
Abstract
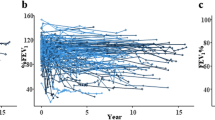
This prospective study focused on risk factors and clinical outcome of pulmonary and cardiac late effects after allogeneic hematopoietic stem cell transplantation (allo-HSCT). We prospectively evaluated 162 children by pulmonary function tests (PFTs) and cardiac shortening fraction (SF) before allo-HSCT and yearly up to the 5th year of follow-up. The 5-year cumulative incidence of lung and cardiac impairment was 35 (hazard rate=0.03) and 26% (hazard rate=0.06), respectively. Patients presenting abnormal PFTs and SF at last follow-up were 19 and 13%, respectively, with a median Lansky performance status of 90% (70–100). Chronic graft-versus-host disease (c-GVHD) was the major risk factor for reduced lung function in univariate (P=0.02) and multivariate analysis (P=0.02). Total body irradiation (TBI) alone and TBI together with pre-transplant anthracycline administration were significant risk factors for reduced cardiac function in univariate analysis, only (P=0.04 and 0.004, respectively). In conclusion, our prospective study demonstrates an asymptomatic post-allo-HSCT deterioration of pulmonary and cardiac function in some long-term survivors, who had been transplanted in childhood, and thus emphasizes the need for lifelong cardiopulmonary monitoring and the development of new strategies both to reduce pre-transplant cardiotoxic regimens and to treat more efficiently c-GVHD.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others
References
Rubin P, Van Houtte P, Constine L . Radiation sensitivity and organ tolerances in pediatric oncology: a new hypothesis. Front Radiat Ther Oncol 1982; 16: 62–82.
Flowers ME, Deeg HJ . Delayed complications after hematopoietic cell transplantation. In: Blume KG, Forman SL, Appelbaum FR (eds). Thomas' Hematopoietic Cell Transplantation. Blackwell Publishing: Oxford, UK, 2004.
Atkinson K, Turner J, Biggs JC, Dodds A, Concannon A . An acute pulmonary syndrome possibly representing acute graft-versus-host disease involving the lung interstitium. Bone Marrow Transplant 1991; 8: 231–234.
Cooke KR, Krenger W, Hill G, Martin TR, Kobzik L, Brewer J et al. Host reactive donor T cells associated with lung injury after experimental allogeneic bone marrow transplantation. Blood 1998; 106: 2571–2580.
Crawford SW, Pepe M, Lin D, Benedetti F, Deeg HJ . Abnormalities of pulmonary function tests after bone marrow transplantation predict non relapse mortality. Am J Resp Crit Care Med 1995; 152: 690–695.
Rovelli A, Pezzini C, Silvestri D, Tana F, Galli MA, Uderzo C . Cardiac and respiratory function after bone marrow transplantation in children with leukemia. Bone Marrow Transplant 1995; 16: 571–576.
Soubani AO, Miller KB, Hassoun PM . Pulmonary complications of bone marrow transplantation. Chest 1996; 109: 1066–1077.
Nicolini B, Rovelli A, Uderzo C . Cardiotoxicity in children after bone marrow transplantation. Med Pediatr Oncol 2000; 17: 203–209.
Bearman SI, Petersen FB, Schor RA, Denney JD, Fisher LD, Appelbaum FR et al. Radionucleotide ejection fractions in the evaluation of patients being considered for bone marrow transplantation: risk for cardiac toxicity. Bone Marrow Transplant 1990; 5: 173–177.
Larsen RL, Barber G, Heise C, August CS . Exercise assessment of cardiac function in children and young adults before and after bone marrow transplantation. Pediatrics 1992; 89: 722–729.
Lele SS, Durrant STS, Atherton JS, Moore TD, Thomson HL, Khafagi FA et al. Demonstration of late cardiotoxicity following bone marrow transplantation by assessment of exercise diastolic filling characteristics. Bone Marrow Transplant 1996; 17: 1113–1118.
Pihkala J, Saarinen UM, Lundstrom U, Salmo M, Virkola K, Virtanen K et al. Effects of bone marrow transplantation on myocardial function in children. Bone Marrow Transplant 1994; 13: 149–155.
Eames GM, Crosson J, Steinberger J, Steinbuch M, Krabill K, Bass J et al. Cardiovascular function in children following bone marrow transplant: a cross-sectional study. Bone Marrow Transplant 1997; 19: 61–66.
Sakata-Yanagimoto M, Kanda Y, Nakagawa M, Asano-Mori Y, Kandabashi K, Izutsu K et al. Predictors for severe cardiac complications after hematopoietic stem cell transplantation. Bone Marrow Transplant 2004; 33: 1043–1047.
