
Abstract
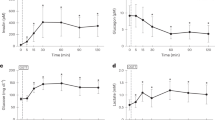
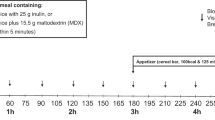
Summary: Continuous nocturnal intragastric feeding, combined with frequent daytime feedings, has been reported to improve both linear growth and the metabolic abnormalities in patients with glucose-6-phosphatase deficiency (Type I Glycogen Storage Disease). However, elevated blood levels of lactate have persisted. The present studies explore the relationship between blood lactate concentrations in six patients with glucose-6-phosphatase deficiency and variations in the rate and composition of the intragastric feeding. Blood lactate and plasma glucose concentrations were determined at rates of dextrose administration ranging from 3–34 mg/kg/min. Dextrose infusion at 100–200% of estimated normal glucose production rates gave the best control of blood lactate concentrations. Lower rates of dextrose infusion resulted in significantly higher blood lactate levels; higher rates produced hyperglycemia, but no significant further reduction of blood lactate. At identical rates of glucose administration, a dextrose-containing infant formula and a high carbohydrate enteric feeding solution gave no significant improvement hi control of blood lactate levels compared to dextrose alone. Plasma glucose levels fell more rapidly when intragastric feeding was stopped than after a mixed meal and hypoglycemia appeared to develop before counter-regulatory responses could be mobilized. These observations may account for the increased susceptibility to symptomatic hypoglycemia reported in patients treated with intragastric feeding.
Speculation: These results indicate that intragastric glucose infusion at a rate equal to or slightly greater than normal hepatic glucose production gives maximal control of the metabolic abnormalities in patients with glucose-6-phosphatase deficiency. Complete normalization of hyperlactatemia and hypertriglyceridemia in these patients may require the development of additional forms of therapy.
Similar content being viewed by others

Article PDF
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Stanley, C., Mills, J. & Baker, L. Intragastric Feeding in Type I Glycogen Storage Disease: Factors Affecting the Control of Lactic Acidemia. Pediatr Res 15, 1504–1508 (1981). https://doi.org/10.1203/00006450-198112000-00010
Issue Date:
DOI: https://doi.org/10.1203/00006450-198112000-00010
This article is cited by
-
Effect of continuous glucose therapy with uncooked cornstarch on the long-term clinical course of type 1a glycogen storage disease
European Journal of Pediatrics (2002)
-
Type I glycogen storage disease: favourable outcome on a strict management regimen avoiding increased lactate production during childhood and adolescence
European Journal of Pediatrics (2002)
-
Chronic pancreatitis in a child with glycogen storage disease type 1
European Journal of Pediatrics (1991)
-
Hyperglycaemia associated with lactic acidaemia in a renal allograft recipient with type I glycogen storage disease
Journal of Inherited Metabolic Disease (1991)
-
Hyperfiltration and renal disease in glycogen storage disease, type I
Kidney International (1989)
