
Key Points
-
Compared with previously reported prevalence rates of legionella spp. in dental hospitals in Europe and North America the prevalence of legionellae in dental unit water samples taken from general dental practices in London and rural Northern Ireland was very low.
-
A correspondingly low level of legionella antibody was detected in the recruited dentists, which were comparable to background levels in blood donors.
-
It cannot be assumed that all GDP dental unit waterlines will be free of legionellae as environmental conditions may prevail in an individual surgery that promotes the growth of legionellae.
-
In order to provide safe DUWL water that complies with drinking water quality standard, dentists are advised to follow Health and Safety Commission and BDA infection control guidelines for water management.
Abstract
Objectives To determine the prevalence of legionellae in dental unit waterlines (DUWL) in general dental practices in London and rural Northern Ireland and whether the organism occurs at a high enough frequency and magnitude in DUWL to represent a threat to dentists' health.
Materials and method Two hundred and sixty six (166 London, 100 Northern Ireland) randomly selected dental surgeries were recruited. Standardised 250 ml water samples were taken from the DUWL and 1 litre samples from the surgery cold water tap to measure the prevalence of legionellae. The dentists provided a blood sample for legionella serology.
Results The prevalence of legionellae was very low (0.37%). Legionellae were not isolated from DUWL or surgery basin taps in Northern Ireland. Legionella spp were isolated from the DUWL and surgery basin of one practice in London and from the cold water supply of a further three practices. The prevalence of Legionella pneumophila antibodies was less than that seen in a comparable group of London blood donors.
Conclusion The risk to dentists' health from potential exposure to legionellae in this cohort of dentists was very low and this was confirmed by the very low seroprevalence and antibody titres to legionella detected in the dentists.
Similar content being viewed by others


Main
Legionellae are commonly found in environmental water sources such as rivers, lakes and reservoirs where they generally occur in low numbers and may eventually colonise water cooling plants and hot and cold plumbing systems fed by municipal water supplies. Typically legionellae enters the dental unit waterlines (DUWL) from the mains drinking water where they are able to proliferate in the biofilm.1 Biofilm formation occurs on the inner surface of the waterlines as a result of water stagnation in microbore tubing and intermittent patterns of water use, combined with poor waterline management, which culminates in the generation of contaminated aerosols.2,3 In order to multiply, legionellae need other microorganisms and a supply of nutrients and temperatures in the range of 20–45°C;4 they will not proliferate in sterile water. Sludge at the base of water storage tanks and the micro-habitat within the DUWL biofilm provide favourable conditions for the colonisation and growth of legionellae within plumbing systems.5 The organism is protected from the bactericidal action of biocides by growth intracellularly in amoeba and/or within the biofilm matrix,6 and under suitable growth and temperature conditions legionellae can be amplified in the DUWL biofilm to potentially reach high concentrations (>103 per litre). Infection is by aerosol droplet inhalation or rarely, aspiration of contaminated water by susceptible individuals.8 Aerosol droplets generated by dental handpieces are of sufficient size and stability to enter the alveolae of the lungs. The Legionellaceae comprises more than 45 species but Legionella pneumophila is isolated from ≥90% of culture proven clinical cases with L. pneumophila serogroup 1 being the most common cause of Legionnaires' disease.8 Approximately 250 cases per year of Legionnaires' disease occur in the UK but this is considered to be an underestimate of the true number.9 Legionellosis can present either as an atypical pneumonia or as a milder flu-like illness, known as Pontiac fever.9 Many clinical cases occur sporadically and are not linked to a definite source but outbreaks of infection have been associated with cooling water systems, water fountains, spa pools and hot and cold water systems in public buildings.9 Fortunately, the attack rate is low at 2-5% for infections resulting in Legionnaires' disease although approximately 12% of cases are likely to be fatal. Even higher death rates are reported in nosocomial cases and in susceptible immunocompromised individuals.9 Risk factors known to be associated with contracting Legionnaires' disease include male sex, age greater than 50 years, smokers, alcoholics, diabetics and people with chronic respiratory or renal disease and cancer.10
It has been suggested that legionellae within DUWL may contribute to respiratory illness amongst the dental team.11,12 The reported prevalence of legionellae in DUWL varies widely from 0–68% depending, in part, on the isolation procedures.13,14,15 Variations in recovery rates are seen with different geographic locations, presence of large cold-water tanks and complex plumbing systems,7 thermal conditions and the type of dental equipment.16 Much of the data on legionellae in DUWL has derived from hospital-based studies where the plumbing and environmental conditions may not replicate those found in general practice. Extrapolation of these data to general practice is likely to be unsatisfactory and may be potentially misleading.13,15 Information on the colonisation of DUWL systems in general dental practice, and the health risk to the dental team who are subject to prolonged daily exposure to DUWL contaminated with legionellae, is limited.