Hankinson JL, Bang KM . Acceptability and reproducibility criteria of the American Thoracic Society as observed in a sample of a general population. Am Rev Respir Dis 1991; 143: 516–525.
Gardner RM, Hankinson JL, Clausen L, Crapo RO, Johnson RL, Epler GR . Standardisation of spirometry: 1987 update. Official statement of the American Thoracic Society. Am Rev Respir Dis 1987; 136: 1285–1298.
Marubini E, Valsecchi MG . Analysing Survival Data from Clinical Trials and Observational Studies. Wiley & Sons: Chichester, NY, 1995.
Agresti A . Categorical Data Analysis. Wiley & Sons: New York, NY, 1990.
Armitage P, Berry G . Statistical Methods in Medical Research, 2nd edn. Blackwell Scientific Publications: Oxford, London, 1987.
Kaplan EL, Meier P . Non-parametric estimation from incomplete observation. J Am Stat Assoc 1958; 53: 457–481.
Bearman SI, Appelbaum F, Buckner CD, Petersen FB, Fisher LD, Clift RA et al. Regimen related toxicity in patients undergoing bone marrow transplantation. J Clin Oncol 1988; 6: 1562–1568.
Kupari M, Volin L, Suokas A, Hekali P, Ruutu T . Cardiac involvement in bone marrow transplantation: serial changes in left ventricular size, mass and performance. Bone Marrow Transplant 1990; 5: 259–266.
Socié G, Salooja N, Cohen A, Rovelli A, Carreras E, Locasciulli A et al. Non-malignant late effects after allogeneic stem cell transplantation. Blood 2003; 101: 3373–3385.
Marras T, Szalai JP, Chan CK, Lipton JH, Messner HA, Laupacis A . Pulmonary function abnormalities after allogeneic bone marrow transplantation: a systematic review and assessment of an existing predictive instruments. Bone Marrow Transplant 2002; 30: 599–607.
Palmas A, Tefferi A, Myers JL, Scott JP, Swensen SJ, Chen MG . Late-onset non infectious pulmonary complications after allogeneic bone marrow transplantation. Brit J Haematol 1998; 100: 680–687.
Leneveu H, Bremont F, Rubie H, Peyroulet MC, Broue A, Suc A . Respiratory function in children undergoing bone marrow transplantation. Pediatr Pulmonol 1999; 28: 31–38.
Kaplan EB, Wodell RA, Wilmott RW, Leifer B, Lesser ML, August CS . Late effects of bone marrow transplantation in pulmonary function in children. Bone Marrow Transplant 1994; 14: 613–621.
Freudenberger TD, Madtes DK, Randall Curtis J, Cummings P, Storer BE, Hackman RC . Association between acute and chronic graft-versus-host disease and bronchiolitis obliterans organizing pneumonia in recipients of hematopoietic stem cell transplants. Blood 2003; 102: 3822–3828.
Fraser CJ, Bhatia S, Ness K, Carter A, Francisco L, Arora M et al. Impact of chronic graft-versus-host disease on the health status of hematopoietic cell transplantation survivors: a report from the Bone Marrow Transplant Survivor Study. Blood 2006; 108: 2867–2873.
Reiter A, Schrappe M, Ludwig WD, Hiddemann W, Sauter S, Henze G et al. Chemotherapy in 998 unselected childhood acute lymphoblastic leukemia patients. Results and conclusions of the multicenter trial ALL-BFM 86. Blood 1994; 4: 3122–3133.
Balduzzi A, Valsecchi MG, Uderzo C, De Lorenzo P, Klingebiel T, Peters C et al. Chemotherapy versus allogeneic transplantation in childhood very high risk acute lymphoblastic leukaemia in first complete remission: a comparison by genetic randomization in an International Prospective Study. Lancet 2005; 366: 635–642.
Khadadah ME, Jayakrishnan B, Al-Gorair S, Al-Maradni N, Onadeko B, Malaviya AN . Effect of methotrexate on pulmonary function in patients with rheumatoid arthritis-a prospective study. Rheumatol Int 2002; 22: 204–207.
Lateef O, Shakoor N, Balk RA . Methotrexate pulmonary toxicity. Expert Opin Drug Saf 2005; 4: 723–730.
Kharasch VS, Lipsitz S, Santis W, Hallowell JA, Goorin A . Long-term pulmonary toxicity of multiagent chemotherapy including bleomycin and cyclophosphamide in osteosarcoma survivors. Med Pediatr Oncol 1996; 27: 85–91.
Gillespie AM, Lorigan PC, Radstone CR, Waterhouse JC, Coleman RE, Hancock BW . Pulmonary function in patients with trophoblastic disease treated with low-dose methotrexate. Brit J Cancer 1997; 76: 1382–1386.
