
Abstract
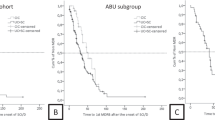
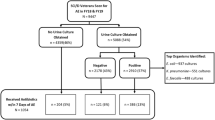
A prospective study to evaluate the microbiological efficacy of antimicrobial treatment for urinary tract infection (UTI) was performed in 64 catheter-free spinal cord injured (SCI) patients who were visited monthly by a public health nurse who collected urine for culture and urinalysis. Patients also mailed urine dip slides for weekly bacterial counts. UTI was defined as a culture yielding ≥ 100,000 colonies/ml. Treatment was given to asymptomatic patients only if pyuria (≥10 urinary leukocytes/high powered microscopic field) was present. Initial treatment was for 7–14 days (group 1). When it became apparent during the study that eradication was difficult and relapse or reinfection frequently occurred within a short time after cessation of antibiotic, a second treatment course of ≥ 28 days (group 2) was given. By the end of the study, in which all patients were followed for a minimum of 30 days post treatment, 39/42 (93%) cases in group 1 and 11/13 (85%) in group 2 who had initial eradication, had relapsed or become reinfected. The median number of days and standard error for group 1 to relapse or become reinfected was 16 ± 2.5, and for group 2 it was 27 ± 6. Development of drug resistance was documented when bacteria isolated prior to any treatment were compared with strains isolated after ≥ 28 days of antibiotics. In this study, urine sterility was achieved in a minority of treated UTIs and was relatively short lived. Advisability of treating asymptomatic UTI following SCI is questionable from both a medical-economic and microbiologic standpoint, particularly in view of the likelihood of inducing multidrug resistance with prolonged antibiotic exposure.
Similar content being viewed by others
Article PDF
References
Kuhlemeier K V, McEachran A B, Lloyd L K, Stover S L, Tauxe W N, Dubovsky E V et al (1984) Renal function after acute and chronic spinal cord injury. 131: 439–445.
Anderson R U, Hatami-tehrani G (1979) Monitoring for bacteriuria in spinal cord-injured patients on intermittent catheterization. Urology 14: 244–246.
Gribble M J, McCallum N M, Schecter M T (1988) Evaluation of diagnostic criteria for bacteriuria in acutely spinal cord injured patients undergoing intermittent catheterization. Diagn Microbiol Infect Dis 9: 197–206.
Deresinski S C, Perkash I (1985) Urinary tract infections in male spinal cord injured patients part two: diagnostic value of symptoms and of quantitative urinalysis. J Am Paraplegia Soc 8: 7–10.
Stickler D J, Chawla J C (1988) An appraisal of antibiotic policies for urinary tract infections in patients with spinal cord injuries undergoing long-term catheterization. Paraplegia 26: 215–225.
Fleiss J L (1981) Statistical Methods for Rates and Proportions. John Wiley and Sons, New York.
Kaplan E L, Meier P (1958) Nonparametric estimation from incomplete observations. J Am Statistical Assoc 53: 457–481.
Stover S L, Lloyd L K, Waites K B, Jackson A B (1989) Urinary tract infection in spinal cord injury. Arch Phys Med Rehabil 70: 47–54.
Stannard A J, Sharples S J, Norman P M, Tillotson G S (1990) Ciprofloxacin therapy of urinary tract infections in paraplegic and tetraplegic patients: a bacteriological assessment. J Antimicrob Chemother (Suppl F) 26: 13–18.
Pedersen S S, Horbov S, Biering-Sorensen F, Hoiby N (1990) Peroral treatment with ciprofloxacin of patients with spinal cord lesion and bacteriuria caused by multiply resistant bacteria. Paraplegia 28: 41–47.
Waites K B, Canupp K C, DeVivo M J (1990) Norfloxacin treatment of nosocomial urinary tract infection in patients undergoing intermittent catheterization following spinal cord injury. Curr Ther Res 48: 503–511.
Waites K B, Canupp K C, DeVivo M J (1991) Efficacy and tolerance of norfloxacin in treatment of complicated urinary tract infection in outpatients with neurogenic bladder secondary to spinal cord injury. Urology 38: 589–596.
Elliott T S J, Slack R C B, Bishop M C (1986) Scanning electron microscopy and bacteriology of the human bladder in acute and chronic urinary tract infections. In: Asscher AW, Brumfitt W, editors. Microbial Diseases in Nephrology. J Wiley & Sons, New York: 31.
Boerema J B J, Van Saene K F (1986) Norfloxacin treatment in complicated urinary tract infection. Scand J Infect Dis (Suppl) 48: 20–26.
Donovan W H, Stolov W C, Clowers D E, Clowers M R (1978) Bacteriuria during intermittent catheterization following spinal cord injury. Arch Phys Med Rehabil 59: 351–357.
Donovan W H, Hull R, Cifu X, Brown H D, Smith N J (1990) Use of plasmid analysis to determine the source of bacterial invasion of the urinary tract. Paraplegia 28: 573–582.
Fawcett C, Chawla J C, Quoraishi A, Stickler D J (1986) A study of the skin flora of spinal cord injured patients. J Hosp Infect 8: 149–158.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Waites, K., Canupp, K. & De Vivo, M. Eradication of urinary tract infection following spinal cord injury. Spinal Cord 31, 645–652 (1993). https://doi.org/10.1038/sc.1993.104
Issue Date:
DOI: https://doi.org/10.1038/sc.1993.104
Keywords
This article is cited by
-
Prevention of Urinary Tract Infection for Patients with Neurogenic Bladder
Current Bladder Dysfunction Reports (2014)
-
Urinary Tract Infections in Patients with Spinal Cord Injuries
Current Infectious Disease Reports (2011)
-
Antibiotic therapy for patients with spinal cord injury undergoing urologic procedures
Advances in Therapy (2006)
-
Self-appraised problem-solving skills and the prediction of secondary complications among persons with spinal cord injuries
Journal of Clinical Psychology in Medical Settings (1994)