The aim of this study was to try and answer these questions by firstly determining the prevalence of Legionella spp. in DUWL in general dental practices located in rural and metropolitan areas. Secondly, to evaluate whether legionellae are found at a high enough frequency and magnitude in DUWL to represent a threat to the health of the dental team, by determining whether dentists in the UK exhibited serological evidence of increased exposure to L. pneumophila above that expected in the background population.
Materials and Methods
Sample Group
Ethics committee approval was obtained from the Multicentre Ethics Committee. A total of 266 principal dentists (270 dental practices) were recruited into the study; 100 practices from rural Northern Ireland and 170 from the Greater London postal area. Rural practices were supplied by rural water sources including bore wells, loch and upland water sources managed by one of the four water boards which serve the province. In London all the dentists received supplies from Thames Water Utilities to their premises. Names of principal dentists located in the areas supplied by the five water boards were obtained from local health authority lists of NHS registered dentists. They were randomly selected using computer generated random numbers.
Dentists were initially contacted by letter and then telephoned. The research nurse visited dentists wishing to enrol in the study and written consent was obtained. The dentists completed a self-administered respiratory health questionnaire with questions pertaining to their general health, risk factors for infection with respiratory pathogens and evidence of current and past serious respiratory illness. Known lifestyle risk factors that could potentially confound the prevalence rates of L. pneumophila antibody titres were recorded. A blood sample (10 ml) was collected for legionella serology.
Ambient room, waterline and surgery tap water temperatures were recorded with a digital thermometer. The dentist was supplied with water sample bottles containing sufficient sodium thiosulphate to neutralise any remaining residual chlorine in the water sample and trained by the nurse in the method of water collection. Water sample collection was standardized to a single period of overnight water stagnation. On the designated water collection day, before the equipment was used at the start of morning surgery, the dentists collected the first 250 ml of water flushed through the dental unit from the air/water syringe and airturbine hand piece. One litre of water was sampled from the surgery basin cold-water tap. The latter sample acted as a microbiological control of the incoming mains water into the surgery. Water samples were stored in the dark, in a fridge prior to collection by the nurse and transported in a cool box to the laboratory. Collection of water samples by the dentist and transport to the receiving laboratory took less than six hours.
Legionellae isolation and identification
Processing of water samples for legionellae counts was undertaken in United Kingdom Accreditation Service accredited laboratories, according to a standard operating procedure based on methods specified in the British Standard Institute, 1992.17 100 ml of the water sampled from DUWL and 450 ml of water obtained from the surgery basin tap were filtered through a 0.2 μm polyamide membrane filter. The sample concentrate was suspended in 10 ml of Page's saline and centrifuged at 3,000 g for 30 minutes. The supernatant was removed aseptically to leave 1 ml of fluid in which the deposit was resuspended and 0.1 ml of the suspension was inoculated onto GVPC (Glycine, Vancomycin, Polymixin, Cycloheximide agar, Oxoid®) selective agar and incubated at 36°C for 2–14 days. Legionellae only grow in the presence of cysteine so presumptive legionellae colonies were confirmed by subculturing onto buffered charcoal yeast extract agar with and without L-cysteine. A legionella latex agglutination kit Oxoid® was used to confirm and further identify the legionellae. Positive cultures were then sent to the Respiratory and Systemic Infection Laboratory for definitive identification. Identification was undertaken by immunofluorescent antibody staining using L. pneumophila species-specific monoclonal antibody (MONFLUOR, Bio-Rad Ltd), and further subtyping with L. pneumophila serogroup 1 specific monoclonal antibody. All L. pneumophila non-serogroup 1 isolates were characterised using a hyperimmune rabbit antisera against all recognised serogroups and species of legionella.18
Legionella serology
The prevalence and concentration of L. pneumophila antibodies in the dentists' blood was used as evidence of previous or recent exposure to legionellae and thus acted as a surrogate marker of the dentists' risk from respiratory disease caused by Legionella spp. Detectable antibody against any individual antigen at a dilution of 1:16 is considered positive: no detectable antibodies at this dilution is considered a negative result. Positive sera were further titrated to determine the endpoint and a titre to ≥128 is interpreted as being suggestive of infection at an undetermined time. Using an indirect immunofluorescent test (IFAT) with monovalent antigens,19 the presence or absence in dentists' blood of antibodies against L. pneumophila serotypes 1-6 and 8, was quantified. These results were compared with the antibody titres derived using the same antigens from a cohort of 500 London blood donors.
