
Abstract
Background
Normative blood pressure (BP) values and definition of hypertension (HTN) in children in outpatient setting cannot be reliably used for inpatient therapy initiation. No normative exists to describe HTN in hospitalized pediatric populations. We aimed to study the prevalence of hypertension and produce normative BP values in hospitalized children.
Methods
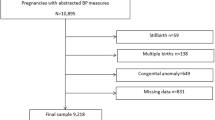
Cross sectional observational study of all children hospitalized on acute care floors, ≥2 and <18 years age, at Stanford Children’s Hospital, from Jan-01-2014 to Dec-31-2018. Cohort included 7468 hospital encounters with a total of 118,423 automated, oscillometric, BPs measured in the upper extremity during a hospitalization of >24 hours.
Results
Overall prevalence of HTN, defined by outpatient guidelines, was 12–48% in boys and 6–39% in girls, stage 1 systolic HTN in 12–38% of boys and 6–31% of girls, stage 2 systolic HTN in 3–10% of boys and 1–8% of girls. Centile curves were derived demonstrating overall higher BP reading for hospitalized patients compared to the outpatient setting.
Conclusion
Higher blood pressures are anticipated during hospitalization. Thresholds provided by the centile curves generated in this study may provide the clinician with some guidance on how to manage hospitalized pediatric patients based on clinical circumstances.
Impact
-
Hospitalized children have higher blood pressures compared to patients in the ambulatory setting, hence outpatient normative blood pressure values cannot be reliably used for inpatient therapy initiation.
-
No normative exists to describe hypertension in hospitalized pediatric populations.
-
The thresholds provided by the centile curves generated in this study may provide the clinician with some guidance on how to manage hospitalized pediatric patients based on clinical circumstances.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 14 print issues and online access
$259.00 per year
only $18.50 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

Data availability
De-identified data from the analysis can be made available after authors’ review of request and might require compilation of specific categories to protect patient privacy.
References
Chaudhuri, A. & Sutherland, S. M. Evaluation and management of elevated blood pressures in hospitalized children. Pediatr. Nephrol. (Berl., Ger.) 34, 1671–1681 (2019).
Lurbe, E. et al. 2016 European society of hypertension guidelines for the management of high blood pressure in children and adolescents. J. Hypertens. 34, 1887–1920 (2016).
Baker-Smith, C. M. et al. Diagnosis, evaluation, and management of high blood pressure in children and adolescents. Pediatrics 142, e20182096 (2018).
Bell, C. S., Samuel, J. P. & Samuels, J. A. Prevalence of hypertension in children. Hypertension 73, 148–152 (2019).
Song, P. et al. Global prevalence of hypertension in children: A systematic review and meta-analysis. JAMA Pediatr. 173, 1154–1163 (2019).
Tran, C. L. et al. Recent trends in healthcare utilization among children and adolescents with hypertension in the United States. Hypertension 60, 296–302 (2012).
Axon, R. N., Cousineau, L. & Egan, B. M. Prevalence and management of hypertension in the inpatient setting: A systematic review. J. Hosp. Med. 6, 417–422 (2011).
Stanistreet, B., Nicholas, J. A. & Bisognano, J. D. An evidence-based review of elevated blood pressure for the inpatient. Am. J. Med. 133, 165–169 (2020).
Vondracek, S., Scoular, S. & Patel, T. Management of severe asymptomatic hypertension in the hospitalized patient. J. Am. Soc. Hypertens. 10, 974–984 (2016).
James, P. A. et al. 2014 Evidence-based guideline for the management of high blood pressure in adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (Jnc 8). JAMA 311, 507–520 (2014).
Weder, A. B. Treating acute hypertension in the hospital: A lacuna in the guidelines. Hypertension 57, 18–20 (2011).
Sharma, P. Inpatient Hypertension Management.
