day produced a median increase of 1 kg; whereas, the placebo and ziprasidone 160 mg/day groups produced no change in the median weight.
Safety–Clinical Laboratory Tests
The over-all incidence of abnormalities was similar in the ziprasidone groups and the placebo group, and no clear dose-related effect of ziprasidone was observed (Table 5). No patient discontinued as a result of a laboratory test abnormality.
Changes in liver enzyme levels were notably rare. Only two patients in the ziprasidone 160 mg/day group, and one in the ziprasidone 80 mg/day group, experienced an elevation in plasma SGPT levels (>3 × upper limit of normal). One of the patients in the ziprasidone 160 mg/day group had cytomegalovirus antibody and Epstein–Barr nuclear antigen, and the other had elevated SGPT at baseline, which decreased while on treatment. Therefore, these abnormalities were not judged to be related to ziprasidone. No patient in any group experienced elevations in either blood urea nitrogen (1.3 × upper limit of normal) or creatinine (1.3 × upper limit of normal). There was no evidence of agranulocytosis.
Although the incidence of elevated eosinophils was higher in the ziprasidone 160 mg/day group than the other two groups, the elevations were transient, and the most abnormal value was 15%. Elevation of eosinophils was not associated with rash. There was no median change from baseline to the last observation in eosinophil values in any group. Analysis of the median changes from baseline in other laboratory test variables confirmed the absence of any pattern or dose relationship for laboratory test abnormalities with ziprasidone, any changes being small and balanced across treatment groups.
Ziprasidone Serum Concentrations
Mean (and standard deviation) trough serum ziprasidone concentrations on days 7, 14, 21, and 42 were, respectively, 50 ng/ml (32), 52 ng/ml (38), 35 ng/ml (16), and 47 ng/ml (35) for the 80 mg/day ziprasidone group, and 98 ng/ml (65), 97 ng/ml (58), 98 ng/ml (74), and 109 ng/ml (55) for the 160 mg/day ziprasidone group.
DISCUSSION
This randomized, double-blind, parallel group study compared the efficacy and safety of two fixed doses of ziprasidone, 80 mg/day (n = 106) and 160 mg/day (n = 104), with placebo (n = 92) over 6 weeks in patients hospitalized in 34 North American centers for an acute exacerbation of schizophrenia or schizoaffective disorder. Although the baseline characteristics and clinical histories of the patients in the study population were highly variable, they were balanced among the three treatment groups. The entry criteria ensured that patients were at least moderately ill when randomized to treatment. Baseline assessments confirmed this.
Ziprasidone at dosages of 80 mg/day and 160 mg/day was effective in treating the psychotic manifestations of acute exacerbation of schizophrenia and schizoaffective disorder. Both doses of ziprasidone were statistically significantly superior to placebo in reducing total, positive, negative, and general psychopathology subscales of the PANSS, as well as physicians’ global impressions of illness between baseline and 6 weeks (p < .05). A lower rate of discontinuation because of insufficient clinical response was seen in patients on ziprasidone 160 mg/day (15%) and 80 mg/day (25%) as compared with placebo (35%). Moreover, improvement occurred rapidly. On all measures for ziprasidone 160 mg/day and most measures for 80 mg/day, improvement reached statistical significance at week 1, was clinically observable and generally increased in magnitude subsequently. The benefits of ziprasidone 80 mg/day, which was initiated without dose titration, were apparent by 1 to 3 weeks after the initiation of treatment, indicating that ziprasidone can be initiated at a clinically effective dose.
The effectiveness of ziprasidone was further demonstrated in the analysis of responders on both the PANSS total scale (defined as a ≥30% improvement between baseline and endpoint) and the CGI-I scale (score of 1 or 2 at endpoint). Almost one-third of patients were classified as PANSS responders and over 40% as CGI-I responders in the ziprasidone 160 mg/day group, the difference from placebo being statistically significant for both variables (p < .05). The percentage of patients classified as responders in the ziprasidone 80 mg/day group was also greater than placebo, but did not attain statistical significance for either variable.
