
Key Points
-
Patients diagnosed with a lack of posterior support should be treatment planned for dental implants to re-establish support.
-
Sufficient restorative space must exist when treatment planning dental implants in posterior quadrants.
-
There are many advantages in designing posterior dental implant restorations to be retrievable.
-
Splinting of multiple posterior implants provides many benefits.
Key Points
Implants
-
1
Rationale for dental implants
-
2
Treatment planning of implants in posterior quadrants
-
3
Treatment planning of implants in the aesthetic zone
-
4
Surgical guidelines for dental implant placement
-
5
Immediate implant placement: treatment planning and surgical steps for successful outcomes
-
6
Treatment planning of the edentulous maxilla
-
7
Treatment planning of the edentulous mandible
-
8
Impressions techniques for implant dentistry
-
9
Screw versus cemented implant supported restorations
-
10
Designing abutments for cement retained implant supported restorations
-
11
Connecting implants to teeth
-
12
Transitioning a patient from teeth to implants
-
13
The role of orthodontics in implant dentistry
-
14
Interdisciplinary approach to implant dentistry
-
15
Factors that affect individual tooth prognosis and choices in contemporary treatment planning
-
16
Maintenance and failures
Abstract
Differences in anatomy and biomechanics make treatment of posterior quadrants with dental implants substantially different to that of anterior areas. Without implants, when posterior teeth were lost, treatment options included a long span fixed partial denture or a removable prosthesis, especially when no terminal abutment was available. Today, with the use of implants, options are available that allow preservation of unrestored teeth.1 When teeth are missing, implant supported restorations can be considered the treatment of choice from the perspective of occlusal support, preservation of adjacent teeth and avoidance of a removable partial denture.
Similar content being viewed by others

Main
From 1993 to the present, single tooth implants have been shown to be the most predictable method of tooth replacement. Multiple studies of at least five years' duration demonstrate a higher survival rate than other methods of tooth replacement.2,3,4,5 Introduction of implants in posterior quadrants reduced the risk of fixed partial dentures which challenged the support available from teeth, the retention and resistance form of abutments and the limitations of the materials available to fabricate these prostheses. Situations where compromised abutment teeth were incorporated into prostheses could be avoided when abutment teeth were not available; long span fixed partial dentures were no longer fabricated. Dental implants allowed the ability to segment the restoration and provide support to the restoration without depending on the abutment teeth. Segmentation brought many advantages including easier fabrication, improved marginal fidelity and retrievability. The purpose of this article is to look at the diagnostic factors that affect treatment planning of dental implants in the posterior quadrants.
When the issue of treatment planning of posterior quadrants arises the choice between conventional dentistry and implants should be based on scientific evidence and objective prosthetically orientated risk and cost assessment. Decisions to salvage questionable teeth should be weighed against the predictability of implant therapy and the efficacy of long term outcomes. Due to advances in bone augmentation techniques, sinus floor elevation and distraction osteogenesis virtually no limits exist to placement of implants. 6,7,8
The broad use of implants in posterior quadrants is not exclusively based on favourable long term reports;3,4,5 other factors such as biomechanical advantages and the availability of prefabricated components have made this treatment modality appealing to the clinician.
Implant retained restorations provide considerable advantages over removable partial dentures. Improved support, a more stable occlusion, preservation of bone and simplification of the prosthesis are a few reasons why implants are the treatment of choice for missing posterior teeth. Additionally, long term oral health is often improved because less invasive restorative procedures are required for the remaining dentition.9
The predictability of the outcome of an implant restoration in the posterior part of the mouth is dependent on many variables including but not limited to the following:
-
1
Available space
-
2
Implant number and position
-
3
Occlusal considerations
-
4
Type of prosthesis
-
5
Overall treatment plan.
Treatment planning considerations
Available space
a. Mesiodistal
Though aesthetics is secondary in restoring the posterior areas of the oral cavity, care should still be taken with implant position to allow restorations that will be functional and as close to the natural dentition as possible, to allow proper development of occlusion and embrasure forms for patient comfort.
Mesiodistal space is evaluated in two dimensions. Adequate prosthetic space must exist to provide the patient with a restoration that mimics natural tooth contours. If inadequate prosthetic space exists, it must be created through enameloplasty of adjacent teeth or orthodontic repositioning (Figs 1,2,3,4)