Statistical analysis
The Chi square test was employed to demonstrate whether there was a statistically significant association between the presence of legionellae in the DUWL and the corresponding species-specific antibody titres. The data were analysed using the statistical package SPSS.
Results
The response rate for recruitment was 64.4%. A separate questionnaire was used to evaluate dentists not wishing to enrol in the study. Dentists from London were less likely to consent to take part in the study than their Northern Ireland counterparts (OR 0.43, 95%CI 0.25 to 0.72, p=0.001). Non-recruited dentists had been qualified for longer (recruited dentists: mean time 18.44 yrs (sd 9.37) versus non-recruited dentists: mean time 20.61 yrs (sd 8.77); p=0.04). There was no significant difference for any of the other variables (smoking, chronic respiratory disease, number of surgeries, whether water was taken directly from the mains, held in a tank or an independent bottled water system installed) between enrolled and non-enrolled dentists.
Practice visits took place throughout the year, 9.2% of water samples were collected in the spring, 15.8% in the summer, 36.9% in the autumn and 38.1% during the winter months. All enrolled dentists used municipal water supplies in their surgeries, 80.4% used mains drinking water to supply the dental waterlines, but in 10% of cases, the water was not taken directly from the mains but was held in a storage tank. An independent water reservoir system had been fitted to the airturbine waterline by 27.85% of dentists but the reservoirs were filled with mains tap water in 35.7% of cases. Only 17.2% of the practices filled the reservoir with sterile water and the remainder of dentists used non-sterile distilled water to fill the reservoir. The median number of hours when the dental unit was not in use and the water in the DUWL was stagnant was 131 hours per week. The mean ambient air temperature of the surgeries was 21.6°C (range 16.2-27.2°C), mean airturbine water temperature was 20.6°C (range 12.7- 32.3°C) and the mean temperature of water from the surgery basin was 18.1°C (range 6.4-31.1 °C).
Legionella isolation from dental waterlines
Legionellae were not isolated from DUWL or surgery basin taps in Northern Ireland. In one practice in London L. pneumophila serogroup 14 was isolated from the surgery basin tap (8 × 102 colony forming units (cfu) L−1) and the DUWL (10.8 × 10 4cfu L−1).
Initial samples from the cold water surgery basin tap from three other practices in London were positive for legionellae. In none of these three practices were legionellae isolated from the DUWL. L. pneumophila serogroup 1, was only recovered from the surgery basin tap water in one dental practice and only in low numbers (5.2 × 102 cfu L−1). However on further water sampling the organisms were isolated from the hot water plumbing. All three practices had sinks fitted with mixer taps and crossover between the hot and cold supply may have occurred within the mixer tap.
Dentists' legionella serology
Blood samples were obtained from 246 of the 266 dentists recruited into the study. The dentists recruited into the study were either the principal or senior partner in the practice and had been qualified for a mean of 18.4 years and had spent a mean of 10.8 years working in the inspected dental surgery. The male:female ratio was 84.2%:15.8% and the mean age was 42.3 years. London blood donors were used for comparison. They had been selected by age and sex with an excess of males. The age range of the 500 blood donors was 30 – 59 years and 166 of the donors were aged between 40 and 49 years. Although the blood donors were not matched to the dentists the overall demographic parameters were comparable.
Smokers accounted for 12.5% of the dentists and ex-smokers 22.6%. Two (0.75%) of the dentists suffered from diabetes mellitus and one from renal disease. No dentists reported experiencing Legionnaires' disease or Pontiac fever although one dentist was diagnosed with pneumonia (cause unknown) in the last year and 14% reported asthma and 7.6% bronchitis and one dentist (0.37%) suffered from Sarcoidosis.