Although direct comparisons cannot be drawn across the variations in methodology of different clinical trials, experience with other agents may provide a context in which to view the magnitude of change in symptomatology brought about by ziprasidone. With this in mind, we compared the results of the present study with similar studies of other novel agents in which baseline scores and placebo responses were also similar. In the current study, the mean percentage improvements from ziprasidone 160 mg/day in PANSS total, BPRSd total scores, and PANSS negative symptom subscale (17.9, 18.7, and 16.0%, respectively) were similar to a placebo-controlled, 8-week study of risperidone 6 mg/day in the treatment of schizophrenia, where improvement from baseline on the same scales was 17.2, 17.7, and 13.1%, respectively (Marder and Meibach 1994). The mean improvements in PANSS total, PANSS negative subscale, and CGI-S from baseline with ziprasidone 80 mg/day (12.6, 12.6, and 10.4%, respectively) were of similar magnitude to those observed with olanzapine 10 mg/day (12.5, 10.6, and 12.2%, respectively), in a placebo-controlled, 6-week study (Beasley et al. 1996). Considered in the context of these other agents, the results of this study indicate that ziprasidone 80 and 160 mg/day reduces negative symptoms as well as positive symptoms of acute exacerbations of schizophrenia or schizoaffective disorder, as predicted by its high 5HT2/D2 receptor binding affinity ratio in vitro (Meltzer et al. 1989; Seeger et al. 1995). Although this contrasts with standard neuroleptics that tend to have little or no efficacy in negative symptoms (Möller 1993), it is important to note that the effect of any agent on negative symptoms in acutely ill patients may be, at least in part, attributable to such secondary effects as reductions in positive symptoms and extrapyramidal side effects (Möller et al 1994).
In addition to assessing the effects on over-all psychopathology, positive symptoms, and negative symptoms, the effects of ziprasidone on depressive symptoms were assessed using the MADRS. Depression is a common complication of chronic schizophrenia that can be distinguished from negative psychotic symptoms (Barnes et al. 1989). Depressive symptoms are commonly associated with schizophrenia, and the high prevalence of clinically significant depression at entry observed in the present study is consistent with this well-known association. Estimates of the prevalence of depressive symptoms during acute exacerbations range from 40 to 75% and are similar to the 50% observed in the present study (Johnson 1981; Knights and Hirsch 1981; Koreen et al. 1993; Mauri et al. 1995). Research suggests that depression is not restricted to the postpsychotic phase and may occur at any time in the course of the illness (Bartels and Drake, 1988). A considerable proportion of chronically ill patients (13 to 50%) will also have depressive symptoms, although their psychosis is relatively stable (Barnes et al. 1989; Lindenmeyer et al. 1991; McGlashan and Carpenter 1976), and it has been estimated that approximately 60% of patients with schizophrenia suffer a major depressive episode at sometime during the course of their illness (Martin et al. 1985). Such episodes often lead to suicide (Drake et al. 1985).
The results of this study provide further evidence that depressive symptoms are commonly associated with schizophrenia—over 50% of patients had clinically significant depression at baseline (baseline MADRS ≥ 14, mean 23.5). In these patients, ziprasidone 160 mg/day was associated with a substantial improvement (31.3%) in the mean MADRS score as compared with placebo (12.6%, p < .05) at 6 weeks, which was clinically and statistically significant. In the analysis of patients who had a primary diagnosis of schizoaffective disorder, ziprasidone 160 mg/day and 80 mg/day were associated with appreciable improvements in the mean MADRS scores (30.0 and 18.5%, respectively), as compared with placebo (11.9%), although these were not statistically significant, possibly because of the relatively small sample size (n = 19–24 per treatment group).
