
Key Points
-
Methyl methacrylate monomer is a widely used chemical.
-
Its use has been associated with localised sensory nerve abnormalities in the hands of dental technicians.
-
This case study shows that MMA can induce generalised neuropathy.
-
Practitioners should be aware in order that appropriate precautions should be taken.
Abstract
A 36-year-old dental technician for 14 years developed paraesthesia and numbness in her legs. Neurophysiological studies revealed absent sensory nerve action potentials (SNAPs) from her lower limbs and normal upper limb SNAPs on presentation. Motor nerve studies were normal. Repeat studies 2 months after leaving her job showed some improvement in the lower limb SNAPs. It is suggested that her symptoms were caused by occupational exposure to methyl methacrylate monomer.
Similar content being viewed by others


Main
Occupational exposure to methyl methacrylate (MMA) monomer a widely used chemical has been associated with contact dermatitis,1,2,3 asthma,4 drowsiness, head-ache, anorexia and decrease in gastric motor activity.5 Localised distal sensory neuropathies have been reported limited to the hands of dental technicians,6 and orthopaedic surgeons1 handling MMA. In addition, a generalised motor and sensory axonal neuropathy has been reported in a dental prosthetic technician following 40 years of exposure to MMA.7 However, the neurotoxic effects of MMA have not been fully evaluated and have been considered permanent. We report a predominantly sensory polyneuropathy in a dental technician following exposure to MMA, with resolution of neuropathic features when exposure to MMA was avoided.
Case study
A 36-year-old right-handed dental technician for 14 years presented with 11-month history of paraesthesia and numbness with a stocking distribution bilaterally. This caused her to stumble occasionally and she also experienced difficulty while walking on carpets. There was no muscle weakness or wasting, neither were there any symptoms in the upper limbs. She has worked in the present dental laboratory for 3 years where she used autopolymerisation and selfcuring formulations containing MMA monomer for various procedures, applying manipulatory methods similar to that described by Donaghy et al.7 The room where she worked had only one window which was kept closed most of the time. Fan extractors or fume cupboards were not used, and the pungent odour of MMA monomer permeated the atmosphere.
Her medical history included sickle cell trait, mild asthma and a healed pelvic fracture following a road traffic accident that had occurred 4 years earlier. There was no history of alcoholism. Her brother, who worked as a dental technician in a different laboratory for 12 years had complained of similar sensory symptoms but had not related them to exposure to MMA. Interestingly, the sensory symptoms in her brother recovered gradually within 2 years of changing his profession. Her father was diabetic.
Neurological examination showed no abnormalities in cranial nerves and upper limbs. In the lower limbs there was no muscle weakness or wasting. The knee jerks were present, and ankle jerks were absent bilaterally. Both planter responses were flexor. Sensation to pin-prick, light touch and temperature was reduced bilaterally in a stocking distribution. Vibration sense was diminished in both feet and lower limbs to the level of the knees. Joint position sense was intact. Sacral and peri-anal sensation was preserved. There was no postural drop in blood pressure. She was examined again 2 months after leaving the profession, when neurological signs remained unchanged except for detection of the right ankle jerk. She was still complaining of numbness in both legs.
The following investigations were within normal range: full blood film haematological parameters, ESR, blood glucose, urea and electrolytes, liver and thyroid function tests, serum B12, folate levels and urinalysis. Serology for syphilis and autoantibody profile were negative. She was not on any neurotoxic drugs.
Neurophysiology
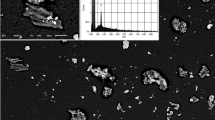
Nerve conduction, using surface electrodes and concentric needle electromyography (EMG) studies performed 11 months after presentation and repeated 6 months later, 2 months after she left her dental employment, revealed no motor or sensory nerve abnormalities in the hands and normal motor values from the lower limbs in both studies. However, no sensory nerve action potentials (SNAPs) were obtained from the legs in the first study, while in the second study small sural SNAPs were obtained from the right (amplitude 3.0 μV conduction velocity 36.1 m/s), and the left (3.0 μV, 34.6 m/s (fig. 1)) legs (Normal ≥ 5.0 μV, 40.0 m/s). Other SNAPs from the legs remained unrecordable.

Top: Absent left sural SNAP on presentation, Bottom: Some recovery in left sural SNAP 2 months after avoidance of MMA exposure.
External temperature of finger and sole of feet was maintained at between 35 to 35.5°C in both studies.