The results of the L. pneumophila serology can be seen in Table 1. Only one dentist had a positive antibody titre 1:16 to L. pneumophila serogroup 1 One dentist had a titre of 1:128 to L. pneumophila serogroup 3 but this was not associated with any clinical symptoms. A blood sample was obtained from three out of the four dentists where the surgery plumbing was positive for Legionella species: the fourth dentist refused permission. All three dentists had negative serology.
The prevalence of L. pneumophila antibodies in this study's population of dentists did not exceed the background levels seen in London blood donor control group. In fact the titres were significantly lower for the dentists compared with the blood donors for the following serogroups L. pneumophila serogroup 2 (p=0.0002), L. pneumophila serogroup 3 (p=0.005), L. pneumophila serogroup 6 (p=0.012) and L. pneumophila serogroup 8 (p=0.035).
Discussion
The prevalence of legionellae in DUWL in the Greater London postal area was very low (1/166 practices, 0.6%). Legionellae were not isolated from DUWL or surgery basin taps in Northern Ireland. Legionellae were isolated from the DUWL and surgery basin of one practice in London. The circumstances in this case were unusual. The practice was situated in a large building with a communal cold-water tank supplying the entire building. Although the dentist had installed an independent water reservoir system, the dentist used tap water from the surgery basin to fill the reservoir. The surgery basin tap water was subsequently found to be contaminated with L. pneumophila serogroup 14.
This study was designed as a cross sectional prevalence survey rather than a longitudinal design. It could be argued that this might account for the low prevalence rate recorded in the study as Challacombe et al.16 found only 23 of 49 contaminated units to be positive on more than one occasion over a 44 month period. Whereas, Pankhurst et al.7 repeatedly sampled a dental unit waterline colonised with L. bozemanii on nine occasions over a period of 15 weeks and the water samples were consistently positive. Results obtained from a 13-year retrospective survey of a hospital water system concluded that specific strains of L. pneumophila can persistently colonize a hospital water supply and cause recurrent clusters of nosocomial infection.20 The persistence of legionellae in plumbing systems would support the appropriateness of the cross-sectional design.
We had expected to find a much higher prevalence of L. pneumophila as previous studies had reported frequencies of 8% in the USA,13 21.8% in Italy,15 and 25% in London.16 Atlas et al.13 employed a polymerase chain reaction (PCR) to identify all species of legionellae in DUWL and reported a prevalence of 68% in waters sampled from hospital and dental practices. However, a recent cross sectional survey by Walker et al.14 looking exclusively at general dental practices (in the South West of England) found only 1 of the 55 surgeries examined was culture positive for L. pneumophila; a similar prevalence rate to that obtained in this study. In general, higher recovery rates of legionellae have been associated with water samples taken from dental hospitals and other large institutions. Storage of water in large tanks acts as a reservoir for repeated seeding of the plumbing system and complex plumbing systems found in large institutions are more prone to colonisation with legionellae.7 Whereas the vast majority of dentists in this survey took their surgery water supply directly from the mains water and only 10% used an intermediary cold-water storage tank, which may in part explain the low numbers of legionellae positive samples.
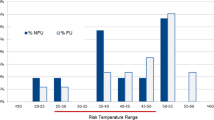
Thermal control is recommenced as an infection control measure in hot and cold plumbing systems.9 Water temperatures in the range 20–45°C favour the growth of legionellae, temperatures below 20°C inhibit proliferation and the organism cannot survive for more than a few seconds above 60°C. Temperatures between 20–25°C are associated with lower concentrations of bacteria and reduced virulence of the organism.21 The recorded temperature of water sampled from the handpieces in the present study was in the range 12.7– 32°C with a mean of 20.8°C. However, Zanetti et al.15 who found that 16.7% of the samples taken from ten private dental surgeries contained L. pneumophila, reported similar water temperature means and ranges.
The majority (73%) of the water samples were collected in London and Northern Ireland in the cooler autumn and winter months. Although the ambient air temperature range is fairly steady in the dental surgery thought the year, the temperature of the municipal water held in reservoirs, lochs or taken from rivers will vary markedly throughout the year with lower temperatures expected in the winter months. Temperature differences may explain some of the geographic variations seen in previously published results in Europe and North America. Other environmental factors such as a higher organic content in surface compared with ground waters22 and water hardness15 are also know to favour the prevalence of legionellae.