The finding that ziprasidone 160 mg/day has a clinically significant effect on depressive symptoms could reflect its unique constellation of activities at serotonergic and adrenergic receptors; potent 5HT1A agonism, potent 5HT1D and 5HT2C antagonism, and ability to moderately inhibit the synaptic re-uptake of serotonin and norepinephrine (Seeger et al. 1995). The effect of ziprasidone on clinically significant depressive symptoms observed in this study clearly warrants further study, because these effects may have been confounded by changes in other domains of psychopathology (such as positive symptoms) in these acutely ill patients. However, it is noteworthy that the antidepressant effects associated with ziprasidone were accompanied by a rapid and significant reduction in psychotic symptoms. In contrast, the treatment of acute schizophrenia with combinations of neuroleptics and antidepressants may be clinically problematic. In combination with neuroleptic treatment, tricyclic antidepressants have been reported to delay the resolution of psychosis (Kramer et al. 1989), and selective serotonin re-uptake inhibitors may exacerbate motor side effects by both pharmacokinetic and pharmacodynamic mechanisms (Meyer et al. 1996).
Overall, ziprasidone was well tolerated, and the total incidence of adverse events and the severity of adverse events associated with each ziprasidone dose was similar to placebo. In the ziprasidone 160 mg/day, 80 mg/day, and placebo groups 7.7, 1.8, and 1.1% of patients were discontinued for adverse events, respectively, and these adverse events resolved within 3 days of cessation of treatment. As anticipated, some adverse events were more frequent with ziprasidone than placebo. Ziprasidone was associated with a higher incidence of somnolence (19% in each group) than placebo (5%). This was generally mild and was noted to subside over the course of the study. Ziprasidone 80 mg/day was associated with a higher incidence of nausea and ziprasidone 160 mg/day with a higher incidence of dyspepsia than placebo. These effects, although not clearly dose related and generally mild, may be related to the serotonergic activities of ziprasidone. They were observed soon after initiation of ziprasidone and were transient. The incidence of dry mouth, but not constipation, was higher with ziprasidone 160 mg/day than with placebo. The higher incidence of dry mouth may be attributable to the higher incidence of benztropine use in patients treated with ziprasidone 160 mg/day, because ziprasidone has negligible intrinsic anticholinergic activity (Seeger et al. 1995).
In view of their relative frequency in association with some other antipsychotic therapies, adverse events that were notable by their low incidence or absence included dystonia, tachycardia, orthostatic hypotension, weight gain, and male sexual dysfunction. The lack of orthostatic hypotension implies that ziprasidone can be initiated at an effective dose, 80 mg/day, without dose-titration. This probably reflects relatively modest affinity of ziprasidone for the α1 receptor, a feature that differentiates it from risperidone, sertindole, and quetiapine (Seeger et al. 1995; Schotte et al. 1996; Bymaster et al. 1996). Although data from direct comparative clinical trials are unavailable, the relatively modest effect of ziprasidone on body weight seems to be in contrast with the significant weight gain reported in acute trials of other newer antipsychotics, such as risperidone, olanzapine, and sertindole (Casey 1996). Although thorough examination of the pharmacological activities that may explain this difference is beyond the scope of this publication, it may be related to ziprasidone's unique collection of serotonergic activities.
The low propensity for ziprasidone to induce movement disorders, shown by the thorough investigation of this phenomenon, is encouraging. The incidence of extrapyramidal symptoms in the present study was much lower than that associated with conventional neuroleptic therapy in the literature (Ortiz and Gershon, 1986; Keepers et al. 1983; Casey and Keepers 1988). This observation is consistent with the findings of another short-term study where ziprasidone in doses up to 160 mg/day were shown to have lower potential to induce movement disorders than haloperidol 15 mg/day (Goff et al. 1998). Although there was evidence of a relationship between ziprasidone 160 mg/day and emergent EPS classified as an adverse event, this was very infrequent (7%). More patients in the ziprasidone 160 mg/day group (25%) and the ziprasidone 80 mg/day group (20%) than in the placebo group (13%) took benztropine during double-blind treatment. Akathisia did not seem to be dose related (placebo: 7%; 80 mg/day: 14%; 160 mg/day 13%). The requirement for β-adrenoceptor antagonist therapy during the study was extremely low and was actually lower in the ziprasidone 160 mg/day group than the placebo group. Mean measures of neuroleptic-induced parkinsonism and akathisia improved or were unchanged as compared with baseline in each treatment group. In addition, only one patient discontinued with movement disorders. Collectively, the investigations of motor side effects undertaken in this study are consistent with the very low propensity for movement disorders predicted by the in vitro receptor binding profile, PET studies, and the relatively low potency for induction of catalepsy (Seeger et al. 1995) and observed in other clinical trials (Goff et al. 1998, Keck et al. 1998).
