
Abstract
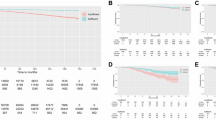
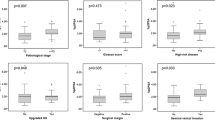
The objective of this study was to preoperatively predict non-organ-confined disease in patients considering radical prostatectomy. To account for the stage migration seen in prostate cancer, we included only those patients who underwent prostatectomy after the year 2000. Information on a cohort of 1895 patients who underwent radical prostatectomy from 2000 to 2008 was retrieved from the Duke Prostate Center database. Race (African American, non-African American), body mass index, age at surgery, PSA, biopsy Gleason sum (<7, 7 and >7) and clinical tumor stage (cT1, cT2/3) were analyzed by univariate analysis followed by logistic regression analysis. The Duke Interactive Clinical Equation for staging (DICE-S score) was calculated from the logistic regression model. The model was then internally validated using a bootstrapping technique. Biopsy Gleason sums 7 and >7 were more likely to have non-organ-confined disease compared with <7 (OR=2.97, Gleason sum=7; OR=3.25, Gleason sum>7). Clinical tumor stage, cT2/3, predicted non-organ-confined disease (OR=1.58). Older age was associated with non-organ-confined disease (OR=1.02), as was greater PSA (OR=1.12). DICE-S equation x=ln (p/1−p)=−3.627+0.019 (age)+0.109 (PSA)+1.087 (bGleason=7)+1.180 (bGleason >7)+0.459 (clinical T stage >T1), where p=(ex)/(1+ex). A concordance index (prediction accuracy) of 0.73 was reached on internal validation. Using the DICE-S score, age, PSA, biopsy Gleason sum and clinical tumor stage, we can predict non-organ-confined disease in radical prostatectomy at an acceptable accuracy. Preoperative information on disease stage may aid in treatment decisions and surgical approach.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
Bianco Jr FJ, Scardino PT, Eastham JA . Radical prostatectomy: long-term cancer control and recovery of sexual and urinary function (‘trifecta’). Urology 2005; 66: 83.
Brown JA, Rodin DM, Harisinghani M, Dahl DM . Impact of preoperative endorectal MRI stage classification on neurovascular bundle sparing aggressiveness and the radical prostatectomy positive margin rate. Urol Oncol 2008; 27: 174–179.
Wolf Jr JS, Shinohara K, Carroll PR, Narayan P . Combined role of transrectal ultrasonography, Gleason score, and prostate-specific antigen in predicting organ-confined prostate cancer. Urology 1993; 42: 131.
Hricak H, Wang L, Wei DC, Coakley FV, Akin O, Reuter VE et al. The role of preoperative endorectal magnetic resonance imaging in the decision regarding whether to preserve or resect neurovascular bundles during radical retropubic prostatectomy. Cancer 2004; 100: 2655.
Bernstein MR, Cangiano T, D’Amico A, Chittams J, Hardy C, Whittington RD et al. Endorectal coil magnetic resonance imaging and clinicopathologic findings in T1c adenocarcinoma of the prostate. Urol Oncol 2000; 5: 104.
Desireddi NV, Roehl KA, Loeb S, Yu X, Griffin CR, Kundu SK et al. Improved stage and grade-specific progression-free survival rates after radical prostatectomy in the PSA era. Urology 2007; 70: 950.
Dong F, Reuther AM, Magi-Galluzzi C, Zhou M, Kupelian PA, Klein EA . Pathologic stage migration has slowed in the late PSA era. Urology 2007; 70: 839.
Magheli A, Rais-Bahrami S, Trock BJ, Humphreys EB, Partin AW, Han M et al. Prostate specific antigen versus prostate specific antigen density as a prognosticator of pathological characteristics and biochemical recurrence following radical prostatectomy. J Urol 2008; 179: 1780.
Vickers AJ, Bianco FJ, Gonen M, Cronin AM, Eastham JA, Schrag D et al. Effects of pathologic stage on the learning curve for radical prostatectomy: evidence that recurrence in organ-confined cancer is largely related to inadequate surgical technique. Eur Urol 2008; 53: 960.
Ward JF, Zincke H, Bergstralh EJ, Slezak JM, Myers RP, Blute ML . The impact of surgical approach (nerve bundle preservation versus wide local excision) on surgical margins and biochemical recurrence following radical prostatectomy. J Urol 2004; 172: 1328.
Hernandez DJ, Epstein JI, Trock BJ, Tsuzuki T, Carter HB, Walsh PC . Radical retropubic prostatectomy. How often do experienced surgeons have positive surgical margins when there is extraprostatic extension in the region of the neurovascular bundle? J Urol 2005; 173: 446.
Ohori M, Kattan MW, Koh H, Maru N, Slawin KM, Shariat S et al. Predicting the presence and side of extracapsular extension: a nomogram for staging prostate cancer. J Urol 2004; 171: 1844.
Partin AW, Kattan MW, Subong EN, Walsh PC, Wojno KJ, Oesterling JE et al. Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer: a multi-institutional update. JAMA 1997; 277: 1445.
Richstone L, Bianco FJ, Shah HH, Kattan MW, Eastham JA, Scardino PT et al. Radical prostatectomy in men aged >or=70 years: effect of age on upgrading, upstaging, and the accuracy of a preoperative nomogram. BJU Int 2008; 101: 541.
Chun FK, Briganti A, Graefen M, Montorsi F, Porter C, Scattoni V et al. Development and external validation of an extended 10-core biopsy nomogram. Eur Urol 2007; 52: 436.
Shikanov SA, Thong A, Gofrit ON, Zagaja GP, Steinberg GD, Shalhav AL et al. Robotic laparoscopic radical prostatectomy for biopsy Gleason 8 to 10: prediction of favorable pathologic outcome with preoperative parameters. J Endourol 2008; 22: 1477.
Nakanishi H, Troncoso P, Babaian RJ . Prediction of extraprostatic extension in men with biopsy Gleason score of 8 or greater. J Urol 2008; 180: 2441.
Acknowledgements
This study was supported by research funds from the Committee for Urologic Research, Education, and Development (CURED) of Duke University (AAC, LS, BDL, KL, PT, DAS, DMA and JWM).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Caire, A., Sun, L., Lack, B. et al. Predicting non-organ-confined prostate cancer in men diagnosed after 2000. Prostate Cancer Prostatic Dis 13, 248–251 (2010). https://doi.org/10.1038/pcan.2010.15
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pcan.2010.15
