
Abstract
Objectives To ascertain the training received in management of medical emergencies recalled by general dental practitioners (GDPs), as undergraduates and since graduation, to examine how well prepared they felt to manage such events and how their readiness might be improved.
Design Postal questionnaire survey of a random sample of GDPs in Great Britain
Subjects 1500 GDPs, 1000 in England & Wales and 500 in Scotland
Results There was a 74% response. Among respondents, 75% had received training as undergraduates in the management of medical emergencies, 95% had subsequently received training. The proportion considering themselves 'well' or 'fairly well' prepared to manage emergencies rose from 30% at graduation to 80% currently. The 20% who felt themselves 'not very well' or 'not at all' prepared were less likely to possess the drugs and equipment to manage an emergency. Nevertheless, a need for further training was expressed by 96%: only 3% felt no need.
Conclusions Virtually all GDPs (99.2%), had received training in the management of medical emergencies at some time, principally since graduation. The 20% who feel inadequately prepared are less likely to possess the necessary drugs and equipment. There is a perceived need for further training among the majority of respondents.
Similar content being viewed by others


Main
Training in the management of medical emergencies is considered an essential component of the undergraduate dental curriculum, with a recommendation for annual training in first aid, including cardiopulmonary resuscitation (CPR).1 The GDC guidelines on the professional conduct of dentists state that all members of the dental team must be trained and prepared to deal with a medical emergency and that there be frequent practice of resuscitation routines. The latest guidelines go so far as to list equipment which must be available in a dental surgery to manage such an event.2
Few studies have assessed how competent dentists consider themselves in managing medical emergencies. A questionnaire survey in Australia found that two-thirds of respondents felt that they could carry out expired air resuscitation and that just over half believed themselves to be competent in CPR.3 A study of undergraduates at the University of Washington in the United States into their self-assessed confidence in various aspects of geriatric dentistry found that they consistently reported the area of 'management of medical emergencies' to be where most training was needed. These assessments had been undertaken before and after a course of lectures and after clinical experience of treating geriatric patients.4
Against this background of limited information, with doubts over perceived competence among dentists in the management of medical emergencies, the present study aimed to investigate:
-
The training received by a sample of GDPs as undergraduates and sought as postgraduates
-
How well prepared they considered themselves to manage emergency events
-
How their preparedness might be improved, if this was considered necessary.
This is the last of three reports on the findings of a questionnaire survey of GDPs in Great Britain. Details of the method, including a copy of the questionnaire, have been reported in Part 1 of this series.5
Results
Undergraduate and postgraduate training
The average length of time in practice of respondents was 15.8 years, with a range of 9 months to 42 years. Three-quarters of respondents (75.2%) indicated that they had received training in the management of medical emergencies as undergraduates and 22.1% that they had not. There was a statistically significant difference among respondents according to the length of time in practice. Only one in ten (10.4%) of those in practice less than the average of 15.8 years did not recall having received training as undergraduates compared with four out of ten (41.5%) who had been in practice for longer than 15.8 years (P < 0.001). The majority of respondents, 94.8%, reported that they had sought training in management of medical emergencies since graduation and only 3.8% indicated that they had not. There was no association with the length of time in practice. Overall, 99.2% reported training at some stage — either as undergraduates or since graduation.
The specific elements of training for medical emergencies from the undergraduate programme and from postgraduate training are listed in Table 1. For each, they were asked whether they had received training in CPR, gaining intravenous (IV) access, and in the use of emergency drugs. They were also invited to mention other aspects of training that they recalled. CPR was the most frequently recalled: by 93.9% who recalled undergraduate training and by 98.9% who had sought postgraduate training. This was followed by use of emergency drugs: by 61.7% during undergraduate training and 63.3% in postgraduate training. Other types of training sought following graduation included advanced life support and SAAD (Society for the Advancement of Anaesthesia in Dentistry) courses. There were two who were also medically qualified.
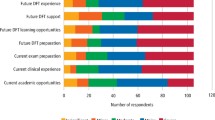
Figure 1 shows how well prepared respondents considered themselves to manage a medical emergency as a result of their undergraduate training. About two-thirds of respondents — 65% in England & Wales, 72% in Scotland (this difference was significant (P = 0.041)) — felt they were either 'not very well' or 'not at all' prepared: these were more likely to be recent graduates (P < 0.001). The 20% who reported no training as undergraduates were more likely to feel 'not very well' or 'not at all' prepared to manage a medical emergency upon graduation (P < 0.001).