No patient was discontinued for laboratory abnormalities. No agranulocytosis occurred. The incidence of elevated eosinophils in the ziprasidone 160 mg/day group, and the incidence of elevations in cholesterol levels and urine white blood cell counts in the ziprasidone 80 mg/day group were higher than placebo. These abnormalities were not accompanied by any clinically significant findings.
The paucity of such side effects as EPS, akathisia, sexual dysfunction, and weight gain, which are leading sources of noncompliance in schizophrenia (Van Putten 1974; Young et al. 1986; Pfeiffer et al. 1991; Silverstone et al. 1988), is encouraging, particularly if this is maintained with long-term ziprasidone treatment. Thus, the over-all safety and tolerability profile evidenced in the study seems favorable. The results of the analysis of efficacy are also promising. Ziprasidone at both 80 and 160 mg/day doses rapidly and significantly improved over-all psychopathology, positive symptoms, and negative symptoms in patients with an acute exacerbation of schizophrenia or schizoaffective disorder. Furthermore, ziprasidone was initiated at an effective dose. In addition, ziprasidone 160 mg/day was associated with substantial and significant improvement in depressive symptoms in patients with a clinically relevant level of depression on entry to the study.
Long-term studies in larger populations will determine whether the combination of efficacy in a wide range of symptoms that characterize schizophrenia and an encouraging degree of safety and tolerability observed in the current study can result in improved compliance, lower relapse rates, and greater well-being in patients with schizophrenia. Clinical trials directly comparing the recently developed antipsychotic agents are required to provide definitive data contrasting their efficacy and side-effect profiles.
References
American Psychiatric Association. (1987): Diagnostic and statistical manual of mental disorders, 3rd edition, revised, APA, Washington, DC
Barnes TRE . (1989): A rating scale for drug-induced akathisia. Br J Psych 154: 672–682
Barnes TRE, Curson DA, Liddle PF, Patel M . (1989): The nature and prevalence of depression in chronic schizophrenic inpatients. Br J Psychiatry 154: 486–491
Bartels SJ, Drake RE . (1988): Depressive symptoms in schizophrenia: Comprehensive differential diagnosis. Compr Psychiatry 29: 467–483
Beasley CM, Satterlee W, Sanger T, Tollefson G, Tran P, Hamilton S . (1996): Olanzapine versus placebo: Results of a double-blind, fixed-dose olanzapine trial. Psychopharmacology 124: 159–167
Bench CJ, Lammertsma AA, Dolan RJ, Grasby PM, Warrington SJ, Gunn K, Cuddigan M, Turton DJ, Osman S, Frackowiak RS . (1993): Dose-dependent occupancy of central dopamine D2 receptors by the novel neuroleptic CP-88,059-01: A study using positron emission tomography and 11C-raclopride. Psychopharmacology 112: 308–314
Bench CJ, Lammertsma AA, Grasby PM, Dolan RJ, Warrington SJ, Boyce M, Gunn KP, Brannick LY, Frackowiak RSJ . (1996): The time course of binding to striatal dopamine D2 receptors by the neuroleptic ziprasidone (CP-88,059-01) determined by positron emission tomography. Psychopharmacology 124: 141–147
Briley M, Moret C . (1993): Neurobiological mechanisms involved in antidepressant therapies. Clin Neuropharmacol 16: 387–400
Brooks EW, Mansbach RS . (1997): Effects of the combined 5-HT2/D2 antagonist ziprasidone on drug-disrupted prepulse inhibition in the rat. Soc Neurosci Abstr 23: 1953