In this defined cohort of dentists, the results from a single blood specimen indicate that serological evidence for exposure to L. pneumophila is minimal and there is no evidence of an excess of positives above background levels resulting from occupational exposure whilst practicing dentistry. The low seroprevalence levels of L. pneumophila antibodies in this study parallel the low isolation rate of the bacterium from the dental surgery samples. In a previous study a high prevalence of legionellae seropositivity was recorded in 34% in the dental team compared with 5% of the control non-medical population.11 Eleven per cent of the dentists and dental nurses had strong antibody titres of >1:128 suggestive of possible recent infection. Positive results were associated with working in the dental surgery for more than 1.5 years.11 Similar results were found in dental personnel working in a dental hospital in the USA.12 No cases of Legionnaires' disease or Pontiac fever were reported amongst the study volunteers but unfortunately the DUWL were not tested for the presence of Legionellae. Presumably one would have expected to see heavy contamination of the system. The authors concluded that the data represented a requirement for repeated exposure to the antigen before serconversion occurred11 suggesting that low concentrations of legionellae in the DUWL may be insufficient to precipitate frank infection but may 'immunise' the dentist.
These results were not confirmed in publications from two of the London dental schools who reported legionellae in the DUWL but found no correlation with respiratory illness or legionella serconversion in their staff.7,23 A single fatal case of legionella pneumonia in a dentist caused by L. dumoffi has been reported. L. dumoffi and other Legionella spp were recovered from his surgery waterlines after his death, but only in low numbers from his domestic water supply.13 There are no other substantiated cases of occupational Legionnaires' disease linked to dentistry. UK epidemiological surveillance data from notified cases of Legionnaire's disease revealed a small number of dentists who had contracted Legionnaires' disease but investigation of their DUWL were not performed. The dentists had other recognised risk factors for legionellosis and no causal occupational association was made by the authors of the report.24
The very low seroprevalence of raised antibody titres to L. pneumophila detected in the dentists establishes that the risk to the dentists' health in general dental practice in London and Northern Ireland from potential occupational exposure to legionellae was minimal. If there was a risk from long-term exposure to legionellae then it would be expected to be seen first in the dental team as they have the highest and most prolonged risk of exposure. However, the lack of any evidence of long-term exposure in the dentists, strongly suggests that patients would also be at minimal risk of serious respiratory illness.
Nevertheless there is no room for complacency25 and dentists are required to comply with the Health and Safety at Work Act 1974 and the Control of Substances Hazardous to Health Regulations 1999 and implement the water management guidance described in the Heath and Safety Commission's Approved Code of Practice: The control of legionella bacteria in water systems which came in to force in 2001.9
References
Pankhurst CL, Johnson NW, Woods RG . Microbial contamination of dental unit waterlines: the scientific argument. Int Dent J 1998; 48: 359– 368.
Shearer BG . Biofilm and the dental office. J Am Dent Assoc 1996; 127: 181– 189.
Mills SE . The dental unit waterline controversy: defusing the myths, defining the solutions. J Am Dent Assoc 2000; 131: 1427– 1441.
Wadowsky RM, Wolford R, McNamara AM, Yee RB . Effect of temperature, pH and oxygen level on the multiplication of naturally occurring Legionella pneumophila in potable water. Appl Environ Microbiol 1985; 48: 1197– 1205.
Ciesielski CA, Blaser MJ, Wang WL . Role of stagnation and obstruction of water flow in isolation of Legionella pneumophila from hospital plumbing. Appl Environ Microbiol 1985; 48: 984– 987.
King CH, Shotts EB, Wooley RE, Porter KG . Survival of coliforms and bacterial patho-gens within protozoa during chlorination. Appl Environ Microbiol 1988; 54: 3023– 3033.
Pankhurst CL, Phillpott-Howard JN, Hewitt JH, Casewell MW . The efficacy of chlorination and filtration in the control and eradication of Legionella from dental chair water systems. J Hosp Infect 1990; 16: 9– 18.
Joseph CA . Surveillance of Legionnaires' disease in Europe. In Marre R. (Ed) Legionella. Washington: ASM, 2002 pp 311– 317.
Health and Safety Commission (2000). Legionnaires' disease. The control of legionella bacteria in water systems. Approved Code of Practice and Guidance. Third Edition. London: HMSO.
