
Abstract
The BK polyomavirus exhibits tropism for the renal tubular epithelium, where it establishes latent infection. Vigorous immunosuppression of renal allograft recipients can lead to reactivation of the infection and the development of polyomavirus-associated nephropathy (PVAN). Clinically, gradually decreasing renal function, viremia and viruria are observed several months after transplantation; allograft failure occurs in 1–10% of patients. Definitive diagnosis requires an allograft biopsy. Histologically, viral replication results in tubular epithelial cell enlargement, karyomegaly and nuclear inclusion bodies. The cytopathic changes are often associated with lysis of tubular epithelial cells, denudation of the basement membrane and an interstitial inflammatory response. The involvement is multifocal; distal nephron segments are more severely affected than proximal segments. Changes observed during light microscopy are suggestive but not pathognomonic for PVAN, and the diagnosis must be confirmed by adjunct studies. Adjunct studies consist of immunohistochemistry on paraffin sections using an antibody to the SV40 large T antigen, or electron microscopy of infected tubular epithelial cells (virions 40 nm in diameter). PVAN manifests in three histologic patterns: pattern A, viral cytopathic changes with no or only minimal inflammation; pattern B, cytopathic and cytolytic lesions with interstitial inflammation; or pattern C, predominantly interstitial fibrosis and tubular atrophy, with variable cytopathic and inflammatory changes. These patterns correlate with clinical outcomes.
Key Points
-
The incidence of polyomavirus-associated nephropathy (PVAN) of renal allografts has increased since the introduction of new-generation immunosuppressive regimens
-
PVAN is caused by the ubiquitous BK virus, which establishes latent infection in urothelium and renal tubular epithelium; latent BK virus can be reactivated by immunosuppression
-
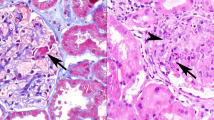
Diagnosis of PVAN requires renal biopsy; histopathological features include enlargement of tubular epithelial cells and development of nuclear inclusion bodies therein, and interstitial inflammation
-
PVAN must be distinguished from other types of viral infections, and acute and chronic rejection
-
Minimization of immunosuppression is the mainstay of PVAN management
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout





Similar content being viewed by others


References
Zuckerman AJ et al. (Eds; 2004) Principles and Practice of Clinical Virology, edn 5. Chichester: John Wiley and Sons Ltd
Pappo O et al. (1996) Human polyoma virus infection of renal allografts: histopathologic diagnosis, clinical significance, and literature review. Mod Pathol 9: 105–109
Boldorini R et al. (2005) Kidney and urinary tract polyomavirus infection and distribution: molecular biology investigation of 10 consecutive autopsies. Arch Pathol Lab Med 129: 69–73
Randhawa P et al. (2005) A comparative study of BK and JC virus infections in organ transplant recipients. J Med Virol 77: 238–243
Kazory A et al. (2003) The first case of JC virus allograft nephropathy. Transplantation 76: 1653–1655
Howell DN et al. (1999) Diagnosis and management of BK polyomavirus interstitial nephritis in renal transplant recipients. Transplantation 68: 1279–1288
Coleman DV et al. (1978) Human polyomavirus (BK) infection and ureteric stenosis in renal allograft recipients. J Clin Pathol 31: 338–347
Ramos E et al. (2002) BK virus nephropathy diagnosis and treatment: experience at the University of Maryland Renal Transplant Program. Clin Transplant 13: 143–153
Binet I et al. (1999) Polyomavirus disease under new immunosuppressive drugs: a cause of renal graft dysfunction and graft loss. Transplantation 67: 918–922
Humar A (2006) Reactivation of viruses in solid organ transplant patients receiving cytomegalovirus prophylaxis. Transplantation 27 (Suppl): S9–S14
Drachenberg CB et al. (2003) BK polyoma virus allograft nephropathy: ultrastructural features from viral cell entry to lysis. Am J Transplant 3: 1383–1392
Drachenberg CB et al. (2005) Polyomavirus disease in renal transplantation: review of pathological findings and diagnostic methods. Hum Pathol 36: 1245–1255