Bymaster FP, Calligaro DO, Falcone JF, Marsh RD, Moore NA, Tye NC, Seeman PW . (1996): Radioreceptor binding profile of the atypical antipsychotic olanzapine. Neuropsychopharmacology 14: 87–96
Casey DE . (1996): Side-effect profiles of new antipsychotic agents. J Clin Psychiatry 57: 40–45
Casey DE, Keepers GA . (1988): Neuroleptic side effects: Acute extrapyramidal syndromes and tardive dyskinesia. In Psychopharmacology: Current Trends. Berlin: Springer, pp 74–93
Deutch AY, Moghaddam B, Innis RB, Krystal JH, Aghajanian GK, Bunney BS, Charney DS . (1991): Mechanisms of action of atypical antipsychotic drugs. Implications for novel therapeutic strategies for schizophrenia. Schiz Res 4: 124–156
Drake RE, Gates C, Whitaker A, Cotton PG . (1985): Suicide among schizophrenics. Compr Psychiat 26: 90–100
Fischman A, Williams SA, Drury C, Etienne P, Rubin R . (1996): Sustained 5HT2 receptor occupancy of ziprasidone using PET ligand [18F]setoperone in healthy volunteers. Eur Neuropsychopharmacol 6: 177
Goff DC, Posever T, Herz L, Simmons J, Kletti N, Lapierre K, Wilner KD, Law GC, Ko GN . (1998): An exploratory haloperidol-controlled dose-finding study of ziprasidone in hospitalized patients with schizophrenia or schizoaffective disorder. J Clin Psychopharmacol 18 (4): 296–304
Janiszewski JS, Fouda HG, Cole RO . (1995): Development and validation of a high-sensitivity assay for an antipsychotic agent, CP-88,059, with solid-phase extraction and narrow-bore high-performance liquid chromatography. J Chromatog 668: 133–139
Johnson DAW . (1981): Studies of depressive symptoms in schizophrenia. Br J Psychiat 139: 89–101
Kay SR, Opler LA, Lindenmeyer JP . (1989): The positive and negative syndrome scale (PANSS): Rationale and standardization. Br J Psychiat 155: 59–65
Keck P, Buffenstein A, Ferguson J, Feighner J, Jaffe W, Harrigan EP, Ziprasidone Study Group. (1998): Ziprasidone 40 mg/day and 120 mg/day in the acute exacerbation of schizophrenia and schizoaffective disorder: A 4-week placebo-controlled trial. Psychopharmacology 140 (2): 173–184
Keepers GA, Clappison VJ, Casey DE . (1983): Initial anticholinergic prophylaxis for neuroleptic-induced extrapyramidal syndromes. Arch Gen Psychiat 40: 1113–1117
Knights A, Hirsch SR . (1981): Revealed depression and drug treatment for schizophrenia. Arch Gen Psychiat 38: 806–811
Koreen AR, Siris SG, Chakos M, Alvir J, Mayerhoff D, Lieberman J . (1993): Depression in first-episode schizophrenia. Am J Psychiat 160: 1643–1648
Kramer MS, Vogel WH, DiJohnson C, Dewey DA, Sheves P, Cavicchia S, Little P, Schmidt R, Kimes I . (1989): Antidepressants in “depressed” schizophrenic inpatients. A controlled trial. Arch Gen Psychiat 46: 922–928
Lindenmeyer J-P, Grochowski S, Kay SR . (1991): Schizophrenic patients with depression: Psychopathological profiles and relationship with negative symptoms. Compr Psychiat 32: 528–533
Lu Y, Zorn SH, Rollema H . (1997): Comparison of the novel antipsychotic ziprasidone with clozapine: Effects on dopamine release in rat prefrontal cortex and dorsolateral striatum. Soc Neurosci Abstr 23: 1931
Marder SR, Meibach RC . (1994): Risperidone in the treatment of schizophrenia. Am J Psychiat 151: 825–835
Martin RL, Cloninger CR, Guze SB, Clayton PJ . (1985): Frequency and differential diagnosis of depressive syndromes in schizophrenia. J Clin Psychiat 46: 9–13
Matsubara S, Matsubara R, Kusumi I, Koyama T, Yamashita I . (1993): Dopamine D1, D2 and serotonin2 receptor occupation by typical and atypical antipsychotic drugs in vivo. J Pharmacol Exp Ther 265: 498–508