Marston BJ, Lipman H, Brelman RF . Surveillance for Legionnaires' disease: risk factors for morbidity and mortality. Arch Intern Med 1994; 154: 2417– 2422.
Reinthaler FF, Mascher F, Stunzer D . Serological examination for antibodies against Legionella species in dental personnel. J Dent Res 1988; 67: 942– 942.
Fotos PG, Westfall HN, Synder IS, Miller RW, Mutchler BM . Prevalence of Legionella-specific IgG and IgM antibody in a dental clinic population. J Dent Res 1985; 64: 1382– 1385.
Atlas RM, Williams JF, Huntingdon MK . Legionella contamination of dental-unit water. Appl Environ Microbiol 1995; 61: 1208– 1213.
Walker JT, Bradshaw DJ, Bennett AM, Fulford MR, Martin MV, Marsh PD . Microbial biofilm formation and contamination of dental-unit water systems in general practice. Appl Environ Microbiol 2000; 66: 3363– 3367.
Zanetti F, Stampi S, De LucaG, Fatch-Moghdam P, Antonietta M, Sabattini B, Checchi L . Water characteristics associated with the occurrence of Legionella pneumophila in dental units. Europ J Oral Sci 2000; 108: 22– 28.
Challacombe SJ, Fernandes LL . Detecting Legionella pneumophila in water systems: a comparison of various dental units. J Am Dent Assoc 1995; 126: 603– 608.
Detection and enumeration of Legionella organisms in water and related materials. British Standard Institute DD211, 1992.
Harrison TG, Taylor AG . Identification of legionellae by serological methods. In Harrison T G, Taylor A G (Eds). A laboratory manual for legionella. Chichester: J. Wiley & Sons 1988, pp 57– 68.
Harrison TG, Taylor AG . Demonstration of legionellae in clinical specimens. In Harrison T G, Taylor A G (Eds). A laboratory manual for legionella. Chichester: J. Wiley & Sons 1988, pp 103– 112.
Rangel-Frausto MS, Rhomberg P, Hollis RJ, Pfaller MA, Wenzel RP, Helms CM, Herwaldt LA . Persistence of Legionella pneumophila in a hospital water system: a 13-year survey. Infect Cont Hosp Epidemiol 1999; 20: 793– 797.
Mauchline WS, James BW, Fitzgeorge RB, Dennis PJ, Keevil CW . Growth temperature reversibly modulates the virulence of Legionella pneumophila. Infect Immunol 1994; 62: 2995– 2997.
Zacheous OM, Martikainen PJ . Occurrence of Legionella in hot water distribution systems of Finnish apartment buildings. Can J Microbiol 1994; 40: 993– 999.
Oppenheim BA, Sefton AM, Gill ON, Tyler JE, O'Mahony MC, Richards PJL, Harrison TG . Widespread Legionella pneumophila contamination of dental stations in a dental school without apparent human infection. Epidemiol Infect 1987; 99: 159– 166.
Bartlett CL, Bibby LF . Epidemic Legionellosis in England and Wales. Zentrablatt Bak Mikrobiol Hyg 1983; 255: 64– 70.
Pankhurst CL . British Dental Association Fact File - Contaminated dental unit waterlines. July 2000. www.bda.org.
Acknowledgements
This work was supported by a grant from the NHS National Primary Dental Care Research and Development Programme RDO/90/08 The assistance of Mrs Mary McCartney research nurse is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Pankhurst, C., Coulter, W., Philpott-Howard, J. et al. Prevalence of legionella waterline contamination and Legionella pneumophila antibodies in general dental practitioners in London and rural Northern Ireland. Br Dent J 195, 591–594 (2003). https://doi.org/10.1038/sj.bdj.4810735
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4810735
This article is cited by
-
Review Global seroprevalence of legionellosis - a systematic review and meta-analysis
Scientific Reports (2020)
-
The risk does exist
British Dental Journal (2010)
-
An audit improves the quality of water within the dental unit water lines of general dental practices across the East of England
British Dental Journal (2010)
-
Comparison of the microbial load of incoming and distal outlet waters from dental unit water systems in Istanbul
Environmental Monitoring and Assessment (2009)
-
Microbial contamination of dental unit waterlines in Istanbul, Turkey
Environmental Monitoring and Assessment (2008)