Chien JW, Martin PJ, Gooley TA, Flowers ME, Heckbert SR, Nichols WG et al. Airflow obstruction after myeloablative allogeneic hematopoietic stem cell transplantation. Am Resp Crit Care Med 2003; 168: 208–214.
Lipshultz SE, Sallan SE . Cardiovascular abnormalities in long-term survivors of childhood malignancy. J Clin Oncol 1993; 11: 1199–1203.
Colan SD, Parness IA, Spevak PJ, Sanders SP . Development modulation of myocardial mechanism: age and growth-related alterations in afterload and contractility. J Am Coll Cardiol 1992; 19: 619–629.
Lipshultz SE, Lipsitz SR, Mone SM, Goorin AM, Sallan SE, Sanders SP et al. Female sex and higher drug dose as risk factors for late cardiotoxic effects of doxorubicin therapy for childhood cancer. New Engl J Med 1995; 332: 1738–1743.
Kremer LC, van der Pal HJ, Offringa M, van Dalen EC, Voute PA . Frequency and risk factors of subclinical cardiotoxicity after anthracycline therapy in children: a systematic review. Ann Oncol 2002; 13: 819–829.
Iarussi D, Indolfi P, Casale F, Martino V, Di Tullio MT, Calabro R . Anthracycline-induced cardiotoxicity in children with cancer: strategies for prevention and management. Pediatr Drugs 2005; 7: 67–76.
Lipshultz SE, Rifai N, Dalton VM, Levy DE, Silverman LB, Lipsitz SR et al. The effect of dexrazoxane on myocardial injury in doxorubicin-treated children with acute lymphoblastic leukaemia. New Engl J Med 2004; 8: 145–153.
Uderzo C, Cavatorta E, Trocino G, Rovelli A, Longoni D, Viganò E et al. Role of echodobutamine in the evaluation of cardiac disfunction in children more than 10 years after bone marrow transplantation. Bone Marrow Transplant 2004; 1: 218 (Suppl. abstr 033).
De Wolf D, Suys B, Maurus R, Benoit Y, Verhaoren H, Matthijs D et al. Dobutamine stress echocardiography in the evaluation of late anthracycline cardiotoxicity in childhood cancer survivors. Pediatr Res 1996; 39: 504–512.
Smibert E, Carlin JB, Vidmar S, Wilkinson LC, Newton M, Weintraub RG . Exercise echocardiography reflects cumulative anthracycline exposure during childhood. Pediatr Blood Cancer 2004; 42: 556–562.
Hogarty AN, Leabey A, Zhao H, Hogarty M, Bunin N, Cnaan A et al. Longitudinal evaluation of cardiopulmonary performance during exercise after bone marrow transplantation in children. J Pediat 2000; 136: 311–317.
Acknowledgements
The principal investigator is indebted to Professor Hans-Jochem Kolb (Munich) for his contribution in the early stage of the project and Joanna Upton for reviewing the paper. We would like to thank Dr Jakob Passweg (Basel) and Professor Maria Grazia Valsecchi (Monza) for their assistance in statistical analysis. This work was partially presented at the 47th Annual ASH meeting (Atlanta, USA, 10–13 December, 2005).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Uderzo, C., Pillon, M., Corti, P. et al. Impact of cumulative anthracycline dose, preparative regimen and chronic graft-versus-host disease on pulmonary and cardiac function in children 5 years after allogeneic hematopoietic stem cell transplantation: a prospective evaluation on behalf of the EBMT Pediatric Diseases and Late Effects Working Parties. Bone Marrow Transplant 39, 667–675 (2007). https://doi.org/10.1038/sj.bmt.1705652
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705652
Keywords
This article is cited by
-
Cardiac and obstetric outcomes of pregnancies for women after cardiotoxic therapy in childhood: a single center observational study
BMC Cancer (2023)
-
Transplant characteristics and self-reported pulmonary outcomes in Swiss childhood cancer survivors after hematopoietic stem cell transplantation—a cohort study
Bone Marrow Transplantation (2021)
-
Cardiovascular disease and its management in children and adults undergoing hematopoietic stem cell transplantation
Journal of Thrombosis and Thrombolysis (2021)
-
Late effects of pediatric hematopoietic stem cell transplantation on left ventricular function, aortic stiffness and myocardial tissue characteristics
Journal of Cardiovascular Magnetic Resonance (2019)
-
Long-term Effects of Myeloablative Allogeneic Hematopoietic Stem Cell Transplantation in Pediatric Patients with Acute Lymphoblastic Leukemia
Current Oncology Reports (2018)