How well prepared respondents felt they were to manage a medical emergency at graduation
Current perceptions of preparedness
Figure 2 shows how competent respondents currently felt about managing medical emergencies. Compared with perceptions at graduation, there has been a marked shift in self-rated capability from 29.9% who felt themselves 'very well' or 'fairly well' prepared at graduation to 78.7% at the time of the survey. Nonetheless, one in five (20.0%) currently felt 'not very well' or 'not at all' prepared to manage a medical emergency.

How well prepared respondents felt currently to manage a medical emergency
Analysis of differences between those who stated that they currently felt either 'very well' or 'fairly well' prepared to manage a medical emergency on the one hand, compared with those who felt either 'not very well' or 'not at all' prepared on the other was undertaken. Those who felt 'well' or 'fairly well' prepared were more likely to provide treatment under general anaesthesia (GA), intravenous sedation (IVS) and inhalation sedation (IS), more likely to possess every item of emergency equipment specifically enquired of in the questionnaire and to have received training at both undergraduate and postgraduate levels (all P < 0.05).
Expressed need for further training
Enquiry was made as to whether respondents considered that there was a need to improve their readiness to manage a medical emergency and, if so, whether this could be achieved by 'hands-on' courses and/or lectures. The vast majority, some 95.7%, expressed a need for some form of further training in this area, whereas only 2.7% felt no need. A total of 90.3% of all respondents expressed a desire for 'hands-on' courses, with 21.2% expressing a wish for lectures in addition to these courses, and just 1.6% wishing for only lectures.
Additional comments were invited and were made by 162 respondents (14.8%). Most stated that the respondent carried out regular in-practice emergency routines or that 'hands-on' courses were the best way to maintain preparedness. Some expressed doubts about correct diagnosis of an event, gaining IV access or the use of emergency drugs. The 2.7% who felt no need to improve their ability to manage medical emergencies were found to be more likely to feel either 'well prepared' or 'fairly well prepared' to manage a medical emergency (P = 0.035).
Discussion
The similarities between England & Wales and Scotland are prominent features but respondents in Scotland were found to be significantly more likely to feel 'not very well' or not at all' prepared to manage a medical emergency upon graduation.
About 20% of respondents did not recall training as undergraduates in managing medical emergencies, with a marked bias toward those who had been in practice for longer. Also, more than two-thirds of respondents felt inadequately prepared to deal with a medical emergency upon graduation. That recent graduates were more likely to have recalled training as undergraduates may reflect a changing emphasis in the curriculum in dental schools or it may simply be that older practitioners did not recall this aspect of their undergraduate training. The results relate to undergraduate programmes held over many years and do not directly imply the state of the present situation. There is a need to ensure that effective undergraduate training is available, particularly as those who recalled undergraduate training were more likely to feel better prepared in the longer term. Developments in vocational or general professional training may provide a useful opportunity to consolidate these skills. Adequate training in the use of drugs and equipment can also enhance confidence.
Respondents who provide GA, IVS and IS perceived a high state of readiness to deal with medical emergencies. It is clear that they felt they had benefited from those components of undergraduate and postgraduate courses that had offered them relevant skills. This may help explain why those who felt 'well' or 'fairly well' prepared to manage a medical emergency were significantly more likely to have all the emergency drugs or items of equipment specifically enquired of in the questionnaire. Perhaps they felt better prepared because they possessed these items. Conversely, it may be that those who felt 'not very' or 'not at all' well prepared are less likely to possess them because they feel unhappy about using them. Comments made by some respondents indicate that they bought the drugs and equipment recommended because this is required of them, whether or not they would actually use them in an emergency situation, for fear of litigation in the event of further complications arising from their use.
Over 95% — the vast majority — expressed the need for further training in the management of medical emergencies, mainly by means of 'hands-on' courses. Recent GDC guidelines emphasise the need for training of the whole dental team in the management of medical emergencies2 and the importance of maintaining these skills has also been highlighted.6,7 Schemes are now being instituted where dental practice staff are trained as a team in CPR skills in their dental surgery premises.8
The present survey found that 94% of respondents had sought training since graduation which involved CPR, compared with 64% in Australia, and 79% felt well or fairly well prepared to manage a medical emergency compared with 57% who felt that they were capable of doing CPR for 5 minutes. A potential result of the attention drawn to this subject by the 'Poswillo report' may be that more dentists in Britain have sought training and consequently feel better prepared than their Australian counterparts.