Inadequate mesiodistal space for implant retained premolar sized restoration

Lateral view showing mesial tilting of molar and osseous defect

Inadequate mesiodistal space for implant restoration

Mesiodistal contours of restoration in first premolar region are compromised
The mesiodistal space required essentially depends on the type of tooth being replaced (molar or premolar), and the number of teeth being replaced. The natural maxillary first and second premolar, and first molar have an average mesiodistal size of 7.1, 6.6 and 10.4 mm respectively. The dimensions of these teeth at the CEJ are 4.8, 4.7 and 7.9 mm. At a distance 2 mm from the CEJ the teeth measure 4.2 mm, 4.1 mm and 7.0 mm.10,11 Decisions need to be made with regards to implant size. The following guidelines should be used when selecting implant size and evaluating mesiodistal space for implant placement:12
-
1
The implant should be at least 1.5 mm away from the adjacent teeth
-
2
The implant should be at least 3 mm away from an adjacent implant
-
3
A wider diameter implant should be selected for molar teeth.
Based on the above for two 4 mm diameter implants a space of 14 mm is required. This amount of space would suffice to replace two premolars. If two premolars and a molar are required an additional space is necessary. This situation can be resolved by placement of two implants and fabrication of an FPD or placement of three implants. In either case a wider diameter implant is required in the molar region (5 mm). If three implants are planned a total space of 23 mm is required.
Similar guidelines should be followed when treatment planning implants in the posterior mandible (Figs 5,6,7,8). The size of the prosthetic tooth must be considered when placing implants; the implant must be placed sufficiently away from the adjacent tooth to allow the restorative dentist to develop appropriate contours. If an implant placed for a premolar restoration is placed too close to the adjacent tooth, compromised contours and unnecessary loss of hard and soft tissue adjacent to the implant result (Figs 9,10,11). Placing the restoration too far from the adjacent tooth also results in unfavourable contours and development of cantilever type forces on the implant (Figs 12,13,14,1516). Treatment planning a premolar restoration requires the surgeon to place the implant 1.5 mm away from the adjacent root (Figs 17-18). Molar teeth are wider mesiodistally and for molar implant restorations the implant needs to be placed 2.5 mm away from the adjacent tooth to allow development of appropriate restorative contours (Figs 19-20). Placing an implant for a molar tooth too close or to far from the adjacent tooth will also result in compromised restorative contours (Fig. 21).

There should be a space of 3 mm between implants

Occlusal view illustrating ideal screw access position for implants placed between teeth

Lateral view of implant restoration in Figure 6 illustrating ideal contours

Clinical view of case in Figure 6

There is also a compromise in the contours of the implant restoration

This results when a surgical guide is not used

Implants are so close together that it is impossible to make an impression with conventional pick-up type impression copings. Custom impression coping have to be fabricated

Implant for premolar tooth placed too far away from adjacent tooth

Diagnostic wax up of implant restoration illustrating compromised contours

Occlusal view illustrates contours and mesial cantilever on implant restoration.

Laboratory view of final restoration illustrating compromised contours

Final restorations illustrating compromised aesthetics and contours

This allows optimum emergence profile to be created

Lateral view of Figure 17 illustrating an aesthetic outcome and optimal contours

The implant needs to be placed at least 2.5 mm away from the adjacent root to allow optimum emergence

Laboratory view illustrating emergence of anticipated restoration from the head of the fixture

If implant for a molar restoration is placed too close to the adjacent tooth, compromised contours result
b. Buccolingual
At least 6 mm of bone buccolingually is required for placement of a 4 mm diameter implant and 7 mm for a wider diameter 5 mm implant. The implants should be placed so that the projection of the fixture is contained within the anticipated crown form. The screw access should be positioned towards the centre of the occlusal surface. Posterior mandibular fixtures should be placed so that the exit angle of the screw access should point towards the inner incline of the palatal cusp. Posterior maxillary implants should be placed so that the exit angle of the screw access points towards the inner incline of the buccal cusp (Fig. 22).

The screw access should be positioned towards the centre of the occlusal surface. Posterior mandibular fixtures should be placed so that the exit angle of the screw access should point towards the inner incline of the palatal cusp. Posterior maxillary implants should be placed so that the exit angle of the screw access points towards the inner incline of the buccal cusp
Correct angulation is always achieved if the surgeon is diligent and makes use of a surgical guide to place implants in the correct position. Placing implants in off angle positions always complicates the process for the restorative dentist who now has to use a host of restorative components to achieve an acceptable end result (Figs 23,24,25,26,27,28,29).

