
Abstract
Design Multi-centre split mouth randomised controlled trial.
Intervention Following prophylaxis, isolation, etching and drying the allocated resin-based fissure sealant (RBS) was applied according to the manufacturer's instructions. Reviews were undertaken by a blinded observer at 6,12,18 and 24 months. Operators and observers were calibrated for ICDAS .
Outcome measure The primary outcome was the presence of an ICDAS (International Caries Detection and Assessment System) 3-6 lesion on sealed tooth during the two-year follow-up. Sealant retention was a secondary outcome.
Results Four hundred children (663 tooth pairs) were randomised, 290 children (483 tooth pairs) completed the two-year follow up. There was a lower risk of ICDAS 3-6 lesions in sealed molars; Hazard ratio [HR] = 0.16 (95% CI: 0.14 - 0.19). The effect was similar for both fluoride; HR= 0.15 (95% CI: 0.12 - 0.19) and non-fluoride sealants; HR= 0.18 (95% (CI: 0.15 - 0.21)
Conclusions Sealant placement reduced the risk of ICDAS 3-6 lesions at 24 months; similar reductions in caries were seen for fluoride and non-fluoride sealants.
Similar content being viewed by others

A Commentary on
Muller-Bolla M, Courson F, Lupi-Pégurier L, Tardieu C, Mohit S, Staccini P, Velly AM.
Effectiveness of Resin-Based Sealants with and without Fluoride Placed in a High Caries Risk Population: Multicentric 2-Year Randomized Clinical Trial. Caries Res 2018; 52: 312-322. doi:10.1159/000486426. [Epub ahead of print] PubMed PMID: 29495020.

GRADE rating
Commentary
The primary objective of this study is stated as assessing the effectiveness of RBS in preventing the occurrence of ICDAS 3-6 caries lesions within a two-year follow-up. This represents cavitated caries lesions within enamel (ICDAS 3) and all caries into dentine of any severity (ICDAS 4-6). A second objective was to assess the effectiveness of sealants with fluoride and without fluoride. Also examined were sealant retention rates and risk factors implicated in carious and retention outcomes.
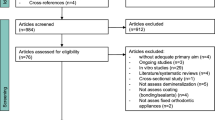
Children of a wide age range (5-15 years) were included in the study, one or two pairs of contralateral molar teeth were selected per child. Within each pair one tooth was either sealed with a fluoride containing sealant or a non-fluoride containing sealant, while the control tooth on the other side was left unsealed. To be included in the study each tooth pair had to be either caries free (ICDAS 0) or be affected by no more than a non-cavitated caries lesion (ICDAS 1,2). To be eligible the child had to be deemed at risk of dental caries as evidenced by at least one ICDAS lesion at baseline (although it is not clear whether this had to be in a permanent tooth).
This study was designed as a split-mouth randomised clinical trial. While the study has been well conducted and reported, there are a number of factors that merit comment. The clinical outcome was determined at 24 months, the minimum time at which it is possible to make a useful diagnosis of caries increment. Interestingly, the authors report that the total duration of the study was five years and it was closed in 2013. This leaves me wondering why a study that started in 2008, reporting in 2018, only presents data at 24 months. Why have the authors not reported data at the more conventional 36 months or even 48 months? This would have represented even more robust data.
The primary outcome of the study is caries prevention and comparison of the sealed surfaces with the unsealed contralateral molar. It was on this parameter that the study was powered. Caries effectiveness was potentially not the most novel aspect of this study - as the authors note, it is well established that fissure sealants are effective in caries prevention. It might be argued that it was not appropriate to test a proven caries preventive measure against a no treatment control, particularly in high-risk children.
Perhaps a more interesting primary question would have been whether there is a difference in clinical effectiveness in the fluoride containing and non-fluoride containing sealants. The authors conclude that the effect of the sealant was similar irrespective of sealant type. This finding has however to be inconclusive for two reasons. The study was not powered to detect such a difference but perhaps more importantly, it has to be queried whether a split-mouth design is appropriate to test a fluoride leaching product, due to possible cross-over contamination effects.
The 290 (72%) children retained in the study means that study was adequately powered from the perspective of caries prevention. The data presented suggest that teeth with either deep occlusal fissures or non-cavitated enamel caries at the outset fared less well than sound teeth, in that in these circumstances, the protective effect of the fissure sealants was reduced. I would argue that this does not however suggest that such teeth should not be fissure sealed. However, it is important in these circumstances, indeed in all circumstances, that fissure sealants are reviewed regularly and repaired if they are not covering the entire pit and fissure system.
A key determinant of sealant effectiveness is retention rates. In this study 70% were retained intact at 24 months. It is not clear if the sealants were 'topped-up' or repaired during the study but a retention rate of this magnitude can be considered good, and possibly reflects the high standards of moisture control employed during placement, namely the use of rubber dam.
In summary, this study provides further evidence of the caries protective effect of fissure sealants, but despite the prominence given to sealants with and without fluoride in the title of the paper, the work was unable to determine whether fluoride containing resin-based sealants provide any positive effect above a standard resin-based sealants other than the potential marketing effect.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chestnutt, I. Are fluoride-containing sealants more effective than non-fluoride sealants? . Evid Based Dent 20, 12–13 (2019). https://doi.org/10.1038/s41432-019-0019-4
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41432-019-0019-4