Discussion
The use of methyl methacrylate (MMA) is universal in dentistry where it is widely used as an acrylic plastic in denture preparation, in the construction of special trays for impression taking, denture repair relining and rebasing, in removable orthodontic appliances, and for adding a post-dam to an adjusted upper denture.8 MMA is also increasingly used in orthopaedics for fracture treatment and reconstructive orthopaedic procedures,9 in ophthalmology for contact lenses, keratoprosthesis and intraocular lenses10 and applied in ophthalmic surgery for correction of enophthalmos, filling orbital or periorbital bone defects, making socket impressions, as comformers in the management of socket contraction and formation of exenteration implants.5
Donaghy et al. in 1991 reported a 55-year-old dental technician with several years history of motor and sensory symptoms.7 The symptoms had started from the dominant thumb and index finger and gradually spread proximally. Histological examination of a sural nerve biopsy specimen showed a moderately severe, chronic axonopathy with loss of large diameter fibres and unmyelinated axons.7 Other previous reports of neurotoxicity due to MMA were limited to the dominant hand and were mainly a distal sensory neuropathy.1,6 Also animal experiment on rat tail has shown that MMA has a neurotoxic effect when locally applied.11
In the present report, the presence of numbness and parasthesia, absent ankle jerk reflexes and unobtainable SNAPs from the legs were consistent with a predominantly sensory peripheral polyneuropathy affecting the lower limbs. Improvement of neurophysiological abnormalities following avoidance of MMA exposure suggests that this substance is the cause of the neuropathic abnormalities. Motor involvement was not noted on clinical or neurophysiological grounds. Normal sensory conduction values from the ulnar, median and radial nerves bilaterally with absent lower limb SNAPs suggest that neurotoxicity was caused by inhalational rather than cutaenous exposure.
Interestingly, the patient's brother who was also a dental technician for 12 years before leaving dental employment also had similar sensory symptoms in the legs but he never related this to his job. The brother's symptoms gradually improved after leaving the profession for personal reasons with only residual numbness in the big toes, 2 years after he stopped work as a dental technician. The occurrence of MMA-related symptoms in the siblings presented here raises the possibility of a genetic susceptibility, and further studies are indicated to verify this.
Conclusion
The present case and available literature suggest that methyl methacrylate causes both localised and generalised motor and sensory neuropathy. While the wearing of gloves may reduce the risk of localised neurotoxicity, MMA is known to be permeable to gloves12, and the wearing of gloves is considered to affect the feel of manipulation.7 The use of face gas mask, fume-cupboards and extractor fans may help to minimise the risk of neuropathy caused by inhalation.
References
Fisher A A . Paresthesia of the fingers accompanying dermatitis due to methylmethacrylate bone cement. Contact Dermatitis 1978; 5: 56–57.
Fries I B, Fisher A A, Salvati E A . Contact dermatitis in surgeons from methylmethacrylate bone cement. J Bone Joint Surg 1975; 57-A: 547–549.
Estlander T, Rajaniemi R, Jolanki R . Hand dermatitis in dental technicians. Contact dermatitis 1984; 10: 201–205.
Wittczak T, Palczynski C, Szulc B, Gorski P . Bronchial asthma with inflammation of the nose mucous membrane induced by occupational exposure to methyl methacrylate in a dental technician. Medycyna Pracy 1996; 47: 259–266.
Anderson R L, Stasior O G . Self curing methyl methacrylate: is it safe?. Ophthal surg 1976; 7: 28–30.
Seppalainen A M, Rajaniemi R . Local neurotoxicity of methyl methacrylate among dental technicians. Am J Industrial Med 1984; 5: 471–477.
Donaghy M, Rushworth G, Jacobs J M . Generalised peripheral neuropathy in a dental technician exposed to methyl methacrylate monomer. Neurology 1991; 41: 1112–1116.
Combe E C . Notes on dental materials. 6th ed. pp162. Edinburgh: Churchill Livingstone, 1992.
Merendino J, Serti G, Skondia V . Use of biocompatible orthopaedic polymer for fracture treatment and reconstructive orthopaedic procedures. J Int Med Res 1984; 12: 351–355.
Refojo M F . Current status of biomaterials in ophthalmology. Surv Ophtalmol 1982; 26: 257–265.
Verkkala E, Rajaniemi R, Savolainen H . Local neurotoxicity of methylmethacrylate monomer. Toxicol Lett 1983; 18: 111–114.
Waegemaekers T H, Seutter E, den Arend J A, Malten K E . Permeability of surgeons' gloves to methyl methacrylate. Acta Orthopaedica Scandinavica 1983; 54: 790–795.
Author information
Authors and Affiliations
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Sadoh, D., Sharief, M. & Howard, R. Occupational exposure to methyl methacrylate monomer induces generalised neuropathy in a dental technician. Br Dent J 186, 380–381 (1999). https://doi.org/10.1038/sj.bdj.4800117
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4800117
This article is cited by
-
Proportionate Cancer Mortality in Methyl Methacrylate-Exposed Orthopedic Surgeons Compared to General Surgeons
Journal of Medical Toxicology (2011)
-
Cell death effects of resin-based dental material compounds and mercurials in human gingival fibroblasts
Archives of Toxicology (2006)