Radiograph illustrating overlap of fixtures and inability to verify seating radiographically

The pick up impression coping has to be modified so an impression can be made. Access is difficult

These should not be an afterthought but rather planned for at the time of surgery. Use of pre-angled abutments will affect the depth of implant placement

A provisional will be fabricated from this wax up

Note un-aesthetic display of metal

Biomechanically this is an unfavourable situation with excessive cantilevering of the prosthesis to maintain appropriate occlusal relationships

This can be avoided by use of an appropriately fabricated surgical guide
c. Occlusogingival
This parameter also needs to be considered in two dimensions:
-
1
Adequate space for restoration
-
2
Adequate osseous volume for placement of the implant.
Adequate space for restoration
Sufficient space must exist to allow the restorative dentist to fabricate restorations which are harmonious aesthetically with the adjacent teeth. On examination the space between the residual ridge and the opposing occlusal plane should be evaluated. Replacing premolar and molar teeth requires 10 mm of space between the residual ridge and the opposing occlusion. 7 mm would be considered the bare minimum (Fig. 30). Often, when teeth are missing for prolonged periods of time, opposing teeth over-erupt and compromise the restorative space. If this is minimal, enameloplasy or minimal restorative therapy may be required to create space. On occasion molar teeth over-erupt to the extent that they contact the opposing residual ridge (Figs 31-32). Orthodontic intrusion of these teeth is a technique-sensitive procedure which requires diligence from both the surgeon and orthodontist. Options include both elective endodontics, crown lengthening and preparation of the tooth for a full coverage restoration. In instances where the root trunk is short, consideration must be given to extraction and implant replacement as an alternative so that sufficient space can be created. Often when space is limited towards the posterior quadrant the patient must be informed that it may not be possible to fabricate restorations to replace all of their missing teeth (Figs 33-34).

Ideally 7-10 mm of space is required from the head of the fixture to the opposing occlusion

Inadequate space in posterior mandibular area for fabrication of a tooth shaped restoration

Inadequate space in posterior mandibular area for fabrication of a tooth shaped restoration

Patient was referred for implant restorations to replace up to the second molar. Inadequate restorative space existed past the first molar

A three unit splinted implant supported restoration was fabricated for the patient in Figure 33
1. Adequate osseous volume for placement of the implant
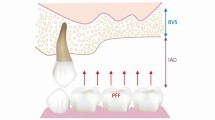
Often the clinician is confronted with single tooth gaps that present all of the pre-requisites for successful implant therapy, with the exception of sufficient vertical bone height. The question arises: what is the minimal height of the implant required to support a posterior restoration? Clinicians have anecdotally used the longest implant possible, being concerned with the ratio between the implant and suprastructure length — the thought process being that an unfavourable implant:suprastructure ratio will cause crestal bone resorption. There are data from prospective multicentre studies to show that shorter implants of 6-8 mm did not show increased crestal bone loss in comparison to longer implants (10-12 mm) and the unfavourable ratio between the implant and the suprastructure did not lead to more pronounced crestal bone resorption.13,14
For a standard protocol 7.5 mm of bone height is required for a 6 mm long fixture and 8.5 mm is required for a 7 mm fixture. Prior to fixture placement the maxillary sinus, inferior alveolar canal and mental foramina must be evaluated by means of a CT scan. There should be at least 2 mm of bone between the apical end of the implant and neurovascular structures. Advances in onlay grafting, distraction osteogenesis and maxillary sinus augmentation allow the surgeon to place implants in sites which were previously contraindicated.6,7,8 Sinus augmentation provides adequate bone volume to place implants but does not correct for vertical space deficiencies (Figs 35-36). The patient must be aware that prosthetically, long teeth with root form or pink porcelain will be required (Fig. 37).

