
Abstract
Background
Overuse of sedation and anesthesia causes delays in gastrojejunostomy tube (GJ) exchanges, increased risk of complications, unnecessary use of resources, preventable hospital admissions, and an adverse impact on patient and family experience. Our hospital was over-utilizing sedation and anesthesia, and we aimed to decrease this use from 78% to 20% within two years.
Methods
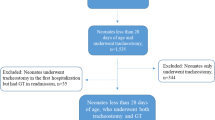
An interdisciplinary quality improvement team comprehensively evaluated current processes for GJ tube exchanges through a retrospective chart review for baseline data with prospective time series analysis after improvement implementation. The primary outcome measure was the percentage of pediatric patients that utilized sedation or anesthesia for routine GJ tube exchanges.
Results
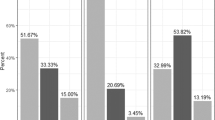
A statistical process control p-chart was used to calculate and show changes over time for patients (n = 45 patients average). The median percent of pediatric GJ tube exchanges performed with sedation or anesthesia decreased from 77.8% to 11.3%. Most patients (76%) were covered by Medicaid programs; with low reimbursement rates, decreased anesthesiologist billing revenue does not have a negative financial impact.
Conclusions
An interprofessional improvement initiative that engaged patients and families, incorporated pediatric-specific staff services, and developed systematic weaning was associated with a significant decrease in the overuse of sedation and anesthesia for GJ tube exchanges.
Impact
We believe that this work is highly relevant and impactful for medical centers caring for children who require gastrojejunostomy tubes, an increasingly common approach to management of children with feeding issues. There is very little literature available on the use of sedation or anesthesia for changing these tubes. While large children’s medical centers in the USA usually do not utilize sedation or anesthesia, there are likely many serious outliers, especially when children receive care outside of a pediatric specific institution. This paper brings awareness to this serious issue and provides information about how we changed care to achieve higher patient safety and lower medical costs.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 14 print issues and online access
$259.00 per year
only $18.50 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

Data availability
The dataset generated and analyzed during the current study is not publicly available due to HIPPA protection but is available from the corresponding author on reasonable request. Reasonable request would also include that the dataset be de-identified prior to sharing.
References
Avinashi, V. et al. A241 A Review of 101 Children with Gastro-jejunal Feeding Tubes Including Their Complications at BC Children’s Hospital. J. Can. Assoc. Gastroenterol. 4, 296–297 (2021).
Wilson, R. E. et al. A Natural History of Gastrojejunostomy Tubes in Children. J. Surg. Res. 245, 461–466 (2020).
Shah, M., Klooster, M., Yanni, G. & Shah, A. Frequency and methods of gastrojejunal tube replacement in children. Curr. Gastroenterol. Rep. 12, 223–227 (2010).
Hoang, T. T. et al. Routine Elective Gastrojejunostomy Tube Changes Are Associated with Reduced Tube Complications and Radiation Exposure. J. Pediatr. Gastroenterol. Nutr. 76, 80–83 (2023).
Provost, L. P., Murray, S. K. The Health Care Data Guide: Learning from Data for Improvement (Jossey-Bass, 2011).
Author information
Authors and Affiliations
Contributions
All authors have met the Pediatric Research authorship requirements. Qianqian Ellie Cheng drafted the initial manuscript; reviewed and revised the manuscript; and approved the final manuscript as submitted. Jan Schriefer coached the quality improvement team, helped draft and revise the manuscript, and approved the final manuscript as submitted. Tina Sosa provided critical input for analyzing and presenting the project, helped draft and revise the manuscript, and approved the final manuscript as submitted. Sarah Haen helped to develop the project and performed critical clinical work related to implementation and maintenance of the program, and she reviewed and approved the final manuscript as submitted. Samantha Ferguson helped to develop the project and performed critical clinical work related to implementation and maintenance of the program, and she reviewed and approved the final manuscript as submitted. Alexander Clark assisted with data analytics, reviewed and approved the final manuscript as submitted. Christine Boerman extracted data from EMR used to analyze and develop the plans for this project; she reviewed and approved the final manuscript as submitted. Carly Hochreiter performed data analysis, developed the Tableau dashboards, reviewed and approved the final manuscript as submitted. Megan Gabel participated on our QI team and was instrumental in leading the pediatric gastrointestinal team to implement the program; she reviewed and approved the final manuscript as submitted. Arvid Yung participated on our QI team and was instrumental in leading the pediatric anesthesiology team to implement the program; he reviewed and approved the final manuscript as submitted. David Lee participated on our QI team and was instrumental in leading the interventional radiology team to implement the program; he reviewed and approved the final manuscript as submitted. Kate Ackerman co-wrote the manuscript, developed and led the project, analyzed the data, wrote and approved of the final manuscript as submitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent Statement
Patient consent was not required for this paper.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Cheng, Q.E., Schriefer, J., Sosa, T. et al. GJ Express: an improvement initiative to decrease sedation and anesthesia for gastrojejunostomy tube exchanges. Pediatr Res (2024). https://doi.org/10.1038/s41390-024-03070-1
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41390-024-03070-1