Sleeper, E. J., Ariza, A. J. & Binns, H. J. Do hospitalized pediatric patients have weight and blood pressure concerns identified? J. Pediatr. 154, 213–217 (2009).
Alperstein, W., Corrales-Medina, F. F., Tamariz, L., Palacio, A. M. & Davis, J. A. Prevalence of hypertension (Htn) and cardiovascular risk factors in a hospitalized pediatric hemophilia population. J. Pediatr. Hematol. Oncol. 40, 196–199 (2018).
Ehrmann, B. J., Selewski, D. T., Troost, J. P., Hieber, S. M. & Gipson, D. S. Hypertension and health outcomes in the Picu. Pediatr. Crit. Care Med. 15, 417–427 (2014).
Park, M. K., Menard, S. W. & Yuan, C. Comparison of auscultatory and oscillometric blood pressures. Arch. Pediatr. Adolesc. Med. 155, 50–53 (2001).
Schell, K. et al. Comparison of arm and calf automatic noninvasive blood pressures in pediatric intensive care patients. J. Pediatr. Nurs. 26, 3–12 (2011).
Schell, K., Morse, K. & Waterhouse, J. K. Forearm and upper-arm oscillometric blood pressure comparison in acutely Ill adults. West J. Nurs. Res. 32, 322–340 (2010).
Eser, I., Khorshid, L., Gunes, U. Y. & Demir, Y. The effect of different body positions on blood pressure. J. Clin. Nurs. 16, 137–140 (2007).
Netea, R. T., Lenders, J. W., Smits, P. & Thien, T. Both body and arm position significantly influence blood pressure measurement. J. Hum. Hypertens. 17, 459–462 (2003).
Kipps, A. K. et al. Inpatient-derived vital sign parameters implementation: An initiative to decrease alarm burden. Pediatrics 140, e20162458 (2017).
Bonafide, C. P. et al. Development of heart and respiratory rate percentile curves for hospitalized children. Pediatrics 131, e1150–e1157 (2013).
Goel, V. V. et al. Safety analysis of proposed data-driven physiologic alarm parameters for hospitalized children. J. Hosp. Med 11, 817–823 (2016).
Eytan, D., Goodwin, A. J., Greer, R., Guerguerian, A. M. & Laussen, P. C. Heart rate and blood pressure centile curves and distributions by age of hospitalized critically Ill children. Front Pediatr. 5, 52 (2017).
Zubrow, A. B., Hulman, S., Kushner, H. & Falkner, B. Determinants of blood pressure in infants admitted to neonatal intensive care units: A prospective multicenter study. philadelphia neonatal blood pressure study group. J. Perinatol. 15, 470–479 (1995).
Roberts, J. S., Yanay, O. & Barry, D. Age-based percentiles of measured mean arterial pressure in pediatric patients in a hospital setting. Pediatr. Crit. Care Med. 21, e759–e768 (2020).
Research Informatics Center, Stanford University” and the Stanford Ctsa Award Number Ul1tr003142.
Starr: “This Research Used Data or Services Provided by Starr, “Stanford Medicine Research Data Repository,” a Clinical Data Warehouse Containing Live Epic Data from Stanford Health Care, the Stanford Children’s Hospital, the University Healthcare Alliance and Packard Children’s Health Alliance Clinics and Other Auxiliary Data from Hospital Applications Such as Radiology Pacs. Starr Platform Is Developed and Operated by Stanford Medicine Research It Team and Is Made Possible by Stanford School of Medicine Research Office.
Rosner, B., Cook, N., Portman, R., Daniels, S. & Falkner, B. Determination of blood pressure percentiles in normal-weight children: Some methodological issues. Am. J. Epidemiol. 167, 653–666 (2008).
Centers for Disease Control and Prevention, National Center for Health Statistics. Cdc Growth Charts: United States. http://www.Cdc.Gov/Growthcharts/. May 30, 2000. Accessed May 1, (2021).
