
Abstract
Extract: The present observations were undertaken to establish the response of children to the acute administration of ammonium chloride, in order to provide a basis for identifying and interpreting abnormalities in the mechanisms involved in renal acid base regulation. Fifty-eight normal children aged 4 to 13 years were studied before and for 5 hours following administration of ammonium chloride. Group A, consisting of 23 children, received 75 mEq/m2 body surface area or 2.75 mEq/kg body weight. Group B, consisting of 35 children, received 150 mEq/m2, or 5.45 mEq/kg.
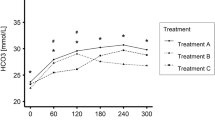
Values for serum electrolytes, urea, creatinine, osmolality and acid-base parameters in children in Groups A and B are shown in tables I and III. Urinary pH and rates of excretion of titratable acid and ammonium are shown in tables II and IV. The relations between blood tCO2 and urinary concentration of H+, rate of excretion of titratable acid, and rate of excretion of ammonium for all subjects are shown in figures 1-3. Progressively lower values of pH were observed over the entire range of tCO2 studied. During control periods, an inverse correlation was present between tCO2 and rates of excretion of both titratable acid and ammonium. At levels of tCO2 below 22.5 mmoles/l, the rate of excretion of TA and ammonium became constant, with mean rates of excretion of 52 μEq/min/1.73 m2 (range, ± 2 SD, 33 to 71), and 73 μEq/min/1.73 m2 (46 to 100), respectively.
These data are interpreted as demonstrating the importance of the blood tCO2 or, more precisely, the concentratibn of bicarbonate in glomerular filtrate in urinary acidification mechanisms as well as in control of excretion of bicarbonate. Assessment of renal acidifying mechanisms requires administration of sufficient ammonium chloride or other acidifying substance to depress blood tCO2 to levels well below the renal threshold.
The physiologic validity of the hydrogen ion clearance index must be questioned, since correcting rates of excretion of hydrogen ion for concentration of total CO2 in blood presumes that there is a fixed relation between these two measurements. In figure 4, urinary excretion of total hydrogen ion is plotted as a function of blood tCO2. Hydrogen ion excretion, negligible at tCO2 levels of 26 or more, increases steadily as tCO2 falls to values below the threshold. The rate of excretion then reaches maximal levels, despite further reduction in blood tCO2. Thus, the hydrogen ion clearance index is valid only over the range of blood tCO2 in which there is a linear relationship with rate of excretion of hydrogen ion. Renal acidification mechanisms should be evaluated with blood tCO2 several millimoles below the threshold, assuring a maximal response and permitting direct comparison with normals. In subjects with a normal bicarbonate threshold, blood tCO2 should be depressed at least to 17–18 mmoles/l in infants and 20–21 mmoles/l in older children. If an abnormal bicarbonate threshold is present the dose must be adjusted accordingly.
Speculation: These studies suggest that both the concentration of bicarbonate in glomerular filtrate and the level of the bicarbonate threshold play major roles in the regulation of renal excretion of hydrogen ion.
Similar content being viewed by others

Article PDF
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Edelmann, C., Boichis, H., Soriano, J. et al. The Renal Response of Children to Acute Ammonium Chloride Acidosis. Pediatr Res 1, 452–460 (1967). https://doi.org/10.1203/00006450-196711000-00004
Issue Date:
DOI: https://doi.org/10.1203/00006450-196711000-00004
Keywords
This article is cited by
-
Clinical and laboratory approaches in the diagnosis of renal tubular acidosis
Pediatric Nephrology (2015)
-
Diagnosis of distal renal tubular acidosis: use of furosemide plus fludrocortisone versus ammonium chloride
Nature Clinical Practice Nephrology (2007)
-
Acidosis increases magnesiuria in children with distal renal tubular acidosis
Pediatric Nephrology (2004)
-
Aldosterone and testosterone producing adrenal adenoma in childhood
Journal of Endocrinological Investigation (1995)
-
Pathophysiology of the renal acidification defect present in the syndrome of familial hypomagnesaemia-hypercalciuria
Pediatric Nephrology (1994)
