
Abstract
Purpose To identify the area of retina required to provide the visual field for driving and to investigate whether the pattern of panretinal photocoagulation (PRP) for proliferative diabetic retinopathy could be altered to avoid treatment in this area whilst leaving the total number of burns constant.
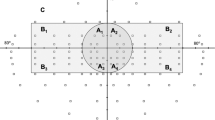
Methods A mathematical model of the emmetropic eye is used to calculate retinal dimensions corresponding to different angles of visual field. These are used to define retinal regions that correspond to the UK DVLC visual field criteria and regions that lie outside this area. Further calculation estimates the number of laser burns applied within these regions for both 500 μm? and 200 μm diameter spot sizes and various burn spacings.
Results Modelling of the number of burns applied in the normal pattern of PRP agrees with the number required to control proliferative retinopathy. Reducing burn spacing or extending treatment up to the ora serrata allows application of sufficient burns to control the disease without encroaching on areas of the retina that provide the driving field.
Conclusion It is theoretically possible to alter the pattern of PRP to avoid treatment in retinal areas concerned with the driving visual field whilst leaving the total number of burns constant. This suggests that a clinical trial of such a pattern PRP could be performed to assess adequate control of proliferative retinopathy along with preservation of the visual field required for driving.
Similar content being viewed by others

Article PDF
References
The Diabetic Retinopathy Research Group. Photocoagulation treatment of proliferative diabetic retinopathy: the second report of diabetic retinopathy study findings. Ophthalmology 1978; 85: 82–106.
Frank RN . Visual fields and electroretinography following extensive photocoagulation. Arch Ophthalmol 1975; 93: 591–8.
Rogell GD . Incremental panretinal photocoagulation. Retina 1983; 3: 308–11.
Russell PW, Sekuler R, Fetkerhur C . Visual function after panretinal photocoagulation. Diabetes Care 1985; 8: 57–63.
Hamilton AM, Townsend C, Khoury D, Gould E, Blach RK . Xenon arc and argon laser photocoagulation in the treatment of diabetic disc neovascularisation. I. Effect on disc vessels, visual fields and visual acuity. Trans Ophthalmol Soc UK 1981; 101: 87–92.
Form CLE 1060. DVLC drivers medical branch, revised 1992.
Buckley SA, Jenkins L, Benjamin L . Fields, DVLC and panretinal photocoagulation. Eye 1992; 6: 623–6.
Hulbert MFG, Vernon SA . Passing the DVLC field regulations following bilateral panretinal photocoagulation in diabetics. Eye 1992; 6: 456–61.
Mackie SW, Webb LA, Hutchinson BM, Hammer HM, Barrie T, Walsh G . How much blame can be placed on laser photocoagulation for failure to attain driving standards? Eye 1995; 9: 517–25.
Pearson AR, Tanner V, Keightly SJ, Casswell AG . What effect does laser photocoagulation have on driving visual fields in diabetics? Eye 1998; 12: 64–8.
Blankenship GW . A clinical comparison of central and peripheral argon laser panretinal photocoagulation for proliferative diabetic retinopathy. Ophthalmology 1988; 95: 170–7.
Trick GL, Trick LR, Kilo C . Visual field defects in patients with insulin-dependent and non-insulin-dependent diabetes. Ophthalmology 1990; 97: 475–82.
Wisznia KI, Lieberman TW, Leopold IH . Visual fields in diabetic retinopathy. Br J Ophthalmol 1971; 55: 183–8.
Taylor E, Dobree JH . Proliferative diabetic retinopathy: site and size of initial lesions. Br J Ophthalmol 1970; 54: 11–8.
Taylor E, Jennings A . Calculation of total retinal area. Br J Ophthalmol 1971; 55: 262–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Davies, N. Altering the pattern of panretinal photocoagulation: Could the visual field for driving be preserved?. Eye 13, 531–536 (1999). https://doi.org/10.1038/eye.1999.132
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1038/eye.1999.132