Due to pneumatisation of the sinuses inadequate space sometimes exists for placement of implants in the posterior maxilla

Developments in maxillary sinus augmentation procedures have allowed the clinician to rehabilitate these patients

The patient must accept either a long tooth or incorporation of pink ceramics to disguise the tooth length
The diameter of the implant also plays a role in occluso-gingival placement. Originally wider diameter implants were created as a rescue implant for conditions in which the standard 3.75 mm implant could not be stabilised. For the restorative dentist the wide diameter implant has been a welcome addition. The improved stability, greater surface area and improved force distribution are particular benefits in the posterior part of the mouth where forces are greater. The success with wide diameter implants replacing molar teeth has been documented in clinical studies.15 Certainly the wider diameter implants come closer to replicating the emergence profile of the molar tooth. With regards to placement, use of a standard 4 mm diameter implant for a molar tooth requires the implant to be placed slightly deeper so that an appropriate emergence profile can be developed. The limiting factor in placement may be vital structures, in which case the prosthesis design will require the contours to extend horizontally from the implant. Maintaining hygiene becomes very difficult and some patients may even complain of food entrapment. Use of wider diameter implants allows shallower placement of the implant since the transition in emergence profile from the wider diameter is not as pronounced (Fig. 38).

If a regular body implant is used the same emergence can only be achieved if the implant is placed deeper. This compromises the biology
Clinicians have also advocated placement of two implants in molar positions to compensate for poor bone quality.16 Double implants more closely mimic the anatomy of the roots being replaced and double the anchorage surface area. Other advantages include eliminations of antero-posterior cantilever, reduction of rotational forces exerted and reduction of screw loosening. However, daily oral hygiene may be more difficult and a major limitation in placing two implants is insufficient mesiodistal space.
2. Implant number and position
The number of implants for single molar restorations has been addressed previously. This section will focus on number of implants required for multiple missing teeth.
There is insufficient scientific evidence to guide the practitioner as to how many implants are required to rehabilitate the patient when multiple teeth are missing in posterior quadrants. Most recommendations are derived from traditional prosthodontic experience and are based on clinician experience which is anecdotal.
When three posterior teeth are missing, two or three implants may be required (Figs 39-40). The number of implants is dependent on bone quantity and quality. Often in the maxilla where less dense bone is found, surgeons favour placing three implants — one for each tooth. The rationale for this is primarily restorative. Should one implant of the three fail, the restorative dentist may still continue with the anticipated prosthesis. If anterior or posterior implants were to fail the prosthesis design would include an anterior or posterior cantilever. Cantilever type prostheses have been associated with higher rates of failure in traditional prosthodontics. These types of prosthesis failed due to mechanical complications of the abutment teeth. These types of complications can be controlled with an implant supported prosthesis. Abutments can be optimised for length and taper and connector size can be improved for maximum strength. On occasion, where bone volume is inadequate, the clinician has to decide if a bone augmentation procedure is justified or whether a more simple approach of cantilevering would suffice. Unfortunately there are insufficient data to guide us on making this decision. When cantilevering, the occlusal surface of the cantilever should be minimised and occlusal contact should be controlled so that the majority of the load is distributed along the long axis of the implants. As with traditional prosthodontic protocols, cantilevering forward is much more favourable than cantilevering posterior to the implants. Distal cantilevers have been reported to be unfavourable from a biomechanical point of view and have increased the number of complications for implant supported prostheses.17 If the smile line dictates an additional tooth posteriorly, it is not unreasonable to fabricate a buccal facing which is cantilevered from the implant abutments. This facing should be fabricated without occlusal contact.

Two implants placed to fabricate a three unit fixed partial denture in the mandible

The quality of the bone was inferior to that of Figure 39. A third implant was placed as a precautionary measure
The choice between using two or three implants is also related to the biomechanics of the prosthesis and how load is distributed. With three implants it is possible to offset the implants and position them for a tripod effect. This has been claimed to give a more optimal bone support than a linear arrangement.17 From a practical perspective it is very difficult to place three implants in an absolute linear arrangement and tripoding, to a certain degree, is always likely to occur. If only two implants are placed, use of a wider diameter implant will often provide an equivalent benefit to the non linear configuration.
When insufficient osseous volume exists in the posterior maxilla and the patient does not want to undergo a sinus augmentation procedure, consideration must also be given to implant placement in the tuberosity area (Figs 41,42,43,44). This technique has been described by many authors;18 it provides adequate posterior support and eliminates the potential problems encountered with cantilevers.