Flynn, J. T. et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 140, e20171904 (2017).
Stasinopoulos, M. D., Rigby, R. A. & Bastiani, F. D. Gamlss: A distributional regression approach. Stat. Model. 18, 248–273 (2018).
Rigby, R. A. & Stasinopoulos, D. M. Smooth centile curves for skew and kurtotic data modelled using the box-cox power exponential distribution. Stat. Med. 23, 3053–3076 (2004).
Distributions for Modeling Location, Scale, and Shape: Using Gamlss in R. In: Routledge Crc Press. https://www.Routledge.Com/Distributions-for-Modeling-Location-Scale-and-Shape-Using-Gamlss-in-R/Rigby-Stasinopoulos-Heller-Bastiani/P/Book/9781032089423. Accessed 18 May (2021).
R Core Team (2019) R: A Language and Environment for Statistical Computing.
Anderson, T. S. et al. Clinical outcomes after intensifying antihypertensive medication regimens among older adults at hospital discharge. JAMA Intern. Med. 179, 1528–1536 (2019).
Rastogi, R. et al. Treatment and outcomes of inpatient hypertension among adults with noncardiac admissions. JAMA Intern. Med. 181, 345–352 (2021).
Yang, W. C., Lin, M. J., Chen, C. Y. & Wu, H. P. Clinical overview of hypertensive crisis in children. World J. Clin. Cases 3, 510–513 (2015).
Sutherland, S. M., Kaelber, D. C., Downing, N. L., Goel, V. V. & Longhurst, C. A. Electronic health record-enabled research in children using the electronic health record for clinical discovery. Pediatr. Clin. North Am. 63, 251–268 (2016).
Fleming, S. et al. Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: A systematic review of observational studies. Lancet 377, 1011–1018 (2011).
Daymont, C., Bonafide, C. P. & Brady, P. W. Heart rates in hospitalized children by age and body temperature. Pediatrics 135, E1173–E1181 (2015).
Porcelli, P. J. & Rosenbloom, S. T. Comparison of new modeling methods for postnatal weight in elbw infants using prenatal and postnatal data. J. Pediatr. Gastroenterol. Nutr. 59, e2–e8 (2014).
Rosenbloom, S. T. et al. Specialized pediatric growth charts for electronic health record systems: The example of down syndrome. AMIA Annu Symp. Proc. 2010, 687–691 (2010).
Bennett, W. E. Jr., Hendrix, K. S., Thompson, R. T., Carroll, A. E. & Downs, S. M. The natural history of weight percentile changes in the first year of life. JAMA Pediatr. 168, 681–682 (2014).
Funding
AMU was a Paul and Yuanbi Ramsay Endowed Postdoctoral Fellow of the Maternal and Child Health Research Institute at Stanford during a period of production of this manuscript. The other authors received no additional funding.
Author information
Authors and Affiliations
Contributions
Study design: Amanda M. Uber, Jialin Han, Maria E. Montez-Rath, Abanti Chaudhuri. Data collection and analysis: Jialin Han, Maria E. Montez-Rath. Data verification: Amanda M. Uber, Jialin Han, Maria E. Montez-Rath, Abanti Chaudhuri. Manuscript writing: Amanda M. Uber, Jialin Han, Paul Grimm, Maria E. Montez-Rath, Abanti Chaudhuri. Writing of the first draft of the manuscript: Amanda M. Uber, Jialin Han, Maria E. Montez-Rath, Abanti Chaudhuri. Final approval of the version to be published: Amanda M. Uber, Jialin Han, Maria E. Montez-Rath, Abanti Chaudhuri
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
IRB approved; no informed consent was required for the collection of this data.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Uber, A.M., Han, J., Grimm, P. et al. Defining systolic blood pressure normative values in hospitalized pediatric patients: a single center experience. Pediatr Res (2024). https://doi.org/10.1038/s41390-024-03059-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41390-024-03059-w