Mauri MC, Bravin S, Fabiano L, Vanni S, Boscati L, Invernizzi G . (1995): Depressive symptoms and schizophrenia: A psychopharmacological approach. L'Encéphale 21: 555–558
McGlashan TH, Carpenter WT . (1976): Postpsychotic depression in schizophrenia. Arch Gen Psychiat 33: 231–239
Meltzer HY . (1995): Role of serotonin in the action of atypical antipsychotic drugs. Clin Neurosci 3: 64–75
Meltzer HY, Shigero M, Lee JC . (1989): The ratios of serotonin 2 and dopamine 2 affinities differentiate atypical and typical antipsychotic drugs. Psychopharmacol Bull 25: 390–392
Metropolitan Life Insurance Company. (1993): Height and Weight Standards
Meyer MC, Baldessarini RJ, Goff DC, Centorrino F . (1996): Clinically significant interactions of psychotropic agents. Drug Saf 15: 333–346
Möller HJ . (1993): Neuroleptic treatment of negative symptoms in schizophrenic patients. Efficacy problems and methodological difficulties. Eur Neuropsychopharmacol 3: 1–11
Möller HJ, Van Praag H, Aufdembrinke B, Working Group on Negative Symptoms in Schizophrenia. (1994): Negative symptoms in schizophrenia: Considerations for clinical trials: Working Group on Negative Symptoms in Schizophrenia. Psychopharmacology 115: 221–228
Montgomery S, Åsberg M . (1979): A new depression scale designed to be sensitive to change. Br J Psychiat 134: 382–389
Moore NA, Calligaro DO, Wong DT, Bymaster F, Tye NC . (1993): The pharmacology of olanzapine and other new antipsychotic agents. Curr Opin Investiga Drugs 24: 281–293
National Institutes of Mental Health. (1976a): Clinical Global Impression Improvement Scale. In Guy W (ed), ECDEU Assessment Manual for Psychopharmacology
National Institutes of Mental Health. (1976b): Clinical Global Impression Severity Scale. In Guy W (ed), ECDEU Assessment Manual for Psychopharmacology
National Institutes of Mental Health. (1976c): Abnormal Movement Scale. In Guy W (ed), ECDEU Assessment Manual for Psychopharmacology
Neal-Beliveau BS, Joyce JN, Lucki I . (1993): Serotonergic involvement in haloperidol-induced catalepsy. J Pharmacol Exp Ther 265: 201–217
Newman-Tancredi A, Chaput C, Verriele L, Millan MJ . (1996): Clozapine is a partial agonist at cloned, human serotonin 5-HT1A receptors. Neuropharmacology 35: 119–121
Niemegeers CJE, Janssen PAJ . (1979): A systematic study of the pharmacological activities of dopamine antagonists. Life Sci 24: 2201–2215
Ortiz A, Gershon S . (1986): The future of neuroleptic psychopharmacology. J Clin Psychiat 47: 3–11
Pfeiffer W, Kockott G, Fischl B, Schleuning G . (1991): Adverse effects of long-term psychopharmacologic therapy on sexual functions. Psychiatrische Praxis 18: 92–98
Reynolds LS, Braselton JP, Sprouse JS . (1997): Ziprasidone, unlike olanzapine, inhibits 5-HT neuronal activity by a 5-HT1A mechanism. Soc Neurosci Abstr 23: 1931
Rickels K, Schweizer E . (1993): The treatment of generalized anxiety disorder in patients with depressive symptomology. J Clin Psychiat 54: 20–22
Schotte A, Janssen PFM, Gommeren W, Luyten WHML, Van Gompel P, Lesage AS, De Loore K, Leysen JE . (1996): Risperidone compared with new and reference antipsychotic drugs: In vitro and in vivo receptor binding. Psychopharmacology 124: 57–73
Seeger TF, Seymour PA, Schmidt AW, Zorn SH, Schulz DW, Lebel LA, McLean S, Guanowsky V, Howard HR, Lowe JA, Heym J . (1995): Ziprasidone (CP-88,059): A new antipsychotic with combined dopamine and serotonin receptor antagonist activity. J Pharmacol Exp Ther 275: 101–113
Seeman P, van Tol HHM . (1993): Dopamine receptor pharmacology. Curr Opin Neurol Neurosurg 6: 602–608