Sinus augmentation procedures can be avoided by placement of implants in the maxillary tuberosity area

The implant in the tuberosity area is used for support

Use of the tuberosity area allows the clinician to extend the prosthesis by an additional tooth

Clinical view of Figures 41 to 43
3. Occlusal considerations
Masticatory forces developed by a patient restored with implant supported restorations are equivalent to those of a natural dentition.19 When treatment planning patients for implant supported restorations, a general assessment of the likely load to be placed on the implants should be made. If the patient is a bruxer the clinician may plan additional implants to allow for more favourable load distribution. Complications with dental implants are most often the result of inadequate treatment planning. Consideration of bone density and volume, anticipated loads and planned restorative design are all important to review before number, length and diameter of implants are determined.
Implants, unlike natural teeth, are ankylosed to the surrounding bone without an intervening periodontal ligament. The mean values of axial displacement of teeth in the socket vary between 25-100 microns.20 The range of motion of osseointegrated implants has been reported to be approximately 3-5 microns.21 Displacement of a tooth begins with an initial phase of periodontal compliance that is non linear and complex, followed by a secondary movement phase occurring with the engagement of the alveolar bone.19 In contrast, an implant deflects in a linear and elastic pattern and movement of the implant under load is dependent on elastic deformation of the bone. There are studies supporting the finding that implants are more susceptible to occlusal overloading than natural teeth.22
The types and basic principles of implant occlusion have been derived from occlusal principles of traditional tooth borne restorations. Techniques should be used to minimise excessive loading on implant supported restorations. The occlusion should be evaluated and organised so that there is anterior guidance and disclusion of posterior teeth on lateral excursion. There should be no contact of posterior teeth on both working and non working sides. If the canine is compromised, group function is acceptable. Initial occlusal contact should occur on the natural dentition. The centric contacts are adjusted with light occlusal contact on the implants; the rationale for this is that the opposing natural dentition is often compressed on firm closure.
Cuspal inclinations on implant supported restorations should also be shallower; anterior disclusion is also easier to develop when posterior occlusal anatomy is shallow. As stated previously any type of cantilever force should be minimised, which includes anterior, posterior and buccolingual cantilever. On occasion when there has been extreme resorption of the maxillary bone, teeth may need to be set in a cross bite relationship to minimise offset loads.
When multiple posterior teeth are replaced it is the authors' preference to splint the implants. This is done primarily for biomechanical reasons. Although the total force passed to the crestal bone will be the same for a given load, stress distribution can be manipulated by splinting.23 Splinting also has practical advantages in that there are fewer proximal contacts to adjust.
4. Type of prosthesis
a. Screw retained or cemented
It is the authors' preference to use screw retained restorations wherever possible. Many advantages of prosthesis retrievability can be afforded by screw retention. Retrievability facilitates individual implant evaluation, soft tissue inspection and any necessary prosthesis modifications. Additionally, future treatment considerations can be made more easily and less expensively. Porcelain repair, changing the shade of a restoration and creating additional access for oral hygiene become minor issues if the prosthesis can be easily unscrewed24 (Figs 45,46).

With a screw retained prosthesis, the screw access holes should exit the centre of the tooth

The margins must follow the contours of the gingiva
Many practitioners favour cemented type restorations because this provides a more aesthetic result, as screw access holes can be avoided. With this practice abutment screws must stay tight because a loose screw cannot be easily accessed. A cemented prosthesis may require sectioning to tighten a loose abutment. Clinicians often use temporary cements to facilitate this; however, retrieval even when cemented with provisional cements may not always be predictable.
It is the authors' opinion that aesthetics of screw retained restorations need not be a problem if the clinician explains to the patient the advantages of retrievability and takes proper care to place an aesthetic composite.
The choice for screw retained or cemented restoration will also be influenced by the tooth that is being replaced. The occlusal surface of a premolar is small and patients may object to occlusal access holes in restorations replacing the first and second premolar (Fig. 47). These restorations may be designed to be cement retained. As the restorations are much further forward in the mouth, the biomechanical risk is reduced. When using cement retained restorations in these teeth, caution must be exercised in the design of the custom abutment. Abutments should be designed to follow the contours of the gingiva, meaning that scalloping of the abutment is required in interproximal regions. Circular margins of the restorations will result in the cement margin being deeper in some locations than others. The margin of the abutment should also be kept as minimally subgingival as aesthetics will allow. Placing a cement margin too deep will cause the practitioner difficulty in removal of excess cement. The literature shows that removing all the cement when an implant is placed too deep can prove to be a difficult endeavour. Agar et al.23 found that when six experienced investigators were asked to remove cement there was a surprising amount of cement left behind, which can lead to serious soft tissue complications. An article later on in the series will elaborate on the important differences between screw retained and cemented type prosthesis designs and when each is indicated.