Namba Y et al. (2005) Prevalence, characteristics, and outcome of BK virus nephropathy in Japanese renal transplant patients: analysis in protocol and episode biopsies. Clin Transplant 19: 97–101
Mengel M et al. (2003) Incidence of polyomavirus-nephropathy in renal allografts: influence of modern immunosuppressive drugs. Nephrol Dial Transplant 18: 1190–1196
Bressollette-Bodin C et al. (2005) A prospective longitudinal study of BK virus infection in 104 renal transplant recipients. Am J Transplant 5: 1926–1933
Nickeleit V et al. (2003) Polyomavirus nephropathy: morphology, pathophysiology, and clinical management. Curr Opin Nephrol Hypertens 12: 599–605
Hirsch HH et al. (2005) Polyomavirus-associated nephropathy in renal transplantation: interdisciplinary analyses and recommendations. Transplantation 79: 1277–1286
Trofe J et al. (2006) Polyomavirus-associated nephropathy: update of clinical management in kidney transplant patients. Transplant Infect Dis 8: 76–85
Josephson MA et al. (2006) Polyomavirus-associated nephropathy: update on antiviral strategies. Transplant Infect Dis 8: 95–101
Boldorini R et al. (2005) Periodic assessment of urine and serum by cytology and molecular biology as a diagnostic tool for BK virus nephropathy in renal transplant patients. Acta Cytol 49: 235–243
Vera-Sempere FJ et al. (2005) Polymerase chain reaction detection of BK virus and monitoring of BK nephropathy in renal transplant recipients at the University Hospital La Fe. Transplant Proc 37: 3770–3773
Ramos E et al. (2004) Retransplantation in patients with graft loss caused by polyoma virus nephropathy. Transplantation 77: 131–133
Womer KL et al. (2006) Preemptive retransplantation for BK virus nephropathy: successful outcome despite active viremia. Am J Transplant 6: 7–9
Nickeleit V et al. (2000) BK-virus nephropathy in renal transplants—tubular necrosis, MHC-class II expression and rejection in a puzzling game. Nephrol Dial Transplant 15: 324–332
Nickeleit V et al. (1999) Polyomavirus infection of renal allograft recipients: from latent infection to manifest disease. J Am Soc Nephrol 10: 1080–1089
Ahuja M et al. (2001) Polyoma virus infection after renal transplantation: use of immunostaining as a guide to diagnosis. Transplantation 71: 896–899
Celik B et al. (2004) Glomerular changes in BK virus nephropathy. Hum Pathol 35: 367–370
Nickeleit V and Mihatsch MJ (2005) Histologic changes in polyomavirus allograft nephropathy. In Updates in Nephropathology and Transplantation; Proceedings of the Nephropathology Pre-congress Meeting of the 20th European Congress of Pathology; Paris, 36–40 (Eds Vizjak A et al.) Ljubljana: Institute of Pathology, University of Ljubljana
Gaber LW et al. (2006) Clinical utility of histological features of polyomavirus allograft nephropathy. Transplantation 82: 196–204
Racusen LC et al. (2003) Antibody mediated rejection criteria—an addition to the Banff '97 classification of renal allograft rejection. Am J Transplant 3: 1–7
Solez K et al. (1993) International standardization of criteria for the histologic diagnosis of renal allograft rejection: the Banff working classification of kidney transplant pathology. Kidney Int 44: 411–422
Acknowledgements
The nephropathologic activities of B Ivanyi are supported by the Hungarian Scientific Research Fund (OTKA) via grant T-038271.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
About this article
Cite this article
Liptak, P., Kemeny, E. & Ivanyi, B. Primer: histopathology of polyomavirus-associated nephropathy in renal allografts. Nat Rev Nephrol 2, 631–636 (2006). https://doi.org/10.1038/ncpneph0319
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1038/ncpneph0319
This article is cited by
-
Routine immunohistochemistry study for polyomavirus BK nephropathy in transplanted kidney biopsies, is it recommended?
BMC Nephrology (2021)
-
Early identification of renal transplant recipients with high risk of polyomavirus-associated nephropathy
Medical Microbiology and Immunology (2015)
-
Activation of innate immune defense mechanisms contributes to polyomavirus BK-associated nephropathy
Kidney International (2012)
-
The BK virus in renal transplant recipients—review of pathogenesis, diagnosis, and treatment
Pediatric Nephrology (2011)