There is of course a great difference between actual and perceived competence and this is as true for managing medical emergencies as anything else. Four-fifths of respondents in this survey currently felt 'well' or 'fairly well' prepared, yet in Australia, only between one-third and two-thirds of respondents gave the correct answers to questions in a 'quiz' included in the questionnaire.9 None of a sample of 16 dental undergraduates and nine dental house officers in Bristol and only 40% of junior hospital doctors who undertook practical assessments of CPR skills achieved the required standard. The authors concluded that there was a need for improved levels of training in CPR in undergraduate training and regular revision to maintain these skills.7,10
Dentists might feel better prepared to manage such events if they felt that they had received adequate training in the use of the drugs and equipment they are required to possess. It is also important that what they are required to possess is realistic in terms not only of the training they have received but also considering the number of times these skills are likely to be used in a working lifetime. The importance of acquiring and maintaining skills in CPR in particular, as stipulated by the GDC guidelines,2 and in managing medical emergencies in general cannot be overemphasised.
Conclusions
This is the first survey in Great Britain on the issue of dentists' perceptions of their training and competence in the management of medical emergencies. There is an awareness of the importance of being prepared to manage medical emergencies which may occur in the dental surgery. The importance of effective undergraduate training in management of medical emergencies, bearing in mind the many demands of the undergraduate curriculum, must be emphasised, as this appears to be of long-term benefit to practising dentists. Those who feel 'well' or 'fairly well' prepared to manage a medical emergency are more likely to possess the emergency drugs and equipment necessary to do so. The majority of respondents indicated a need for further training by means of 'hands-on' courses. This is an ongoing issue. The findings of this study indicate the need to institute and repeat formal training for dental practices in the management of medical emergencies, as stipulated by the General Dental Council.
References
Smales F C, Anderson J, Basker R M, Harrison A, Kramer L D, Macadam T S, McGowan D A, Murray J J . The first five years: the undergraduate dental curriculum. London: General Dental Council, March 1997.
Maintaining standards — guidance to dentists on professional and personal conduct. London: General Dental Council, November 1997.
Chapman P J . Medical emergencies in dental practice and choice of emergency drugs and equipment: a survey of Australian dentists. Aust Dent J 1997; 42: 103–108.
Kiyak H A, Brudvik J . Dental students' self-assessed competence in geriatric dentistry. J Dent Educ 1992; 56: 728–734.
Atherton G J, McCaul J A, Williams S A . Medical emergencies in general dental practice in Great Britain. Part I: their prevalence over a ten year period. Br Dent J 1999; 186: 72–79.
Chate R A C . Evaluation of a dental practice cardiopulmonary resuscitation training scheme. Br Dent J 1996; 181: 416–420.
Goodwin A P L . Cardiopulmonary resuscitation training revisited. J Royal Soc Med 1992; 85: 452–453.
Personal communication: Davies S J . Northern (Eastern) Health Authority regional organiser for general dental practice resuscitation training.
Chapman P J . A questionnaire survey of dentists regarding knowledge and perceived competence in resuscitation and occurrence of resuscitation emergencies. Aust Dent J 1995; 40: 98–103.
Hussain I, Matthews R W, Scully C . Cardiopulmonary resuscitation skills of dental personnel. Br Dent J 1992; 173: 173–174.
Acknowledgements
The authors would like to thank the Astra Foundation for their generosity in funding this project, with grateful thanks also to the Medical & Dental Defence Union of Scotland, Doncaster Royal Infirmary, Evans Medical, Laerdal Medical Ltd, Roche Products Ltd, TriCoDent Ltd and BOC Medical Gases for additional financial support. Thanks are due to Laura Stead and the Clinical Audit department at Doncaster Royal Infirmary for production and distribution of the questionnaires. We also wish to thank Mr David Landes for guidance in setting up the project and Professor Martin Thornhill for advice on presentation of the data. We are indebted to all those who so kindly responded to this survey.
Author information
Authors and Affiliations
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Atherton, G., McCaul, J. & Williams, S. Medical emergencies in general dental practice in Great Britain Part 3: perceptions of training and competence of GDPs in their management. Br Dent J 186, 234–237 (1999). https://doi.org/10.1038/sj.bdj.4800073
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4800073