These restorations may be designed to be cement retained. Being that the restorations are much further forward in the mouth the biomechanical risk is reduced
b. Splinted or non-splinted
Whenever multiple implants are placed in posterior quadrants it is the authors' opinion that they should be splinted. Stress distribution can be manipulated by splinting.23 The retention of the prosthesis is also improved with a greater number of splinted abutments. Splinting also has biomechanical advantages in that it will also reduce the incidence of screw loosening and unretained restorations. Practical advantages include fewer proximal contacts to adjust and delivery of the restoration can be performed more efficiently. There is likelihood that when more than three units are splinted, sectioning and soldering will be required to improve fit; this is no different from what is required with a conventional fixed partial denture framework spanning more than three units.
c. Abutment level vs. implant level restoration,segmented vs. non segmented
When implants are aligned to allow screw retention, unless the soft tissue depth is more than 3 mm, implant supported restorations are almost always restored directly to the implant. Screw retained abutments are only used when the implants are placed deeply or soft tissue depth is excessive; the abutment merely facilitates restorative procedures as there is less soft tissue interference when the restorative interface is raised. There are instances when a titanium interface is desired and in these situations abutments can be selected to allow a supra mucosal restorative interface. Disadvantages of this will be that there will be a display of metal on the restoration and there will be less room for transitional contours. At times screw retained pre angled abutments are required, when these are to be used the implant must be planned to be placed deeper to accommodate the thickness of the abutment, use of pre angled abutments should be designed and not be an afterthought.24 Studies have shown that loading to angled implants is not detrimental to implants – however loading implants at an angle can be problematic to the screw joint between the restoration and the abutment.
When cemented restorations are to be used the abutments placed should embody the transitional contours required to allow proper contour of the restorations and be designed with principles of retention derived from conventional fixed prosthodontics. The cement margin should not be placed more than 1 mm sub mucosal to facilitate cement removal. When cement retention is desired there must be sufficient inter occlusal space.
5. Overall treatment plan
Decisions to use implants should be based on prosthetically oriented risk assessment. When replacing long span fixed partial dentures consideration should be given to decreasing the number of pontics and increasing the number of implant abutments. Use of implants allows the clinician to segment the restoration. The prosthesis design in Figure 48 allowed avoidance of a long span fixed partial denture with a pier abutment. The additional cost of the two implants was justified by the reduction in prosthodontic risk. Prosthetically oriented risk assessment involves comprehensive evaluation of potential abutment teeth. The clinician often has to make the decision to maintain a compromised tooth versus placing an implant. Unfortunately scientific guidelines do not exist for such a decision and often the decision is based on risk assessment and cost effectiveness of the procedures (Figs 49,50,51,52).

This design allowed a reduction in span of the fixed partial denture and reduced the prosthodontic risk associated with these teeth

Three unit fixed partial denture fabricated on a compromised abutment

This patient should have been treated by means of proactive extractions and implant placement instead of the three unit fixed partial denture

Prosthesis sectioned at premolar area and two implants placed to replace molar teeth