Sharma RP, Shapiro LE . (1996): The 5-HT1A receptor system: Possible implications for schizophrenic negative symptomatology. Psychiat Anns 26: 88–92
Silverstone T, Smith G, Goodall E . (1988): Prevalence of obesity in patients receiving depot antipsychotics. Br J Psychiat 153: 214–217
Simpson GM, Angus JWS . (1970): A rating scale for extrapyramidal side effects. Acta Psychiat Scand 212: 11–19
Stockmeier CA, DiCarlo JJ, Zhang Y, Thompson P, Meltzer HY . (1993): Characterization of typical and atypical antipsychotic drugs based on in vivo occupancy of 5HT2 and D2 receptors. J Pharmacol Exp Ther 266: 1375–1384
Tandon R, Harrington E, Zorn SH . (1997): Ziprasidone: a novel antipsychotic with unique pharmacology and therapeutic potential. J Serotonin Research 4: 159–177
Van Putten T . (1974): Why do schizophrenic patients refuse to take their drugs? Arch Gen Psychiat 31: 67–72
Young JL, Zonana HV, Shepler L . (1986): Medication noncompliance in schizophrenia: Codification and update. Bull Am Acad Psychiat Law 14: 105–122
Acknowledgements
This study was sponsored by Central Research Division, Pfizer Inc, Groton, CT, U.S.A. The authors and the study sponsor thank all the investigators in the Ziprasidone Study Group, and the patients, and their families, who participated in this study. The following investigators comprise the Ziprasidone Study Group: Rajiv Tandon, University of Michigan Medical Center Department of Psychiatry Ann Arbor, MI, USA; Cecilia Peabody, Veterans Administration Medical Center, Menlo Park, CA, USA; Alan Buffenstein, The Queens Medical Center, Honolulu, HI, USA; Harold Harsch, John L Doyne Hospital, Milwaukee, WI, USA and Mental Health Center, Milwaukee, WI, USA; James Ferguson and Robert Nash, United States Veterans Administration Hospital, Salt Lake City, UT, USA and CPC Olympus View, Salt Lake City, UT, USA and Wyoming State, Evanston, WY, USA; Sheldon Preskorn, Psychiatric Research Institute, Wichita, KS, USA; Richard Borison, Neuropsychopharmacology Unit, Medical Center, Augusta, GA, USA and Georgia Regional Hospital Oak Unit, Augusta, GA, USA; Mauricio Tohen, McLean Hospital, Belmont, MA, USA; James Claghorn and Michael Lesem, Claghorn-Lesem Research Clinic Inc, Bellaire, TX, USA and HCA Medical Center Hospital, Houston, TX, USA and Charter Hospital of Sugar Land, Sugar Land, TX, USA and West Oaks Hospital, Houston, TX, USA; George Jaskiw, Brecksville Veterans Administration Medical Center, Brecksville, OH, USA; Charles Merideth, Alvarado Parkway Institute, Le Mesa, CA, USA and Charter Behavioral Health Systems of San Diego, Alvarado Parkway Institute, La Mesa, CA, USA and Bayview Hospital, Chula Vista, CA, USA and Harbor View Medical Center, San Diego, CA, USA and Affiliated Research Institute, San Diego, CA, USA; S Craig Risch, Institute of Psychiatry-3N, Medical University of South Carolina, Charleston, SC, USA and Charleston Memorial Hospital, Charleston, SC, USA; Michael Sernyak, Connecticut Mental Health Center, New Haven, CT, USA; James Lohr, San Diego Veterans Affairs Medical Center, Psychiatry Service 116A, San Diego, CA, USA; Louis Fabre, Fabre Research Clinics Incorporated, Houston, TX, USA; William Burke, University of Psychiatric Services, University of Nebraska Medical Center, Omaha, NE, USA and Veterans Administration Medical Center, Omaha, NE, USA; Carl Houck, University of Alabama at Birmingham, Department of Psychiatry, Birmingham, AL, USA and University of Alabama at Birmingham, Clinical Research, Birmingham, AL, USA; John Carman, Carman Research, 