
Key Points
-
Resorption of permanent teeth can be a significant complication of ectopic tooth development.
-
Ectopic tooth development should be suspected in patients presenting with a tooth or teeth missing from the arch.
-
Appropriate radiographs should be undertaken to identify and locate such teeth.
Abstract
This case report highlights the importance of careful clinical and radiographic examination to identify developmental abnormalities before commencing orthodontic treatment.
Similar content being viewed by others

Introduction
Root resorption is a well recognised phenomenon associated with impacted or unerupted teeth. This has been well documented in cases of ectopic canines1 or anterior supernumeraries which can pose a threat to the incisor roots and impacted third molars which can cause resorption of second molars.2 However, there have been few case reports of the resorption of permanent first molar roots by unerupted premolars.
Case report
A 14-year-old girl with no relevant medical history was referred to East Surrey Hospital by her general dental practitioner for an orthodontic opinion regarding the congenital absence of the lower left second premolar and crowding in the upper right quadrant with lack of space for eruption of the upper right second premolar. The patient was happy with her appearance but complained of an occasional dull ache from the upper right first permanent molar on biting.
On examination the patient presented with a crowded class I malocclusion in the permanent dentition with a retained lower left second deciduous molar. In the upper right quadrant there was a full unit of space loss with UR4 and UR6 in contact and an upper centre line shift to the right. UR5 was not palpable. UR6 exhibited slight mobility and tenderness to percussion (Fig. 1).

Crowded upper arch with missing upper right second premolar
Radiographic examination
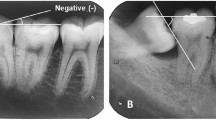
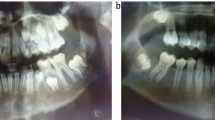
Dental panoramic tomograph (Fig. 2) confirmed developmental absence of the lower right second premolar and showed an impacted UR5 directly above the crown of UR6. The radiographic appearance, together with the clinical examination and history, suggested root resorption of UR6. A periapical radiograph (Fig. 3) was taken to provide enhanced detail of the area and identified the impacted UR5 lying directly above UR6 with possible resorption of UR6 affecting the roots and pulp chamber.

DPT showing impacted upper right second premolar directly above upper right permanent first molar and developmental absence of LL5.

Periapical radiograph confirms root resorption of UR6 by UR5.
Treatment
A diagnosis of resorption of the roots of the UR6 due to ectopic development of UR5 was made, and the decision was taken to remove UR6 and allow UR5 to erupt in its place.
Following LA extraction of the UR6, extensive resorption of the palatal root was evident, together with some medial resorption of the buccal roots and pulpal exposure (Fig. 4).

Extracted UR6 showing extensive root resorption.
Follow up
The patient was reviewed three months post-extraction. UR5 had erupted in the UR6 position with a distopalatal rotation and a brown spot lesion on its occlusal surface (Fig. 5). The patient remained happy with the appearance of her teeth and did not wish to have orthodontic treatment.

UR5 erupted in UR6 position with distopalatal rotation.
Discussion
Buccal segment crowding due to tooth/arch size discrepancy or resulting from early loss of second deciduous molars may lead to insufficient space for the second premolars to erupt in the line of the arch. The second premolar will frequently then erupt in a palatally or lingually displaced position. Therefore, it is valuable to try locating the positioning of the premolar by palpating the surrounding tissues. If no swelling is palpated and the premolar is suspected to be lying in the line of the arch, intra-oral radiographs may be necessary to give enhanced image clarity where there is suspicion of root resorption. Parallax views may also be useful in clarifying tooth position.
Previously documented comparable cases show similar features to this case where the impacted premolars were not palpable in the palate.3,4,5 A further common feature of the cases was intermittent pain.3,5 However, similar cases with no history of pain despite pulp chamber involvement have also been documented.6,7
The marked rotation of the premolar after eruption has also been reported in other similar cases.4,5 In all of the cases the radiographs taken showed overlapping of the first molar root by the impacted second premolar.3,4,5,7,8
In this case it proved impossible to ascertain the aetiology of the crowding in the upper right quadrant as neither the referring general dental practitioner nor the family had any recollection of URE being lost. There was no history of dental extraction. It is likely that early loss of URE occurred either when UR4 erupted or as a result of mesial positioning of UR6 leading to distal root resorption of URE.
This case demonstrates the importance of careful clinical and radiographic assessment to check the condition and presence of all teeth before orthodontic treatment is embarked upon.
References
Ericson S, Kurol J . Incisor root resorptions due to ectopic maxillary canines imaged by computerized tomography: a comparative study in extracted teeth. Angle Orthod 2000; 70: 276–283.
Wang H Y . Root resorption associated with impacted maxillary third molar. Oral Surg Oral Med Oral Pathol 1992; 73: 765–766.
Tracey C, Lee R T . Root resorption: the aggressive, unerupted second premolar. Br Dent J 1989; 166: 19–20.
Harradine N W, Chan K K . Bilateral root-resorption of upper first permanent molars. Primary Dent Care 1995; 2: 23–25.
Sian J S . Root resorption of first permanent molar by a supernumerary premolar. Dent Update 1999; 26: 210–211.
Waterhouse P J, Nunn J H . Crown and root resorption of a maxillary permanent first molar by an impacted second premolar: a case report. Int J Paediatr Dent 1995; 5: 259–262.
Hall F M, Cook P A . Resorption of first mandibular molar. Br Dent J 1989; 166: 19–20.
Baer P N . External resorption associated with tooth eruption. J Clin Pediatr Dent 2001; 25: 123–125.
Acknowledgements
The authors would like to thank Mr R. Sivakumaran, Dental Clinical Director, and Mr A. J. Banner, Consultant Orthodontist, East Surrey Hospital for their advice during the preparation of this paper.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Tabiat-Pour, S., Newlyn, A. Root resorption of a maxillary permanent first molar by an impacted second premolar. Br Dent J 202, 261–262 (2007). https://doi.org/10.1038/bdj.2007.174
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bdj.2007.174