The implant supported restorations have a favourable long term prognosis
Summary
Implants have added options to successful prosthodontic rehabilitations formerly unavailable. Implants must be a consideration for every treatment plan. Implant retained restorations provide considerable advantages over removable partial dentures. Improved support, a more stable occlusion, preservation of bone and simplification of the prosthesis are a few reasons why implants are the treatment of choice for missing posterior teeth. Additionally, long term oral health is often improved because less invasive restorative procedures are required for the remaining dentition. The practitioner must carefully evaluate the parameters outlined to ensure predictability and longevity of restoration.
References
Carvalho W, Casado PL, Caula AL et al. Implants for single first molar replacement, important treatment concerns. Implant Dent 2004; 13; 328–333.
Scmitt A, Zarb GA . The longitudinal clinical effectiveness of osseointegrated dental implants for single tooth replacement. Int J Prosthodont 1993; 6: 187–202.
Ek feldt, A, Carlssson, Borgesson G . Clinical evaluation of single tooth restorations supported by osseointegrated implants: a retrospective study. Int J Oral Maxillofac Implants 1994; 9: 179–183.
Becker W, Becker BE . Replacement of maxillary and mandibular molars with single endosseous implant restorations: A retrospective study. J Prosthet 1995; 74: 51–55.
Henry PH, Laney WR, Jemy T et al. Osseointegrated implants for single tooth replacement: A prospective 5 year multicenter study. Int J Oral Maxillofac Implants 1996; 450–455.
Buser D, Von Arx T . Surgical procedures in partially edentulous patients with ITI implants. Clin Oral Implants Res 2000; 11 (suppl I): 83–100.
Chiapasco M, Abati S, Romeo E, Vogel G . Clinical outcomes of autogenous bone blocks or guided regeneration with a e PTFE membrane for reconstruction of narrow edentulous ridges. Clin Oral Implants Res 1999; 10: 278–288.
Chiapasco M, Romeo E, Vogel G . Vertical distraction osteogenesis of edentulous ridges for improvement of oral implant positioning. A clinical report of preliminary results. Int J Oral Maxillofac Implants 2001; 16: 43–51.
Wetherell J, Smales R . Partial denture failure, a long term clinical survey. J Dent 1980; 8: 333–340.
Hebel KS, Gajjar R . Achieving superior esthetic results, parameters for implant and abutment selection. Int J Dent Symp 1997; 4: 42–47.
Woelfel JB . Dental anatomy: Its relevance to dentistry (4th edn). Philadelphia: Lea and Febiger, 1990.
Misch CE . Dental implant prosthetics. pp 281–307. Mosby, 2005.
Bischof M, Nedir R, Smukler-Moncler S, Bernard JP . A five year life table analysis of ITI implants. Results from a private practice with emphasis on the use of short implants. Clin Oral Implants Res 2001; 12: 396.
Ten Bruggenkate CM, Asikainen P, Foitzik C et al. Short (6 mm) non submerged dental implants: results of a multicenter clinical trial of 1-7 years. Int J Oral Maxillofac Implants 1998; 13: 791–798.
Graves SL, Jansen CE, Siddiqui AA et al. Wide diameter implants, indications, considerations and preliminary results over a two year period. Aust Prosthodont J 1994; 8: 31–37.
Balshi TJ . First molar replacement with an osseointegrated implant. Quint Int 1990; 21: 61–65.
Rangert B, Krough PHJ, Langer B, Van R Roekel N . Bending overload and implant fracture. A retrospective clinical analysis. Int J Oral Maxillofac Implants 1995; 10: 326–334.
Bahat O . Osseointegrated implants in the maxillary tuberosity: report on 45 consecutive patients. Int J Oral Maxillofac Implants 1992; 7: 459–467.
Carr AB, Laney WR . Maximum occlusal force levels in patients with osseointegrated oral implant prosthesis and patients with complete dentures. Int J Oral Maxillofac Implants 1987; 2: 101–108.
Sekine M . Problems of occlusion from the standpoint of prosthetic dentistry, with reference to the significance of balanced occlusion in the denture and biological considerations on the abutment teeth in relation to occlusion pressure in the partial denture. Shikwa Gakuho 1967; 67: 859–867.
Schulte W . Implants and the periodontium. Int Dent J 1995; 45: 16–26.
Mericske-Stern R, Geering AH, Burgin WB, Graf H . Three-dimensional force measurements on mandibular implants supporting overdentures. Int J Oral Maxillofac Implants 1992; 7: 185–194.
Cibirka RM, Razoog ME et al. Determining the force absorption quotient for restorative materials used in implant occlusal surfaces. J Prosthet Dent 1992; 67: 361–364.
Celletti R, Pameijer CH, Bracchetti G et al. Histologic evaluation of osseointegrated implants restored in non axial functional occlusion with pre-angled abutments. Int J Period Rest Dent 1995; 15: 562–573.
McGlumphy EA, Mendel DA, Holloway JA . Implant screw mechanics. DCNA 1998; 42: 71–89.
Agar J, Cameron SM, Hughbanks JC, Parker MH . Cement removal from restorations luted to titanium abutment with simulated subgingival margins. J Prosthet Dent 1997; 78: 43–47.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Jivraj, S., Chee, W. Treatment planning of implants in posterior quadrants. Br Dent J 201, 13–23 (2006). https://doi.org/10.1038/sj.bdj.4813766
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4813766
This article is cited by
-
Comparison of temperature changes in different irrigation methods used in guided piezosurgery: in vitro study
Oral and Maxillofacial Surgery (2023)