4000 Cumberland Parkway, Building 100, Suite A, Atlanta, GA, USA; Donald Addington, Calgary General Hospital, Calgary Alberta, Canada and Foothills Hospital, Calgary Alberta, Canada; Matthew Byerly, Psychiatric Specialty Clinic, University of Florida Shands Clinic, Shands Hospital, Gainesville, FL, USA and Psychotic Disorders Program, Gainesville Veterans Affairs Medical Center, Gainesville, FL, USA; Louis Kirby, Thunderbird Samaritan Behavioral Health Center, Glendale, AZ, USA; Mary Ann Knesevich, Terrell State Hospital, Terrell, TX, USA and Charter Grapevine Behavioral Health System, Grapevine, TX, USA and St Paul Medical Center at Southwestern Medical Center, Dallas, TX, USA; Herbert Meltzer, University Hospitals of Cleveland, Case Western Reserve, University School of Medicine, 2040 Abington Road, Cleveland, OH, USA and University Hospitals of Cleveland, Case Western Reserve, University School of Medicine, 11100 Euclid Avenue, Cleveland, OH, USA; Jorg Pahl, Board of Regents of the University of Oklahoma, Health Sciences Center, Department of Psychiatry, Oklahoma City, OK, USA and Pahl Brain Associates PC, 13301 North Meridian, Suite 101, Oklahoma City, OK, USA and Deaconess Hospital, Oklahoma City, OK, USA and Bethany Pavilion, 76000 Northwest 23rd Street, Bethany, OK, USA; David Garver and Jay Griffith, Dallas Veterans Affairs Medical Center, 4500 South Lancaster Road, Dallas, TX, USA and Veteran Affairs Medical Center, 4500 South Lancaster Road 116A, Dallas, TX, USA; Alan Gelenberg, University of Arizona Health Sciences Center, Tucson, AZ, USA; Roger Hammond, University of New Mexico, School of Medicine, Department of Psychiatry, Albuquerque, MN, USA; Uriel Halbreich, State University of New York at Buffalo, Clinical Center BB 170, Buffalo, NY, USA and Buffalo General Hospital, Buffalo, NY, USA and Erie County Medical Center, Buffalo, NY, USA; Kevin McKenna, Caritas Health Group, Grey Nuns Hospital, Edmonton Alberta, Canada; Jambur Ananth, Harbor-University of California, Los Angeles Medical Center, Torrance, CA, USA; G Michael Shehi, Mountain View Hospital, Gadsden, AL, USA. We also thank Dr. Stevin H. Zorn for assistance in compiling data for the receptor binding table.
Author information
Authors and Affiliations
Consortia
Rights and permissions
About this article
Cite this article
Daniel, D., Zimbroff, D., Potkin, S. et al. Ziprasidone 80 mg/day and 160 mg/day in the Acute Exacerbation of Schizophrenia and Schizoaffective Disorder: A 6-Week Placebo-Controlled Trial. Neuropsychopharmacol 20, 491–505 (1999). https://doi.org/10.1016/S0893-133X(98)00090-6
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1016/S0893-133X(98)00090-6
Keywords
This article is cited by
-
Antipsychotics for negative and positive symptoms of schizophrenia: dose-response meta-analysis of randomized controlled acute phase trials
npj Schizophrenia (2021)
-
Meta-analysis of Dropout Rates in Placebo-Controlled Randomized Clinical Trials of Atypical Antipsychotics Assessed by PANSS
Clinical Drug Investigation (2019)
-
Long-term metabolic effects of aripiprazole, ziprasidone and quetiapine: a pragmatic clinical trial in drug-naïve patients with a first-episode of non-affective psychosis
Psychopharmacology (2018)
-
Meta-analysis of Placebo Response in Randomized Clinical Trials of Antipsychotic Drugs Using PANSS Focusing on Different Approaches to the Handling of Missing Data
Clinical Drug Investigation (2018)
-
Clinical Pharmacokinetics of Atypical Antipsychotics: An Update
Clinical Pharmacokinetics (2018)
